Reason of ear nerve dryness and decreased hearing
Reading File
Finding Sources
Finding Sources
Searching PubMed
"sensorineural hearing loss"[MeSH Terms] AND causes
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have thorough textbook coverage. Let me compile a comprehensive answer.
Causes of Auditory Nerve / Cochlear Damage and Decreased Hearing
The term "ear nerve dryness" is not a formal medical term, but it most accurately describes sensorineural hearing loss (SNHL) — hearing loss arising from damage to the hair cells of the cochlea, the auditory (cochlear) nerve itself, or the central auditory pathways. Here is a full breakdown of causes, organized by mechanism.
What Goes Wrong?
Sensorineural hearing loss results from either:
- Damage to the mechanotransduction apparatus of the cochlea (hair cells, supporting cells), or
- Disruption of the electrical conduction pathway from the inner ear to the brain (auditory neurons, central auditory pathway)
— Harrison's Principles of Internal Medicine 22E
Major Causes
1. Age-Related Degeneration (Presbycusis) — Most Common
Presbycusis is the most common cause of SNHL in adults, affecting over half of adults aged >75 years. It is not a single disease but the cumulative effect of aging on the auditory system. The most consistent pathological finding is degeneration of sensory cells and nerve fibers at the base of the cochlea, causing symmetrical, high-frequency hearing loss that gradually worsens. It is also associated with loss of clarity, difficulty understanding speech in noisy environments, and cognitive decline if untreated.
— Goldman-Cecil Medicine; Harrison's 22E
2. Noise-Induced Hearing Loss
Exposure to loud noise — whether a single intense burst or prolonged — damages hair cells and auditory nerve synapses. Key features:
- Permanent threshold shifts occur with sufficient intensity/duration
- Typically shows a "noise notch" with elevated thresholds at 4000–5000 Hz
- Cochlear synaptopathy ("hidden hearing loss"): noise destroys auditory synapses on hair cells even when routine audiometry appears normal — patients complain of difficulty hearing in background noise — Harrison's 22E; Goldman-Cecil
3. Ototoxic Medications
Several drug classes directly destroy cochlear hair cells and spiral ganglion neurons:
| Drug Class | Examples |
|---|---|
| Aminoglycoside antibiotics | Gentamicin, streptomycin, neomycin |
| Loop diuretics | Furosemide, ethacrynic acid |
| Platinum chemotherapy | Cisplatin, carboplatin |
| Antimalarials / salicylates | Quinine, high-dose aspirin |
| Opioids (abuse) | Hydrocodone |
Aminoglycosides cause irreversible, bilateral, high-frequency hearing loss through accumulation in perilymph/endolymph and degeneration of hair cells and cochlear neurons.
— Harrison's 22E; Goodman & Gilman's
4. Viral Infections / Labyrinthitis
Viral infections of the labyrinth directly damage cochlear hair cells and auditory neurons. Causes include:
- Mumps, measles, cytomegalovirus (CMV), herpes zoster (Ramsay Hunt syndrome)
- Sudden sensorineural hearing loss (SSNHL) is often presumed viral
5. Ménière's Disease (Endolymphatic Hydrops)
Characterized by episodic vertigo, fluctuating sensorineural hearing loss, tinnitus, and aural fullness. Caused by abnormal accumulation of endolymph in the inner ear, distorting the membranous labyrinth and disrupting hair cell function.
— Harrison's 22E
6. Acoustic Neuroma (Vestibular Schwannoma)
A benign tumor of the cerebellopontine angle that progressively compresses the auditory nerve. Causes insidious, progressive unilateral hearing loss, initially in the high frequencies. Diagnosed by MRI with contrast.
— Goldman-Cecil
7. Auditory Neuropathy
A distinct condition where the cochlear nerve itself is dysfunctional despite preserved outer hair cell function (OAEs present, ABRs absent/abnormal). Causes include:
- Genetic mutations: OPA1 gene (optic atrophy protein in mitochondria of spiral ganglion cells), ATP1A3, SPTBN4, WBP2
- Defects in myelin sheath of the auditory nerve (e.g., Charcot-Marie-Tooth syndrome types 1A/1B)
- Oxidative stress damaging auditory nerve terminals
- Ion channel disruption (abnormal K⁺ channel distribution along nerve axons) — Cummings Otolaryngology
8. Genetic / Hereditary Causes
- Connexin 26 (GJB2) mutations — most common cause of recessively inherited deafness; affects gap junctions essential for K⁺ recycling in the cochlea
- Other syndromic conditions (CAPOS syndrome, Usher syndrome, Waardenburg syndrome)
- Congenital inner ear malformations — Goldman-Cecil; Cummings
9. Vascular / Ischemic Causes
- Occlusion of the anterior inferior cerebellar artery (AICA) — supplies the inner ear; occlusion causes sudden unilateral deafness + vestibular loss
- Stroke affecting brainstem cochlear nuclei — Goldman-Cecil
10. Trauma
- Fracture of the temporal bone — directly tears the cochlea or auditory nerve
- Head trauma with hemorrhage into the cochlea — Harrison's 22E
11. Autoimmune & Inflammatory
- Meningitis — bacterial infection that spreads to the cochlea and damages hair cells/nerves; a major cause of acquired deafness
- Multiple sclerosis — demyelination of central auditory pathways
- Cochlear otosclerosis — new bone invades the cochlea — Harrison's 22E
12. Radiation Therapy
Radiation to the head/neck can damage the cochlea and auditory nerve, causing progressive SNHL.
Summary Table
| Category | Mechanism | Key Features |
|---|---|---|
| Presbycusis | Hair cell & nerve fiber degeneration | Bilateral, high-frequency, age-related |
| Noise | Hair cell death + synaptic loss | 4000 Hz notch, hidden hearing loss |
| Ototoxic drugs | Hair cell & neuron destruction | Bilateral, often irreversible |
| Viral labyrinthitis | Direct infection | Often sudden, unilateral |
| Ménière's disease | Endolymphatic hydrops | Fluctuating, + vertigo + tinnitus |
| Acoustic neuroma | Nerve compression | Progressive, unilateral |
| Auditory neuropathy | Nerve fiber / synapse dysfunction | OAEs preserved, abnormal ABR |
| Genetic | Connexin 26, other mutations | Congenital or early-onset |
| Vascular | AICA occlusion, stroke | Sudden, unilateral |
| Trauma | Cochlear/nerve disruption | Temporal bone fracture |
| Meningitis/MS | Infection or demyelination | Often bilateral (meningitis) |
Key point: Most sensorineural hearing loss involves either physical destruction of delicate cochlear hair cells (which do not regenerate in humans) or degeneration of the spiral ganglion neurons that form the auditory nerve. Prevention (noise protection, avoiding ototoxic drugs when possible) is critical, as the damage is typically irreversible. Cochlear implants are the treatment of choice when hearing aids are insufficient.
Age is 43 and also complain of very high noice in some time in ear like noice pollution voice like
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Excellent — comprehensive information gathered. Now I can give a focused, clinically relevant answer.
Tinnitus + Decreased Hearing at Age 43 — Clinical Analysis
The combination of loud roaring/noise-pollution-like sound in the ear (tinnitus) with decreased hearing at age 43 is a very specific clinical picture. Here is what it means and the most likely causes.
What is the Noise (Tinnitus)?
The loud sound the patient hears internally — like noise pollution, roaring, or rushing — is called tinnitus. It is not an external sound; it is generated by the auditory system itself when it is damaged or disturbed. It is almost always a signal that something is wrong with the ear or auditory nerve.
"Tinnitus is most often subjective (heard only by the patient). In most cases, tinnitus is secondary to bilateral sensorineural hearing loss." — Textbook of Family Medicine 9e
Most Likely Diagnoses at Age 43
🔴 1. Ménière's Disease — Top Priority to Rule Out
This is the most important condition to consider given this exact combination at this age.
Classic triad:
- Episodic loud roaring tinnitus (described as "like listening to a seashell")
- Fluctuating sensorineural hearing loss (comes and goes)
- Episodes of vertigo (spinning sensation)
- Aural fullness (blocked/pressure sensation in the ear)
Ménière's disease onset is most frequently in the fifth decade of life (40s–50s) — this patient's age fits perfectly. It is caused by endolymphatic hydrops — abnormal buildup of fluid in the inner ear that distorts and damages cochlear hair cells and vestibular structures.
"Onset is most frequently in the fifth decade of life but may also occur in young adults." — Harrison's Principles of Internal Medicine 22E
Important: If the patient has no vertigo, the condition may be cochlear hydrops (same mechanism, cochlea only).
🟠 2. Noise-Induced Hearing Loss (NIHL)
If the patient has had occupational noise exposure (factory, machinery, loud music, firearms), this is a leading cause at age 43:
- Damages hair cells at the base of the cochlea
- Causes tinnitus that is often high-pitched ringing or hissing
- Begins at 4000 Hz on audiogram
- "Hidden hearing loss" — cochlear synaptopathy can cause tinnitus even when routine hearing test appears normal — Harrison's 22E; Goldman-Cecil
🟠 3. Sudden Sensorineural Hearing Loss (SSNHL)
If the hearing loss came on abruptly (over hours to days) with tinnitus, this is a medical emergency requiring urgent treatment:
- Presumed viral or vascular cause
- Requires immediate high-dose steroids (oral or intratympanic)
- MRI needed to exclude acoustic neuroma — Bailey & Love's Surgery 28E
🟡 4. Acoustic Neuroma (Vestibular Schwannoma)
A benign tumor on the auditory/vestibular nerve:
- Causes progressive unilateral hearing loss + high-pitched tinnitus ("like steam from a kettle")
- Begins insidiously in high frequencies
- Must be excluded by MRI in any patient with unilateral hearing loss + tinnitus — Goldman-Cecil
🟡 5. Ototoxic Medications
If the patient is taking any of these, they could be the direct cause:
| Medication | Effect |
|---|---|
| Aspirin / NSAIDs | Tinnitus + reversible hearing loss |
| Aminoglycoside antibiotics | Irreversible hair cell destruction |
| Loop diuretics (furosemide) | Cochlear damage |
| Quinine / antimalarials | Tinnitus + SNHL |
| Oral contraceptives | Listed as tinnitus cause |
— Textbook of Family Medicine 9e
🟡 6. Metabolic Causes
Systemic conditions that alter blood flow or nerve function near the cochlea:
- Hyperthyroidism / Hypothyroidism — increase/decrease cochlear blood flow
- Hyperlipidemia — reduces cochlear microvascular supply
- Vitamin B12 / folate deficiency — nerve demyelination
- Diabetes mellitus — cochlear microangiopathy and auditory neuropathy
- Hypertension — pulsatile tinnitus, cochlear ischemia
🟡 7. Temporomandibular Joint (TMJ) Dysfunction
The TMJ is anatomically close to the ear. Jaw clenching, grinding, or joint misalignment can cause referred tinnitus in one or both ears — surprisingly common and often overlooked.
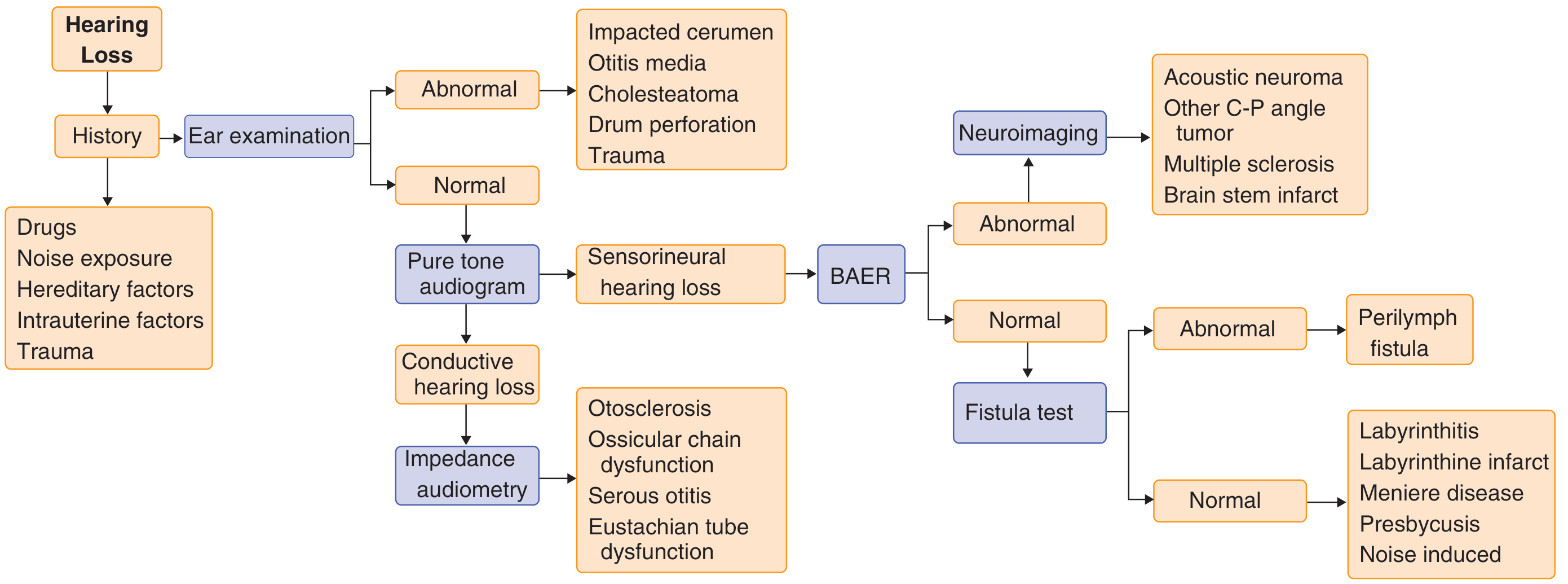
Diagnostic Flowchart (from Goldman-Cecil Medicine)
Red Flags — Seek Urgent Evaluation If:
| Sign | Concern |
|---|---|
| Unilateral tinnitus + hearing loss | Acoustic neuroma — needs MRI |
| Sudden hearing loss (hours/days) | SSNHL — needs steroids urgently |
| Pulsatile tinnitus (beats with heartbeat) | Vascular tumor or aneurysm — needs MRA |
| Tinnitus + vertigo + vomiting | Ménière's disease or labyrinthitis |
| Headache + vision changes | Intracranial mass |
What Should This 43-Year-Old Do?
- See an ENT specialist (Otolaryngologist) — this is the priority
- Pure tone audiogram — identifies type and pattern of hearing loss
- MRI with contrast — to exclude acoustic neuroma or other retrocochlear pathology
- Blood tests: thyroid function, lipid panel, fasting glucose, CBC, B12/folate, inflammatory markers
- Review all medications for ototoxic potential
- History: noise exposure at work? Vertigo episodes? Ear fullness? Family history of hearing loss?
Practical Advice While Awaiting Evaluation
- Avoid loud noise exposure (use earplugs if needed)
- Stop/reduce caffeine and nicotine — both worsen tinnitus
- Reduce salt intake — helps if Ménière's disease is the cause
- Do not ignore this — tinnitus + hearing loss at 43 has treatable causes if caught early
This is a shared conversation. Sign in to Orris to start your own chat.