All i need to know about supracondylar fracture
Reading File
Finding Sources
Searching the Web
supracondylar fracture humerus classification management complications
Searching PubMed
"supracondylar fracture" AND humerus
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Supracondylar Fracture of the Humerus
Overview
Supracondylar humeral fractures are transverse fractures of the distal humerus just above the level of the epicondyles, occurring in the thin metaphyseal region between the olecranon fossa and coronoid fossa. They are the most common elbow fracture in children, occurring at a rate of 60-70 per 100,000 children in the US. The peak age is 4-6 years (mean 5.5 years), with 52% occurring in males, and 98% are extension-type injuries.
- Campbell's Operative Orthopaedics 15th Ed 2026
- Bailey and Love's Short Practice of Surgery 28th Edition
Mechanism of Injury
Extension type (98%) - Fall on an outstretched hand (FOOSH) with the elbow hyperextended. The distal fragment displaces posteriorly, with the triceps muscle bowstringing the brachial artery over the sharp proximal fracture fragment. The distal fragment characteristically displaces backwards, upwards, and slightly internally rotated (forearm usually pronated at the time of injury).
Flexion type (2%) - Fall on a stretched, fully extended elbow driving the lower fragment forward. These are rarer, harder to reduce, have worse outcomes, and are associated with ulnar nerve injury.
- Gray's Anatomy for Students
- S Das Manual on Clinical Surgery 13th Edition
Classification - Modified Gartland (Most Used)
| Type | Description | Stability |
|---|---|---|
| I | No/minimal displacement; posterior fat pad may be only sign | Stable |
| IIA | Displaced, posterior cortex intact, no rotational component | Stable |
| IIB | Displaced, posterior cortex intact, with rotational component | Unstable |
| III | Complete displacement, no cortical contact; may be posteromedial or posterolateral | Unstable |
| IV | Complete circumferential periosteal disruption; multidirectionally unstable (usually high-energy) | Very unstable |
- Rosen's Emergency Medicine | Campbell's Operative Orthopaedics 15th Ed 2026
Clinical Features
Symptoms:
- Pain, gross swelling at the elbow
- Child holds the arm supported with the other hand
- Bruising (may be delayed)
Signs:
- Posterior prominence of the elbow (must differentiate from posterior dislocation)
- Loss of carrying angle
- Tenderness over distal humerus
- Restricted, painful movements
Key difference from posterior dislocation: In supracondylar fracture, the relationship between olecranon and epicondyles is preserved (normal equilateral triangle); in posterior dislocation, this triangle is disrupted.
- S Das Manual on Clinical Surgery 13th Edition
Radiological Assessment
Views needed: AP + lateral of the elbow. Comparison views of the uninjured side are helpful in children.
Five key radiographic signs:
| Finding | Significance |
|---|---|
| Anterior humeral line does not bisect the middle third of capitellum on lateral view | Suggests extension-type supracondylar fracture (capitellum sits posterior) |
| Baumann's angle (intersection of humeral shaft axis with lateral condyle physis on AP) - normal ~75° | Abnormal angle = inadequate reduction |
| Posterior fat pad sign | Strongly suggests occult fracture (76% rate of fracture even without other abnormality) |
| Long axis of ulna not in line with humerus | Possible supracondylar or transphyseal injury |
| Radius does not point to capitellum | Lateral condyle fracture, radial neck fracture, Monteggia, or elbow dislocation |
CRITOE mnemonic - Order of ossification centers (important to avoid misidentifying as fractures):
| Center | Age of Appearance |
|---|---|
| Capitellum | 1-2 years |
| Radial head | 4-5 years |
| Internal (medial) epicondyle | 4-5 years |
| Trochlea | 8-10 years |
| Olecranon | 8-9 years |
| External (lateral) epicondyle | 10-11 years |
- Rosen's Emergency Medicine | Miller's Review of Orthopaedics 9th Edition
Neurovascular Assessment (Critical)
Neurological injury occurs in 10-15% of cases. Must test ALL three nerves:
| Nerve | Type Injured | Test |
|---|---|---|
| Anterior interosseous nerve (AIN) | Most common in extension-type | "OK" sign - pinch thumb and index fingertip; AIN injury = flat pinch |
| Radial nerve | Extension-type | Wrist/finger extension |
| Ulnar nerve | Most common in flexion-type (10%) | Intrinsic hand muscles, sensation little finger |
| Median nerve | Less common | Sensation, thenar muscles |
Most nerve injuries are neuropraxia and resolve within 6-12 weeks following fracture reduction. Loss of nerve function after reduction is a red flag for nerve entrapment - requires urgent open exploration. EMG is indicated if no recovery within 3 months.
Vascular injury to the brachial artery occurs in up to 10-20% of type III fractures. Two scenarios exist:
Vascular Injury Management Algorithm
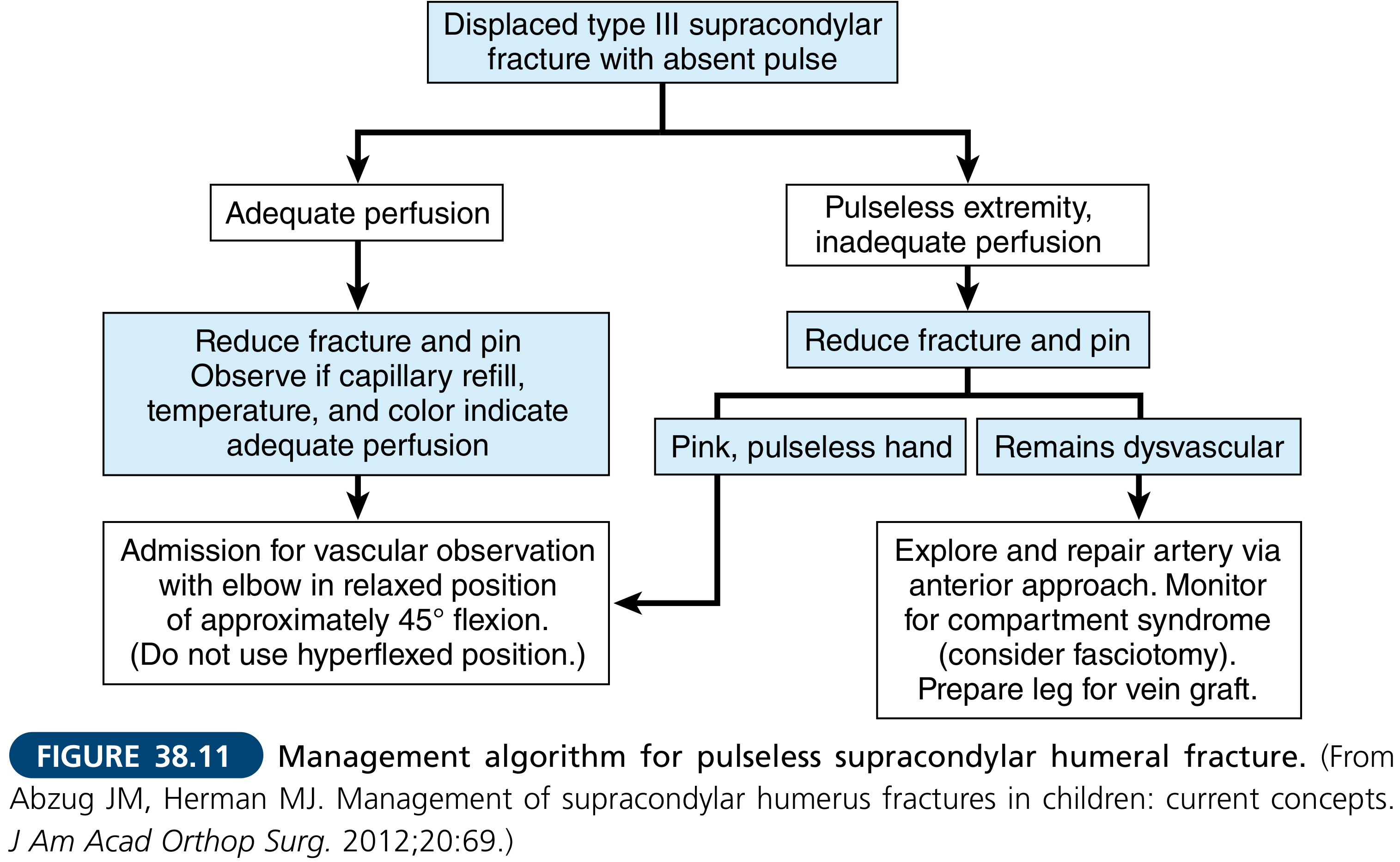
White (pale) pulseless hand: Surgical emergency. Immediate reduction; if pulse does not return, urgent vascular exploration by appropriately trained surgeons.
Pink pulseless hand (controversial): If satisfactory perfusion, no compartment syndrome, and no neurological injury - reduce and stabilize the fracture first. Observe for 24-48 hours as pulse often returns. If hand becomes poorly perfused, obtain vascular consultation.
- Campbell's Operative Orthopaedics 15th Ed 2026 | Bailey and Love's Short Practice of Surgery
Treatment
Type I (Nondisplaced)
- Long-arm cast or backslab in 75-80 degrees of flexion, forearm neutral rotation
- Duration: 3 weeks, then protected range-of-motion
- Even without radiographic findings, a child with localized tenderness should be splinted and followed up in 24-48 hours
- Can be safely discharged from ED with elevation, ice, and follow-up in 1-2 days
Type IIA (Stable, no rotation)
- Closed reduction and casting
- Above-elbow cast for 3-4 weeks if dorsal periosteal hinge is intact
Type IIB (Unstable, rotation present)
- Closed reduction and percutaneous pinning (CRPP) with 2-3 lateral pins
- Post-op long-arm immobilization at 90 degrees flexion
Type III (Complete displacement)
- CRPP is the preferred treatment
- Key: avoid tearing posterior soft tissues during reduction (which would create a type IV injury)
Type IV (High-energy, multidirectionally unstable)
- CRPP (if periosteal hinge is broken, K-wires are essential)
- Important: do NOT place elbow in deep flexion if significant swelling - use K-wire fixation instead (to prevent Volkmann's ischemia from compartment syndrome)
ORIF (Open Reduction and Internal Fixation) - Rarely needed
Indications: rotationally unstable fractures, open fractures, fractures associated with neurovascular injuries. Anterior approach is preferred.
Pin Configuration Debate:
-
Lateral-entry pins only - fewer complications (avoids ulnar nerve), shown to be as stable as crossed pins when adequate pin spread is achieved. Divergent technique is recommended.
-
Crossed pins (lateral + medial) - historically considered more stable biomechanically, but medial pin carries 3-8% risk of iatrogenic ulnar nerve injury
-
Campbell's Operative Orthopaedics 15th Ed 2026 | Miller's Review of Orthopaedics 9th Edition | Bailey and Love's Short Practice of Surgery
Complications
Early
| Complication | Details |
|---|---|
| Vascular injury | Brachial artery injury in 10-20% of Type III; "pink pulseless" vs "white pulseless" hand |
| Nerve injury | Neuropraxia (most common), AIN most common in extension-type, ulnar most common in flexion-type |
| Compartment syndrome | Rate 0.1-0.3% overall, higher with floating elbow (~2%); do not place elbow in hyperflexion with swelling |
Late
| Complication | Details |
|---|---|
| Volkmann's ischaemic contracture | Due to missed compartment syndrome; muscles of anterior forearm compartment rendered ischemic; devastating and often permanent - forearm flexors become severely contracted |
| Cubitus varus ("Gunstock deformity") | Most common late complication; results from malunion with coronal plane tilt; deformity may require corrective osteotomy; primarily cosmetic but can cause functional problems |
| Cubitus valgus | Less common; can cause tardy ulnar nerve palsy |
| Myositis ossificans traumatica | Heterotopic ossification, often from excessive manipulation or aggressive physiotherapy |
| Fishtail deformity | Avascular necrosis of the trochlea causing irregular distal humeral shape |
| Stiffness | Loss of terminal extension most common; usually improves with time |
Note on cubitus varus: Varus deformity often does not remodel because it occurs in the coronal plane - the distal humerus does not grow in a way that corrects this deformity, unlike anteroposterior angulation.
- S Das Manual on Clinical Surgery | Campbell's Operative Orthopaedics 15th Ed 2026 | Bailey and Love's Short Practice of Surgery
Special Scenarios
Floating Elbow
When the supracondylar fracture is associated with an ipsilateral forearm fracture (radius and/or ulna) - occurs in ~5% of type III fractures. This is associated with higher complication rates including compartment syndrome (~2%). Consider urgent fixation for higher-energy injuries.
Ipsilateral Distal Radial Fracture
5-10% of children with supracondylar fractures have an associated distal radial fracture - easily missed.
Obese Children
Higher rate of preoperative and postoperative nerve palsy, and higher likelihood of needing open reduction.
Summary
Supracondylar fractures are the most feared pediatric elbow injury because of neurovascular complications. The priority at presentation is always neurovascular assessment first, followed by fracture classification. The treatment follows the Gartland type - undisplaced fractures are immobilized, while displaced fractures (especially type IIB, III, IV) require CRPP. Volkmann's ischemic contracture (due to compartment syndrome) and cubitus varus (from malunion) are the two most important late complications to prevent and recognize.
This is a shared conversation. Sign in to Orris to start your own chat.