Posterolateral face involvement with Ho of lf hemiplegia diagnosis and dd
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
lateral medullary syndrome Wallenberg brainstem cross section anatomy
Reading File
Reading File
I now have comprehensive information. Let me compile the full answer.
Posterolateral Face Involvement with Ipsilateral (Homo-lateral) Hemiplegia
Understanding the Clinical Pattern
The combination of posterolateral face sensory loss (pain & temperature) + ipsilateral hemiplegia is a rare but diagnostically critical pattern because it is anatomically paradoxical — normally, a lateral medullary lesion causes ipsilateral face + contralateral body sensory loss, with no hemiplegia (pyramids are medial and spared).
When hemiplegia is ipsilateral to the face involvement, this points to a lesion that has extended below the pyramidal decussation.
Primary Diagnosis: Opalski Syndrome (Submedullary Syndrome)
Definition
Opalski syndrome = Classic lateral medullary (Wallenberg) syndrome + ipsilateral hemiplegia/hemiparesis.
Mechanism
The key anatomical explanation:
- Standard Wallenberg syndrome affects the lateral medulla above the pyramidal decussation → corticospinal tract not yet crossed → contralateral hemiplegia (which is typically absent since the pyramids are medial and spared).
- In Opalski syndrome, the lesion extends caudally into the lower medulla, below the level of the pyramidal decussation — i.e., into the submedullary/upper cervical region where the corticospinal tract has already crossed → damage here produces ipsilateral UMN hemiplegia.
"When ipsilateral hemiplegia is associated with symptoms of a lateral medullary syndrome, it corresponds to the submedullary syndrome of Opalski. The ipsilateral hemiplegia is due to the caudal extension of the lesion of the lower medulla involving the corticospinal tract after the pyramidal decussation." — Localization in Clinical Neurology, 8e
Etiology
- Steno-occlusive disease of the vertebral artery (VA)
- Vertebral artery dissection
- Compromise of medullary penetrating arteries
Full Clinical Picture of Lateral Medullary (Wallenberg) Syndrome + Opalski
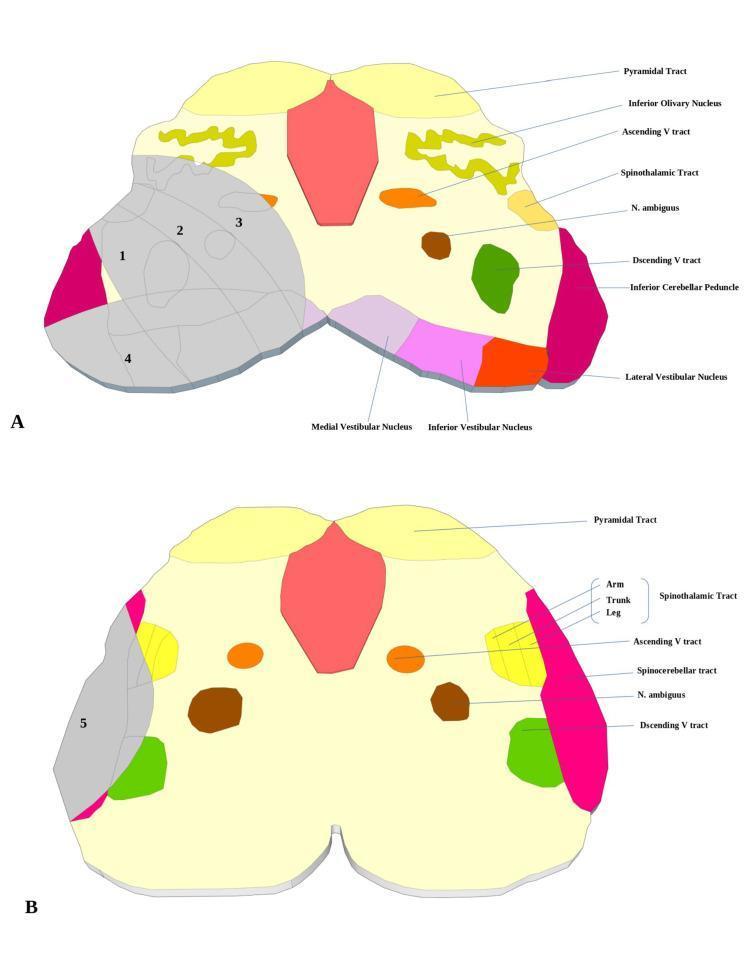
The posterolateral face involvement is due to the spinal nucleus and tract of CN V (trigeminal), which runs through the posterolateral medulla. In Opalski, on top of the classic Wallenberg features, you add ipsilateral hemiplegia:
| Feature | Structure Involved | Side |
|---|---|---|
| Pain & temperature loss — face | Spinal nucleus/tract of CN V | Ipsilateral |
| Pain & temperature loss — body | Lateral spinothalamic tract | Contralateral (classic) |
| Horner syndrome (miosis, ptosis, anhidrosis) | Descending sympathetic tract | Ipsilateral |
| Vertigo, nystagmus, nausea/vomiting | Vestibular nuclei | — |
| Dysphagia, hoarseness, ↓ gag | CN IX, X nuclei (nucleus ambiguus) | Ipsilateral |
| Cerebellar signs, limb ataxia | Inferior cerebellar peduncle, restiform body | Ipsilateral |
| Lateropulsion | Vestibulospinal/spinocerebellar tracts | — |
| Ipsilateral hemiplegia (Opalski feature) | Corticospinal tract below pyramidal decussation | Ipsilateral |
Why Posterolateral Face Specifically?
The spinal (descending) nucleus and tract of the trigeminal nerve courses through the entire lateral medulla in a posterolateral position. It carries pain and temperature from the ipsilateral face (onion-skin pattern, concentric — outer face = more caudal nucleus). Lesions here produce:
- Ipsilateral facial loss of pain and temperature (tactile sense preserved — main sensory nucleus is in pons)
- The classic crossed sensory pattern: ipsilateral face + contralateral body (due to already-crossed spinothalamic tract)
Differential Diagnosis
1. Classic Wallenberg Syndrome (Lateral Medullary Syndrome)
- Same ipsilateral face + contralateral body sensory loss
- No hemiplegia (pyramids spared — medial medulla)
- Cause: PICA or vertebral artery occlusion
- Key distinguishing feature from Opalski: absence of ipsilateral motor deficit
2. Hemimedullary Syndrome (Babinski-Nageotte Syndrome)
- Combined lateral + medial medullary infarction simultaneously
- Ipsilateral face loss (CN V) + contralateral hemiplegia (medial medulla, above decussation) + ipsilateral tongue palsy (CN XII) + ipsilateral Horner + ipsilateral cerebellar signs
- Caused by proximal VA occlusion (before PICA and anterior spinal artery branches)
3. Medial Medullary Syndrome (Dejerine Syndrome)
- Contralateral hemiplegia (pyramids — above decussation)
- Contralateral loss of position/vibration (medial lemniscus)
- Ipsilateral tongue palsy (CN XII)
- No face involvement (spinal V tract spared)
- Cause: anterior spinal artery or VA medial branch occlusion
4. Lateral Pontomedullary Syndrome (AICA Territory)
- All Wallenberg features +
- Ipsilateral facial weakness (CN VII involvement)
- Ipsilateral tinnitus/hearing loss (CN VIII)
- No hemiplegia (unless extended)
5. Complete Unilateral Medullary Infarction (Reinhold Syndrome / Total Lateral Medullary Syndrome)
- All of Wallenberg + extension → crosses medial structures too
- Can have ipsilateral hemiplegia via submedullary mechanism
6. Cervical Cord (C1–C2) Lesion
- Ipsilateral hemiplegia (below decussation)
- Ipsilateral face involvement if ascending V tract involved
- But: typically no vestibular, cerebellar, or autonomic features of Wallenberg
7. Multiple Sclerosis / Demyelination
- Can produce any combination of brainstem signs
- Young patient, relapsing course, MRI lesions elsewhere
Imaging & Diagnostic Approach
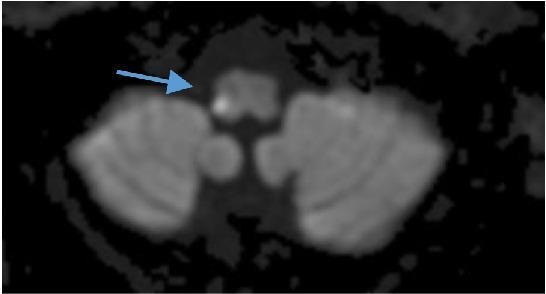
MRI (DWI + FLAIR) is the investigation of choice:
- Axial DWI: hyperintense signal in the lateral medulla (Wallenberg) with extension toward the cervicomedullary junction (Opalski)
- MRA or CT angiography: vertebral artery stenosis/dissection
- If VA dissection suspected: fat-sat MRI of neck
Summary Table: Key Differentials
| Syndrome | Face | Body Motor | Body Sensory | Tongue | Key Vessel |
|---|---|---|---|---|---|
| Opalski | Ipsi pain/temp ↓ | Ipsilateral UMN | Contra pain/temp ↓ | Spared | VA (distal/dissection) |
| Wallenberg | Ipsi pain/temp ↓ | None | Contra pain/temp ↓ | Spared | PICA/VA |
| Babinski-Nageotte | Ipsi pain/temp ↓ | Contralateral UMN | Contra all modalities ↓ | Ipsi atrophy | Proximal VA |
| Dejerine (medial medullary) | None | Contralateral UMN | Contra vibration/position ↓ | Ipsi atrophy | Ant spinal/VA branch |
| AICA (pontomedullary) | Ipsi all modalities ↓ + facial palsy | None/minimal | Contra pain/temp ↓ | Spared | AICA |
References:
- Localization in Clinical Neurology, 8e — Chapter 15, Opalski (Submedullary) Syndrome, p. 930
- Adams and Victor's Principles of Neurology, 12th ed. — Lateral Medullary Syndrome, p. 816
- Neuroanatomy through Clinical Cases, 3rd ed. — Table 14.7, Focal Vascular Syndromes of the Medulla
5th cn onion skin pattern and balaclava pattern expain and explain 5th nerve distribution
Finding Sources
Finding Sources
Finding Sources
Searching Images
trigeminal nerve onion skin pattern face sensory distribution V1 V2 V3
Reading File
Reading File
Searching Images
trigeminal spinal nucleus caudalis somatotopic onion skin concentric facial sensory diagram
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
I now have everything needed. Here is the comprehensive answer:
CN V (Trigeminal Nerve) — Full Distribution, Onion-Skin & Balaclava Patterns
Part 1: CN V Anatomy & Nuclear Complex
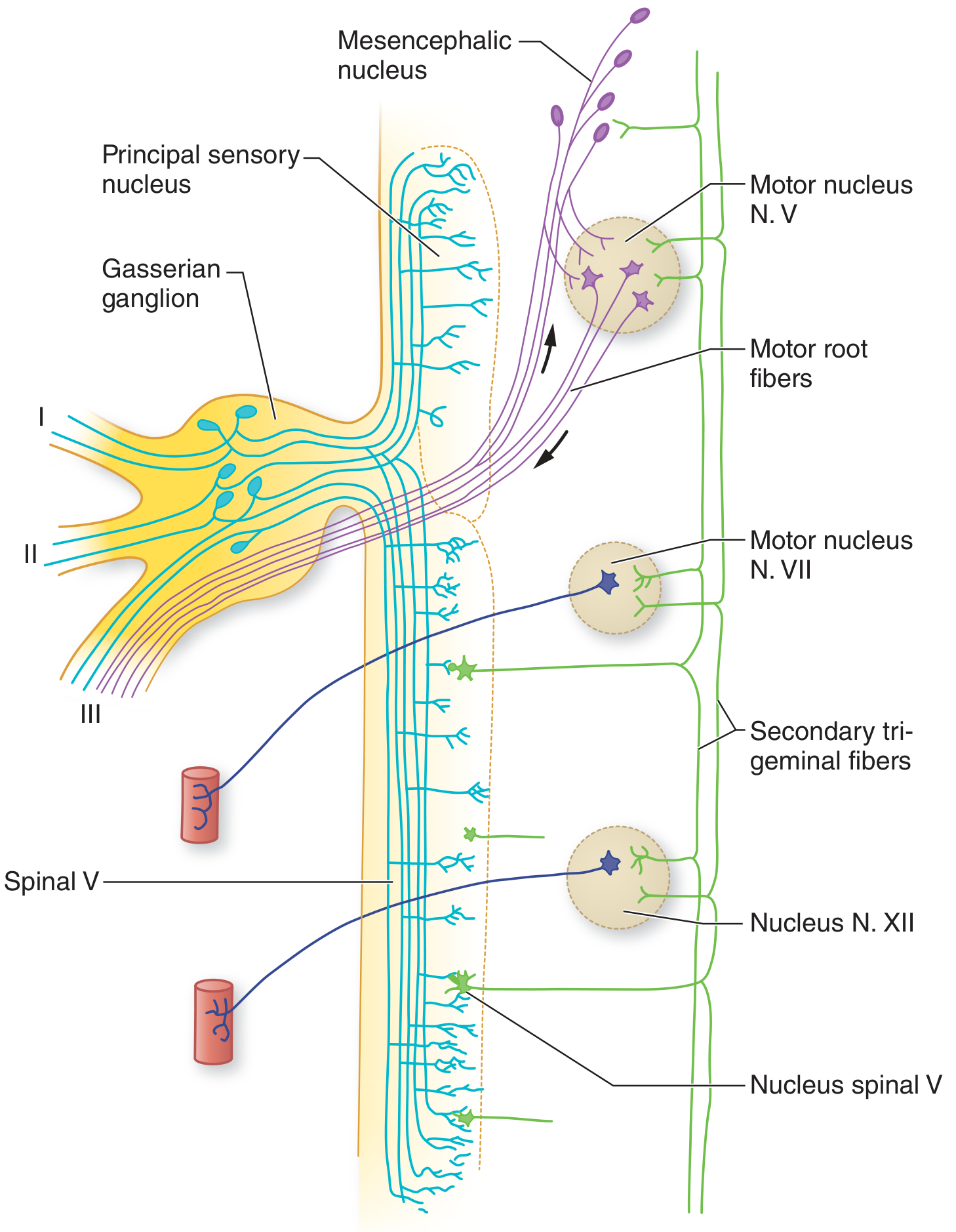
The trigeminal nerve (CN V) is the largest cranial nerve and has one motor root (portio minor) and one large sensory root (portio major). The pseudounipolar cell bodies of the sensory root lie in the Gasserian (semilunar) ganglion at the apex of the petrous bone.
Four Nuclei of CN V
| Nucleus | Location | Function |
|---|---|---|
| Mesencephalic nucleus | Midbrain → upper pons | Proprioception from masticatory muscles; mediates jaw jerk |
| Principal (main) sensory nucleus | Lateral pons | Touch, pressure, two-point discrimination from face |
| Spinal nucleus of V (nucleus caudalis) | Pons → medulla → C2–C4 spinal cord | Pain, temperature, crude touch from face |
| Motor nucleus | Mid-pons | Motor to muscles of mastication (masseter, temporalis, pterygoids) |
Part 2: Three Peripheral Divisions & Their Distribution
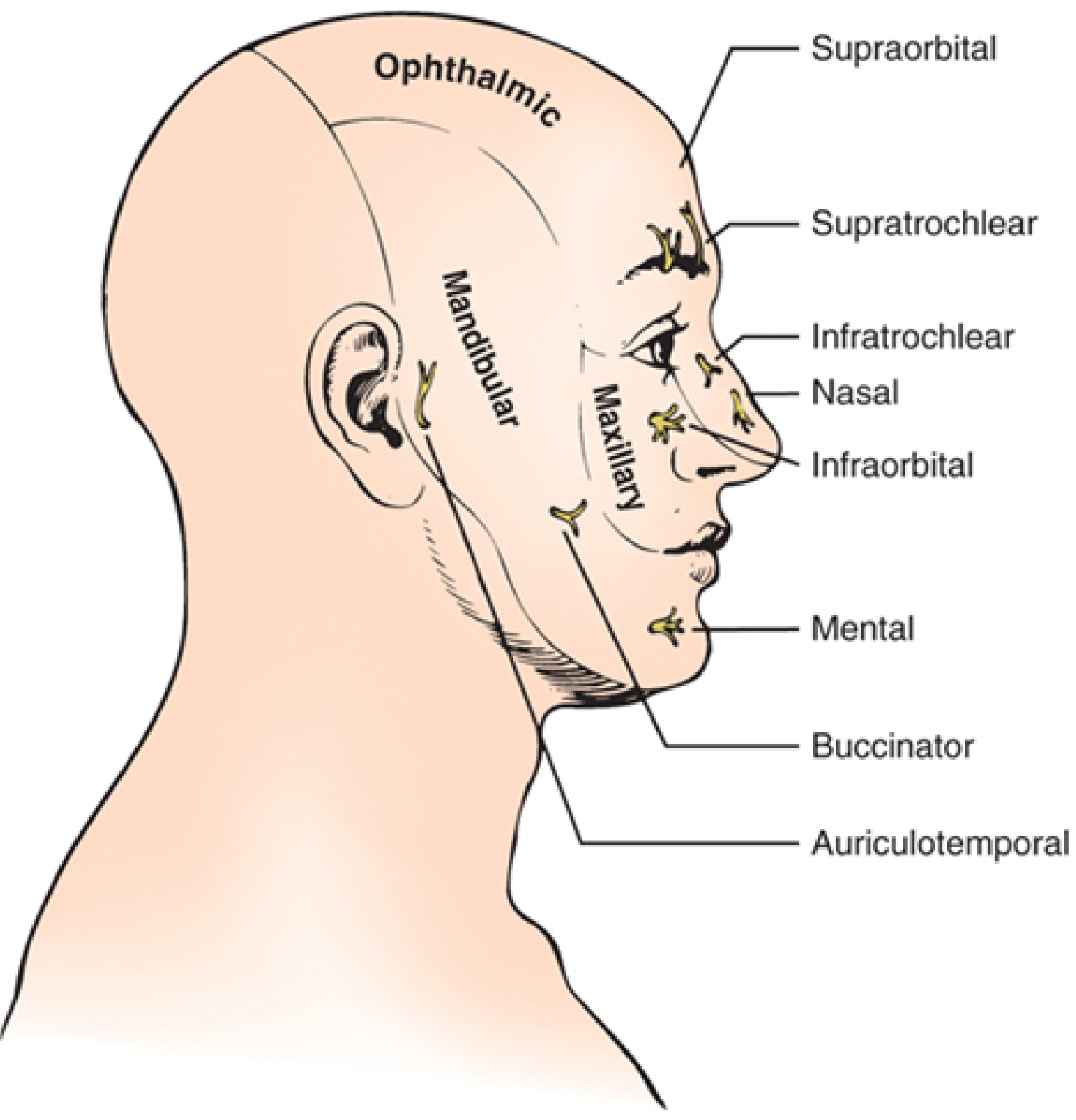
V1 — Ophthalmic Division
- Exits skull via superior orbital fissure
- Runs through the lateral wall of cavernous sinus
- Branches: frontal (supraorbital + supratrochlear), lacrimal, nasociliary
- Supplies:
- Forehead and scalp up to lambdoidal suture
- Upper eyelid, conjunctiva, cornea
- Nose (dorsum, tip, nasal mucosa)
- Frontal, sphenoidal, ethmoidal sinuses
- Dura of anterior fossa, falx, tentorium (meningeal branch)
- Mediates corneal reflex (afferent limb)
V2 — Maxillary Division
- Exits skull via foramen rotundum → sphenopalatine fossa → inferior orbital fissure → infraorbital foramen
- Branches: infraorbital, zygomatic, palatine, nasal, superior alveolar
- Supplies:
- Cheek, lower eyelid, upper lip
- Upper teeth and gums, hard palate
- Maxillary sinus, nasal cavity floor
- Nasopharynx, soft palate
V3 — Mandibular Division
- Mixed nerve (only division with motor fibers)
- Exits skull via foramen ovale
- Branches: auriculotemporal, inferior alveolar (mental nerve), lingual, buccal
- Supplies sensory to:
- Lower lip, chin, lower jaw, lateral face anterior to ear
- Lower teeth and gums
- Anterior 2/3 of tongue (general sensation; taste = chorda tympani/VII)
- Temporomandibular joint, external ear
- Motor to: masseter, temporalis, medial & lateral pterygoids, tensor tympani, tensor veli palatini, mylohyoid, anterior digastric
Important exception: The angle of the jaw (parotid area) is NOT supplied by CN V — it is supplied by the great auricular nerve (C2–C3). This helps distinguish peripheral CN V lesions from C2–C3 lesions.
Part 3: The Spinal Nucleus — Key to the Two Patterns
The spinal nucleus of CN V extends from the mid-pons all the way to C2–C4 and is divided into:
- Pars oralis (pons → inferior olive): intraoral/dental sensation
- Pars interpolaris (inferior olive → obex): pain from teeth
- Pars caudalis (obex → C2–C4): pain & temperature from face; continuous with dorsal horn
Critically, the spinal nucleus has two overlapping somatotopic representations:
Part 4: The TWO Patterns of CN V Sensory Loss
Pattern 1 — "Peripheral" or Divisional Pattern (V1/V2/V3 Strips)
This occurs with peripheral nerve lesions (ganglion, nerve trunk, or root).
- Sensory loss follows the anatomical territory of one division:
- V1 lesion → forehead, upper lid, cornea
- V2 lesion → cheek, lower lid, upper lip
- V3 lesion → lower lip, chin, jaw (sparing angle of jaw)
- All modalities (touch, pain, temperature) affected together
- Arranged in vertical/horizontal strips across the face
- Example causes: trigeminal neuralgia, skull base tumor, Gasserian ganglion lesion, cavernous sinus pathology, herpes zoster (dermatomal)
Pattern 2 — "Onion Skin" / Concentric Pattern (Intramedullary / Nuclear)
This occurs with lesions of the spinal nucleus of CN V within the brainstem.
The Anatomy Behind It
There is a second somatotopic arrangement within the spinal nucleus where:
"The midline facial areas (nose and mouth) are represented rostrally in the spinal nucleus, whereas the more lateral facial sensation fibers terminate in more caudal spinal nucleus regions." — Localization in Clinical Neurology, 8e
In other words:
- Perioral region (lips, nose, central face) → represented in the rostral spinal nucleus (pons/upper medulla)
- Lateral face (cheeks, temple, ear region) → represented in the caudal spinal nucleus (lower medulla/C1–C2)
The Onion-Skin Pattern
Imagine concentric rings like an onion (or the rings of a dartboard):
- The innermost ring (perioral — lips, nose, central face) = most rostral nucleus
- The outermost ring (lateral face, temple, preauricular) = most caudal nucleus
| Level of spinal nucleus lesion | Area of facial sensory loss |
|---|---|
| Rostral (pons/upper medulla) | Perioral ring — around the mouth and nose only |
| Middle (mid-medulla) | Wider ring — central + mid-face |
| Caudal (lower medulla/C1–C2) | Entire face including lateral face up to ear |
So with a progressive/expanding caudal lesion, sensory loss expands from the outside in (lateral to medial); with a rostral lesion, only the central face (perioral) is affected.
This pattern of centrifugal concentric ring loss around the mouth = "onion skin" (or "onion peel") pattern.
Clinical implication
- Perioral numbness = rostral spinal nucleus lesion (high medulla / lower pons) — e.g., small Wallenberg infarct, syringobulbia
- Wide lateral face loss = more caudal involvement — e.g., upper cervical syrinx extending to C2
Pattern 3 — "Balaclava Helmet" Pattern
A balaclava is a full-face ski mask that leaves only the central face exposed (eyes, nose, mouth area uncovered) while covering the scalp, sides of face, and back of head.
What it means neurologically
The balaclava pattern of sensory loss is the inverse of the peripheral distribution:
- Spared: Central face (perioral, perinasal) — i.e., areas supplied by C2 (great auricular nerve) that do NOT overlap with CN V
- Lost: Lateral face, scalp, and forehead — CN V territory
- More accurately: refers to sensory loss over the scalp and lateral face extending posteriorly, involving the posterior scalp which has cervical (C2, C3) overlap
In Clinical Use
The balaclava pattern is most classically described in:
-
Syringomyelia/Syringobulbia — as the syrinx ascends into the brainstem:
- Initial caudal involvement of spinal nucleus → lateral face loss
- Sparing of perioral (rostral nucleus) = balaclava-like distribution
-
Cervical cord lesions at C1–C2 — where C2 dorsal root inputs overlap with the caudal trigeminal nucleus:
- Saddle-distribution loss at the crown of the scalp + lateral face
- Perioral area (V3 rostral) spared
-
The "reverse" or "inverted onion skin" — with high cervical cord lesions, sensory loss is maximal laterally (ears, temples, scalp) and the inner perioral region is preserved — giving the appearance of the face wearing a balaclava (the fabric part covering the outside, the central holes remaining sensate).
Key Distinction
| Pattern | Location | Sensory Loss | Spared |
|---|---|---|---|
| Peripheral (divisional) | Gasserian ganglion / nerve trunk | V1 or V2 or V3 strip | Other divisions |
| Onion skin | Spinal nucleus (intramedullary) | Concentric rings from perioral outward | Depends on level |
| Balaclava | Caudal spinal V nucleus / C1–C2 | Lateral face, scalp, behind ear | Central face (perioral, lips, nose) |
Summary Diagram (Conceptual)
FACE (viewed from front):
PERIPHERAL PATTERN: ONION SKIN PATTERN: BALACLAVA PATTERN:
V1 │ V1 │ V1 ╔═══════════════╗ ░░░░░░░░░░░░░
V2 │ V2 │ V2 ║ ╔═════════╗ ║ ░ ┌─────┐ ░
V3 │ V3 │ V3 ║ ║ ╔═════╗ ║ ║ ░ │ OK │ ░
(vertical strips) ║ ║ ║PERI-║ ║ ║ ░ │(C/F)│ ░
║ ║ ║ORAL ║ ║ ║ ░ └─────┘ ░
║ ║ ╚═════╝ ║ ║ ░░░░░░░░░░░░░
║ ╚═════════╝ ║ (lateral+scalp lost)
╚═══════════════╝
Reflex Summary
| Reflex | Afferent (V) | Efferent | Lesion effect |
|---|---|---|---|
| Corneal reflex | V1 (ophthalmic) | CN VII (orbicularis) | Ipsi + contra blink lost if V1 lesion |
| Jaw jerk | V3 proprioceptive → mesencephalic nucleus | V3 motor → masseter | ↓ with V3/nuclear lesion; ↑↑ with bilateral UMN lesion |
| Blink/glabellar reflex | V1 main sensory nucleus | CN VII bilateral | Absent in V1 or facial N lesion |
References:
- Localization in Clinical Neurology, 8e — Sensory Portion, p. 741–742; Onion skin pattern, p. 742
- Adams & Victor's Principles of Neurology, 12e — Trigeminal nuclei, p. 1367
- Neuroanatomy through Clinical Cases, 3rd ed. — CN V nuclear lesions
Mri s/o hyperintensity in bilateral temporal and cerebellar lobe with 2yr h/o progressive cerebellar symptoms diagnosis
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.