Explain NSTEMI ECG please.
Reading File
Finding Sources
Finding Sources
Searching Images
NSTEMI ECG ST depression T wave inversion
Reading File
Reading File
I have rich textbook content and excellent ECG images. Let me compile the answer now.
NSTEMI ECG
Pathophysiological Basis
In NSTEMI, the culprit lesion causes partial-thickness (subendocardial) ischemia — the occlusion is incomplete or collateral flow protects the epicardium. Because transmural injury does not occur, there is no ST elevation and no pathological Q waves develop. The ECG reflects subendocardial damage through repolarization changes.
Core ECG Findings
1. ST-Segment Depression (most characteristic)
- The hallmark finding — occurs in ~50% of UA/NSTEMI patients and in about one-third of all NSTE-ACS patients
- Must be present in ≥2 contiguous leads to be diagnostic
- Threshold for abnormal J-point depression:
- ≥0.5 mm in leads V2 and V3
- ≥1 mm in all other leads
- Morphology: horizontal or downsloping ST depression is more specific for ischemia than upsloping
2. T-Wave Inversions
- More common than ST depression but less specific
- Become significant when new and deep (≥3 mm / ≥0.3 mV)
- Typically symmetric and pointed
3. Pseudo-normalization of T Waves
- A previously inverted T wave that becomes upright during an ischemic episode — a subtle but important dynamic change
4. No ST Elevation (by definition)
- Absence of ST elevation distinguishes NSTEMI from STEMI
- No new pathological Q waves form (unlike STEMI)
Important Patterns to Recognize
ST Depression + ST Elevation in aVR (± V1)
Diffuse ST depression in multiple leads plus ST elevation in aVR and/or V1 is a high-risk pattern suggesting:
- Left main or proximal LAD occlusion
- Multi-vessel disease This combination mandates urgent angiography (<2 hours).
Wellens Syndrome
- Biphasic or deeply inverted T waves in V2–V4 with QT prolongation
- Occurs in setting of stuttering chest pain in prior 24 hours
- Represents a critical LAD stenosis (often 90%+)
- Two types: Type A (biphasic) and Type B (deep symmetric inversion)
Serial ECG Monitoring
Serial ECGs are essential because NSTEMI changes are dynamic:
- ST depression may be transient and normalize between episodes
- T-wave inversions can deepen hours to days after the event and then gradually resolve
- Comparison with prior ECGs is critical to identify new changes
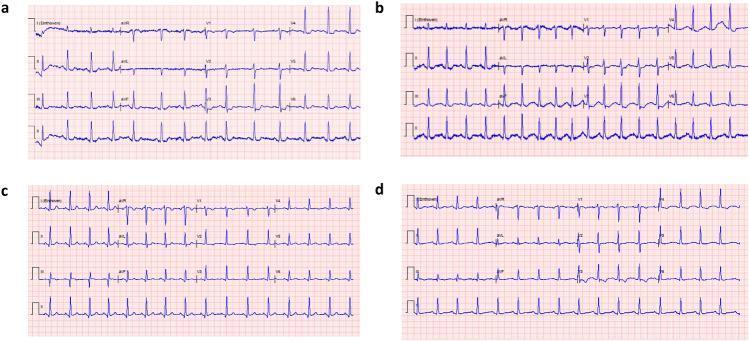
The image below shows the temporal evolution — from initial ST depression at presentation through normalization after reperfusion:
The 12-Lead Picture
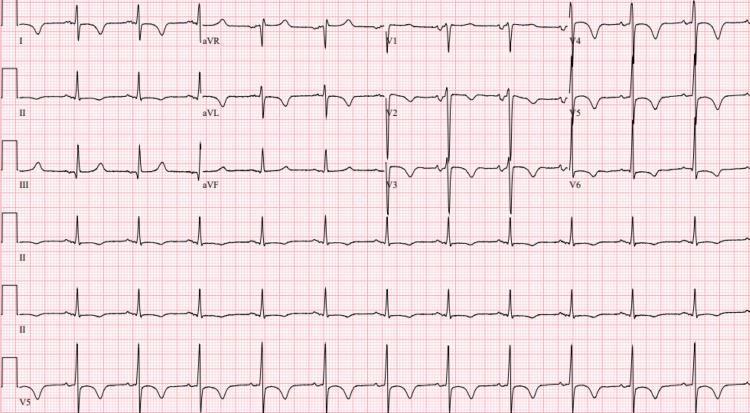
This tracing shows widespread ST depression and deep symmetric T-wave inversions in anteroseptal (V1–V3) and lateral leads (I, aVL, V4–V6) — a high-risk NSTEMI pattern with prolonged QTc.
Limitations of the ECG
- A normal ECG does not exclude NSTEMI — up to 50% of patients have a normal or non-diagnostic tracing at presentation
- The posterior circulation (circumflex territory) is poorly seen on standard leads → consider posterior leads (V7–V9) or echocardiography when suspicion is high
- Non-specific ST changes or T-wave inversions that don't meet voltage criteria are non-diagnostic but still carry higher risk for future events
Summary Table
| Feature | NSTEMI | STEMI |
|---|---|---|
| ST segments | Depression (or no change) | Elevation |
| T waves | Inversion or pseudo-normalization | Hyperacute early, then inversion |
| Q waves | Absent | Develop (transmural) |
| Troponin | Elevated | Elevated |
| Occlusion | Partial / incomplete | Complete |
| Territory | Subendocardial | Transmural |
Sources: Washington Manual of Medical Therapeutics, p. 133; Harrison's Principles of Internal Medicine 22E, p. 2151; Textbook of Family Medicine 9e.
This is a shared conversation. Sign in to Orris to start your own chat.