Intraocular foreign body management
Reading File
Finding Sources
Searching PubMed
"intraocular foreign body" management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
I have comprehensive, high-quality content from multiple authoritative sources. Here is the full structured answer:
Intraocular Foreign Body (IOFB) Management
Overview
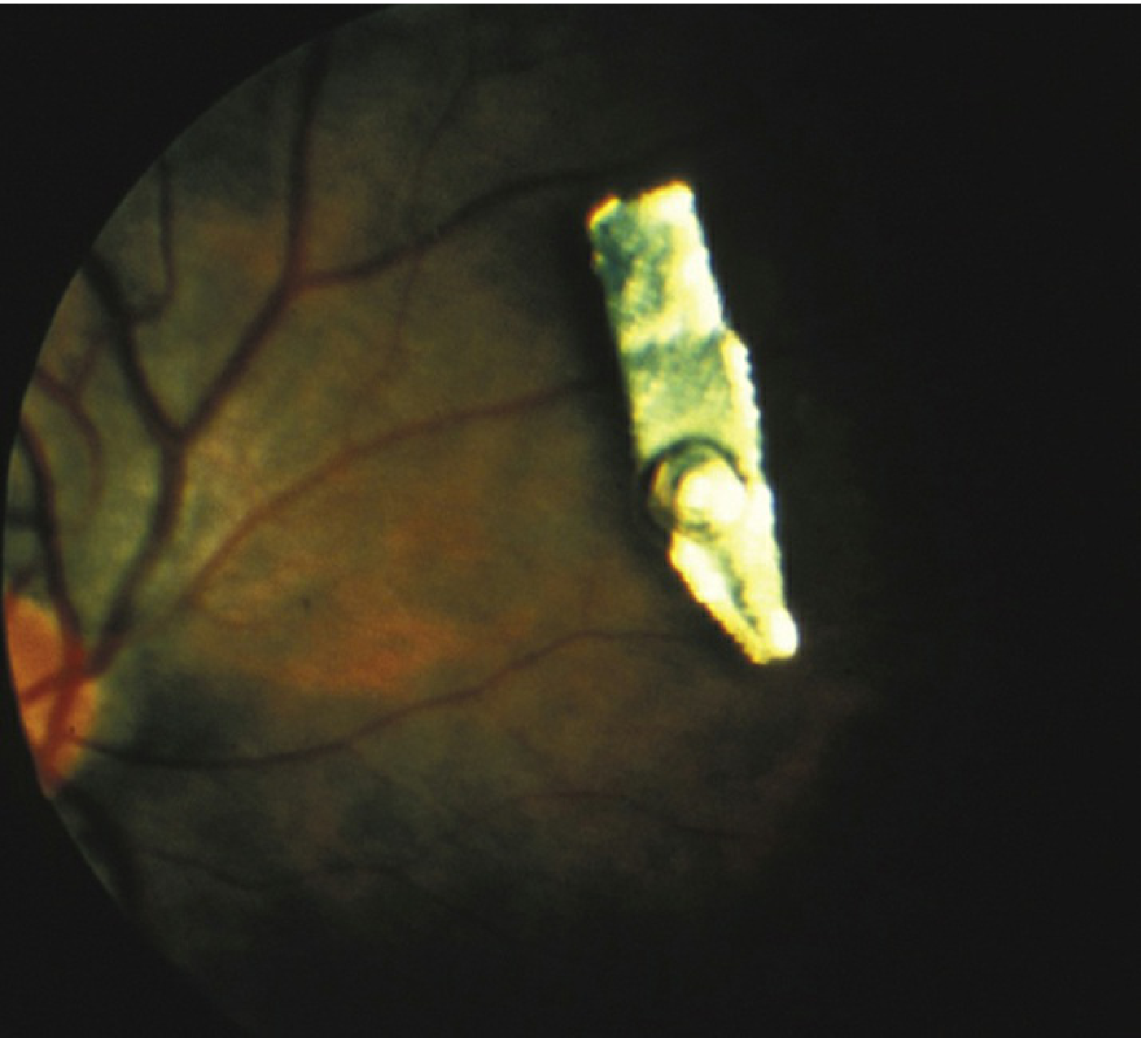
An IOFB may traumatize the eye mechanically, introduce infection, or exert toxic effects on intraocular structures. It can lodge in the anterior segment (AC, iris, lens) or posterior segment (vitreous, retina). Common mechanisms include hammering metal, power tool use, firearm/explosive injuries, and penetrating ocular trauma.
Presentation
Symptoms: Eye pain, decreased vision, or may be asymptomatic — a high index of suspicion is mandatory for any penetrating mechanism.
Signs:
- Clinically visible entry wound (corneal or scleral perforation), iris hole, focal lens opacity, or visible IOFB
- Irregular/teardrop-shaped pupil, hyphema, shallow/flat AC
- Microcystic corneal edema in the peripheral cornea (clue to AC angle foreign body)
- 360° subconjunctival hemorrhage, prolapse of uveal tissue
Classification of Foreign Bodies by Reactivity
| Category | Material | Reaction |
|---|---|---|
| Severe inflammatory / magnetic | Iron, steel, tin | Siderosis; high infection risk |
| Severe inflammatory / non-magnetic | Pure copper, vegetable matter | Endophthalmitis-like picture → phthisis |
| Mild inflammatory / magnetic | Nickel | Mild |
| Mild inflammatory / non-magnetic | Aluminum, mercury, zinc | Mild |
| Inert | Glass, gold, silver, lead, carbon, rubber, platinum, stone, brass | Minimal reaction |
Brass/bronze (copper alloy with low copper content) → chalcosis rather than violent endophthalmitis. Most BBs and gunshot pellets contain 80–90% lead + 10–20% iron.
Workup
History
- Nature and composition of the foreign body
- Mechanism (hammering, grinding, blast)
- Time of last meal (surgical planning)
Examination
Examine with minimal manipulation — if an open globe is suspected, stop the exam and place a rigid protective shield (no patching).
- Visual acuity
- Slit lamp: Entry sites, iris TID (transillumination defects), pupil shape, lens disruption, hyphema, AC depth, IOP
- Gonioscopy if no wound leak and globe appears intact (to locate AC angle FB)
- Dilated indirect ophthalmoscopy — deferred if risk of extrusion of intraocular contents
- CT orbits (axial + coronal + parasagittal, ≤1-mm sections) — preferred imaging; sensitivity superior to plain X-ray and ultrasound for metallic IOFBs
- B-scan ultrasound / UBM — useful for non-metallic foreign bodies and when CT is equivocal; intraocular air can mimic a foreign body
- MRI is contraindicated in the setting of any metallic (especially ferrous) IOFB
Immediate Emergency Management
- NPO — no food or drink until surgical repair
- Rigid protective shield over the eye (do not patch)
- Tetanus prophylaxis (see tetanus schedule)
- Systemic broad-spectrum antibiotics covering gram-positive and gram-negative organisms:
- Vancomycin 1 g IV q12h + ceftazidime 1 g IV q12h
- OR ciprofloxacin 400 mg IV q12h
- OR moxifloxacin 400 mg IV daily
- (Fluoroquinolones contraindicated in children and pregnant women)
- Cycloplegia (e.g., atropine 1% b.i.d.) for posterior-segment IOFBs
- Emergent ophthalmology consultation — any further examination to be performed only in the OR
Surgical Removal
Urgent removal of any acute IOFB is advisable to reduce infection risk and proliferative vitreoretinopathy (PVR).
Magnetic (Ferrous) IOFBs
- Magnetic extraction via sclerotomy adjacent to the foreign body, using an intraocular magnet, followed by cryotherapy to seal any retinal break created
- This is the preferred approach for ferro-magnetic bodies that can be safely reached
Non-Magnetic (or Inaccessible Magnetic) IOFBs
- Pars plana vitrectomy (PPV) with forceps extraction — the IOFB is removed either through the pars plana or the limbus depending on location and size
Special Situations
- Copper/contaminated foreign bodies require especially urgent removal
- Chronic IOFB may be observed if inert, but requires removal if associated with severe recurrent inflammation, location in the visual axis, or evidence of siderosis
- Inert foreign bodies (glass, gold, etc.) are often well tolerated; surgical removal risk must be weighed against the risk of delayed complications
Complications
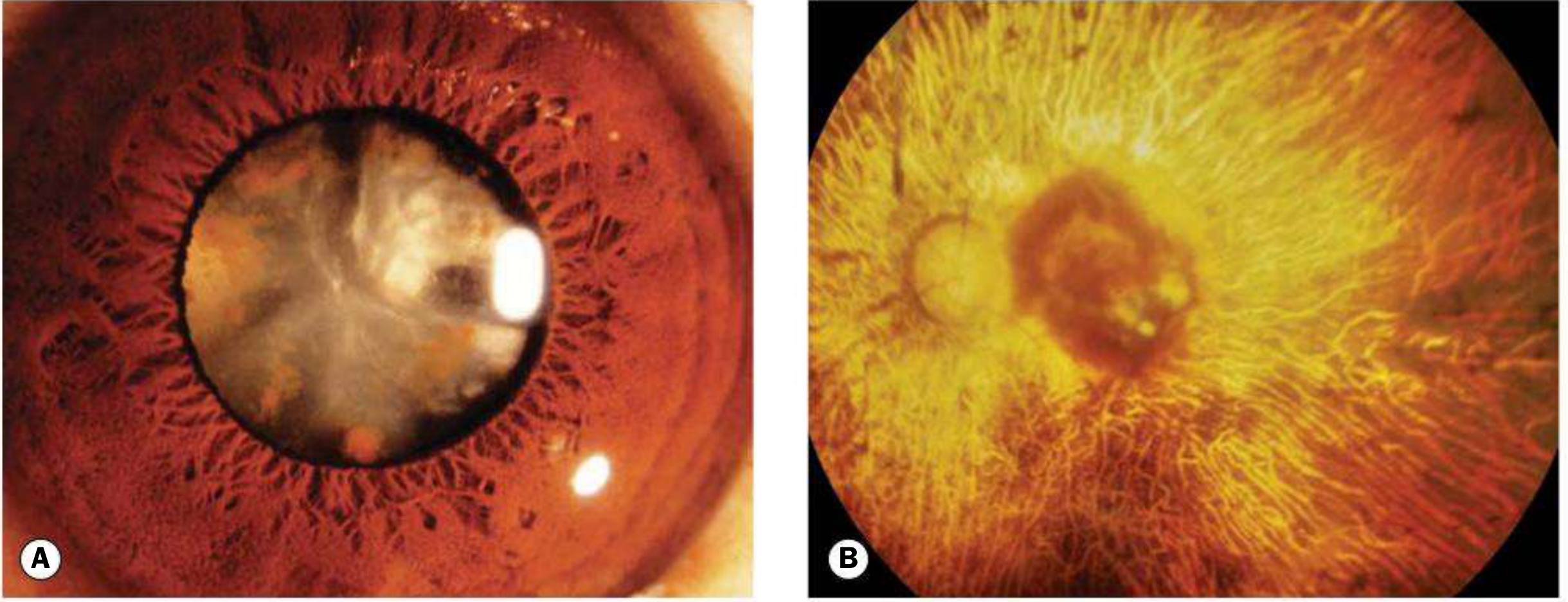
Siderosis Bulbi (Iron/Steel)
Iron dissociates and deposits in intraocular epithelial structures (lens epithelium, iris and ciliary body epithelium, sensory retina), exerting toxic effects on cellular enzyme systems.
Signs:
- Anterior subcapsular cataract (radial iron deposits on anterior lens capsule)
- Reddish-brown iris staining → heterochromia iridis
- Pigmentary retinopathy → RPE atrophy → profound visual loss
- Trabecular damage → secondary glaucoma
- Anisocoria, lens dislocation, optic atrophy
- ERG: Progressive attenuation of the b-wave — a key monitoring tool
Chalcosis (Copper Alloy)
- Copper alloy (brass/bronze) → electrolytic dissociation → copper deposition
- Kayser–Fleischer ring, anterior sunflower cataract, retinal golden plaques
- Less retinotoxic than iron — degenerative retinopathy usually does not develop
Endophthalmitis
- Develops in ~1 in 10 cases of penetrating trauma with retained IOFB
- Risk factors: Delay in primary repair, retained IOFB, wound position/extent
- Pathogens: Staphylococcus spp. and Bacillus spp. account for ~90% of culture-positive cases
- Management: Prompt IOFB removal + prophylactic intravitreal antibiotics (especially for high-risk cases such as agricultural injuries); treat established endophthalmitis as for acute postoperative endophthalmitis
- Culture the removed IOFB
Proliferative Vitreoretinopathy (PVR)
A reason for urgent removal — delayed surgery increases PVR risk.
Sympathetic Ophthalmia
- Vision-threatening autoimmune response to the fellow (uninjured) eye
- Triggered by exposure of the immune system to intraocular contents from the perforated eye
- Rare but devastating; another argument for prompt primary repair
Follow-Up
- Observe closely for signs of inflammation or infection post-repair
- If uncertain whether FB was fully removed, perform post-op CT/B-scan/UBM
- Serial ERGs to monitor for toxic retinopathy when an IOFB is retained — retinopathy often reverses if the FB is removed before severe damage
- Long-term periodic follow-up for years (watch for delayed inflammatory reactions in both the traumatized and fellow eye)
Recent Evidence
A 2025 systematic review and meta-analysis (McMaster et al., Ophthalmology 2025; PMID 39218161) addressed timing of primary repair after open-globe injury. This is relevant context — current evidence supports early primary repair in open-globe injuries including those with retained IOFB.
Sources: Kanski's Clinical Ophthalmology 10th ed., p. 942–943 | Wills Eye Manual 7th ed., pp. 142–147 | Rosen's Emergency Medicine 10th ed.
Fundus florescent angiography
Reading File
Finding Sources
Searching PubMed
"fluorescein angiography" fundus technique interpretation
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have rich, comprehensive content from both Kanski's and the Wills Eye Manual. Let me compile the definitive answer:
Fundus Fluorescein Angiography (FFA / FA)
Principle
Fluorescence is the property of certain molecules to emit light of a longer wavelength when excited by light of a shorter wavelength. Sodium fluorescein:
- Excitation peak: ~465–490 nm (blue light)
- Emission peak: ~520–530 nm (yellow-green light)
Sodium fluorescein is an orange, water-soluble dye. When injected IV, >70–80% is protein-bound and does not cross healthy blood–retinal barriers. The free (unbound) fraction is small but responsible for pathological leakage. Excreted in urine over 24–36 hours (urine turns bright yellow — warn all patients).
Blood–Retinal Barrier Anatomy (Critical to FA Interpretation)
| Barrier | Location | Normal permeability to fluorescein |
|---|---|---|
| Inner BRB | Tight junctions between retinal capillary endothelial cells | Impermeable to bound AND free fluorescein |
| Outer BRB | RPE tight junctions (zonula occludentes) + Bruch membrane | RPE impermeable; choriocapillaris freely permeable (fenestrated) |
Disruption of either barrier → leakage of fluorescein into extravascular space → hyperfluorescence.
Camera Setup & Filters
- Cobalt blue excitation filter: Passes only blue light into the eye (~490 nm) to excite fluorescein
- Yellow-green barrier filter: Blocks reflected blue light, allowing only emitted yellow-green fluorescence to reach the sensor
- Modern digital CCD cameras allow immediate image availability, lower fluorescein doses, and enhanced image manipulation — with correspondingly lower adverse effect rates
Technique
- Adequate pharmacological mydriasis is essential
- Baseline colour photographs + red-free images (green incident light to enhance red detail) + autofluorescence images taken first
- IV cannula inserted (standard cannula preferred over butterfly); flush with normal saline to confirm patency
- 5 ml of 10% sodium fluorescein injected over 5–10 seconds
- Photography begins 5–10 seconds after injection at 1–2 second intervals to capture the critical early transit phases
- Images continue into the late phase (10–20 minutes)
- Oral alternative (if IV access not possible): 30 mg/kg, images taken 20–60 minutes after ingestion
- Stereo images may demonstrate elevation (e.g., neovascular membranes)
Phases of FA
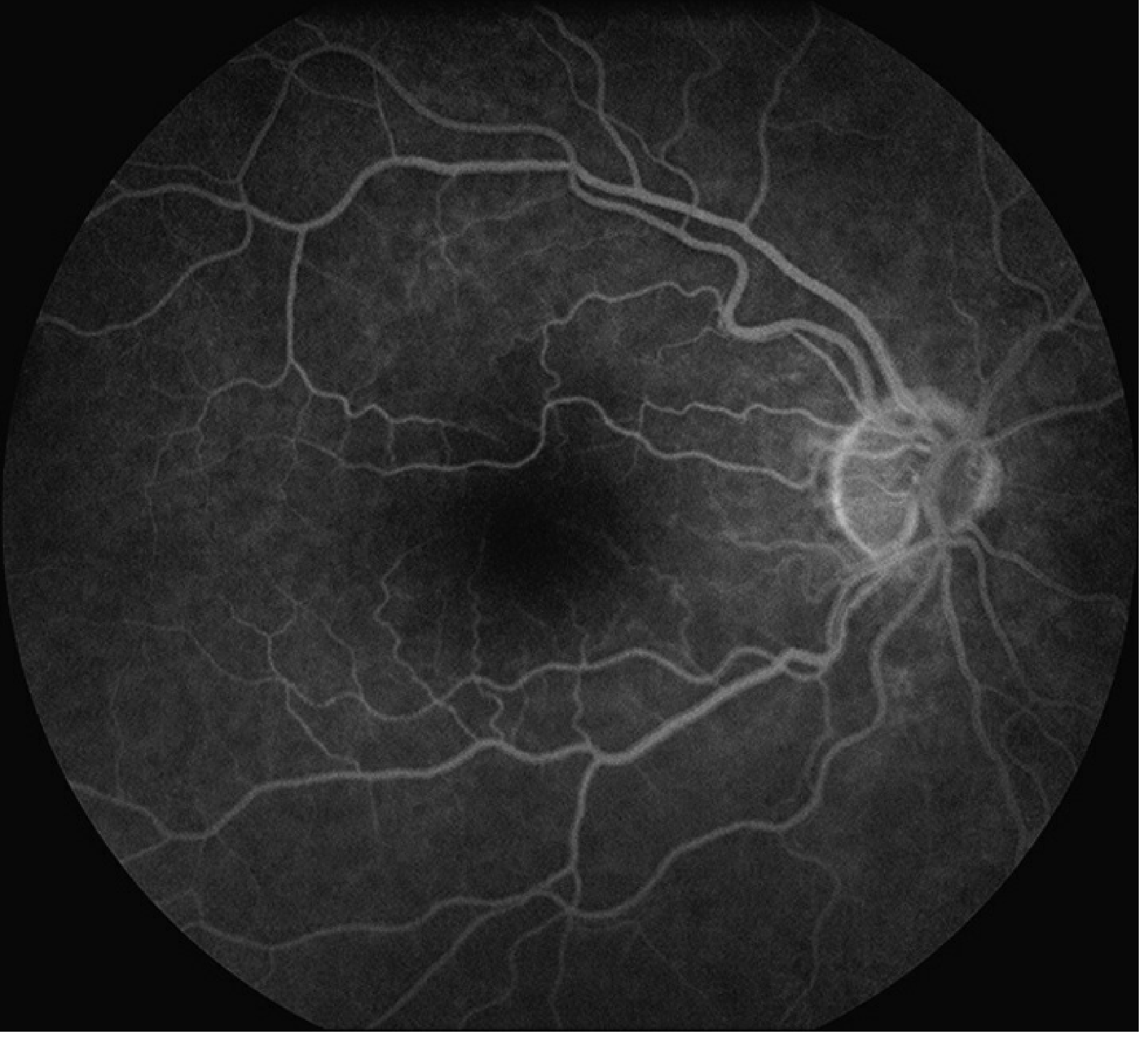
| Phase | Timing | Features |
|---|---|---|
| Pre-arterial / Choroidal | 8–15 sec after injection | Patchy background choroidal fluorescence (choriocapillaris fills first); complete within 5 sec of first appearance |
| Arterial | 1–2 sec after choroidal filling | Retinal arteries fill; arterioles fill centrifugally |
| Arteriovenous (laminar flow) | Overlaps arterial/venous | Laminar flow visible in veins — bright margins, dark centre |
| Venous | A-V transit time normally <11 sec | Veins fill completely; arteries begin to fade |
| Recirculation | 45–60 sec after arterial phase | Dye recirculates; fluorescence diminishes |
| Late phase | 10–30 min post-injection | Normal vessels fade; any persistent fluorescence = leakage or staining |
Foveal dark spot: Results from xanthophyll pigment in the outer plexiform layer and tall, densely pigmented RPE cells. The foveal avascular zone (FAZ) is 300–500 µm in diameter with no retinal capillaries.
Interpreting the Abnormal Study
HYPERFLUORESCENCE (Increased signal)
| Pattern | Mechanism | Characteristics | Examples |
|---|---|---|---|
| Leakage | Breakdown of inner or outer BRB → fluorescein exits vessels | Increases in both size AND brightness over time | CNV, CME, CSCR (subretinal leak), diabetic macular edema, retinal neovascularization |
| Pooling | Fluorescein accumulates in anatomical fluid space | Fixed borders; increases in brightness but not size (sub-RPE pooling) or slow expansion (subretinal) | PED (sub-RPE), CSCR (subretinal space) |
| Staining | Fluorescein absorbed by abnormal tissue | Mild, late-phase fluorescence; borders remain fixed | Scar, drusen, disciform scar |
| Window/Transmission defect | RPE atrophy unmasks background choroidal fluorescence | Early hyperfluorescence, fixed in size, fades in late phase (does not grow) | Geographic atrophy, RPE rip, macular hole, laser scar |
| Autofluorescence | Intrinsically fluorescent structures visible before injection | Detected on pre-injection images | Optic disc drusen, astrocytic hamartoma, lipofuscin |
Key differentiator: Leakage = grows in size AND brightness. Pooling = grows in brightness only (fixed border). Window defect = fades in late phase, does not grow.
HYPOFLUORESCENCE (Reduced signal)
| Pattern | Mechanism | Examples |
|---|---|---|
| Blockage (masking) | Opaque material between camera and fluorescein obscures signal | Hemorrhage (pre-, intra-, sub-retinal), pigment, fibrous tissue, exudate |
| Non-perfusion (vascular filling defect) | Absent blood flow → no fluorescein delivery | Central/branch retinal artery occlusion, capillary non-perfusion in diabetic retinopathy, ischemic CRVO |
Clinical Indications
- Retinal vascular disease — diabetic retinopathy (capillary non-perfusion, neovascularization), CRVO, BRVO, CRAO
- Choroidal neovascularization (CNV) — AMD (classic vs occult), pathologic myopia, angioid streaks
- Macular disease — CSCR, CME, macular degeneration, macular hole
- Optic disc evaluation — disc swelling, drusen, ischemic optic neuropathy
- Iris vasculature — rubeosis iridis
- Transit time analysis — arm-to-retina time, arteriovenous transit time; useful in ocular ischemic syndrome
- Treatment planning — identify targets for laser photocoagulation or anti-VEGF therapy
FA should only be performed if the findings are likely to influence management. — Kanski's
Adverse Effects
| Effect | Frequency |
|---|---|
| Skin + urine discolouration (yellow) | Invariable |
| Nausea/vomiting | Nausea ~10%, vomiting ~2% (lower with modern low-dose technique) |
| Pruritus, urticaria, rash | Uncommon |
| Vasovagal episode | Uncommon |
| Extravasation at injection site (local necrosis) | Treat with cold compresses |
| Anaphylaxis | ~1 in 2,000 |
| Myocardial infarction | Extremely rare |
| Death | ~1 in 220,000 |
Emergency preparation is mandatory: Resuscitation equipment, adrenaline, reclining couch, and trained staff must be present.
Contraindications
| Type | Contraindication |
|---|---|
| Absolute | Known fluorescein allergy |
| Relative | History of severe reaction to any allergen, renal failure (reduce dose), pregnancy, moderate–severe asthma, significant cardiac disease |
| Not a contraindication | Iodine/shellfish allergy (iodine is relevant only for ICG angiography, not FA) |
Comparison with ICG Angiography (ICGA)
| Feature | FA | ICGA |
|---|---|---|
| Dye | Sodium fluorescein | Indocyanine green (iodine-based) |
| Excitation / Emission | 465–490 nm / 520–530 nm | 805 nm / 835 nm (infrared) |
| Protein binding | ~80% | ~95% |
| Penetration | Retinal circulation best | Choroidal circulation (penetrates pigment, fluid, blood) |
| Key indication | Retinal vasculature, CNV, macular disease | Occult CNV, polypoidal choroidal vasculopathy (PCV), choroidal disease |
| Contraindication | Fluorescein allergy | Iodine/shellfish allergy, liver disease (hepatic excretion) |
| Fluorescence intensity | High | 1/25th of FA — requires high-sensitivity camera |
Sources: Kanski's Clinical Ophthalmology 10th ed., pp. 583–591 | Wills Eye Manual 7th ed., pp. 1100–1103
This is a shared conversation. Sign in to Orris to start your own chat.