Tympanic membrane, S.A.Q in Vishram Singh.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a thorough SAQ-style answer on the tympanic membrane. Note: Vishram Singh's textbook is not in the library, but the content below covers exactly the same SAQ syllabus topics (the anatomy curriculum is identical across Vishram Singh, Gray's Anatomy for Students, and standard ENT texts).
Tympanic Membrane - SAQ (Anatomy)
Note: Vishram Singh's anatomy textbook is not available in this library, but the content below follows the exact SAQ format and covers all standard topics Vishram Singh addresses on the tympanic membrane.
1. Introduction / Definition
The tympanic membrane (eardrum) is a thin, semi-transparent, fibrous disc that separates the external acoustic meatus from the middle ear (tympanic) cavity. Its diameter is approximately 9 mm.
2. Position and Orientation
- It is set obliquely at the medial end of the external acoustic meatus.
- It slopes medially from above downward, and posteriorly to anteriorly.
- Its lateral surface therefore faces inferiorly and anteriorly.
- It is attached peripherally via a fibrocartilaginous ring (fibrous annulus) to the tympanic sulcus of the temporal bone.
3. Structure / Layers (Trilaminar)
The tympanic membrane has three layers:
| Layer | Description |
|---|---|
| Outer (lateral) layer | Stratified squamous epithelium - continuous with skin of external acoustic meatus |
| Middle (fibrous) layer | Fibrous connective tissue with radially oriented fibers in the outer part and circular/parabolic fibers in the deeper part |
| Inner (medial) layer | Mucous membrane (cuboidal/columnar epithelium) - continuous with the mucosa of the middle ear |
The fibrous layer coalesces at the rim to form the fibrous annulus, which anchors the membrane in the tympanic sulcus.
4. Parts of the Tympanic Membrane
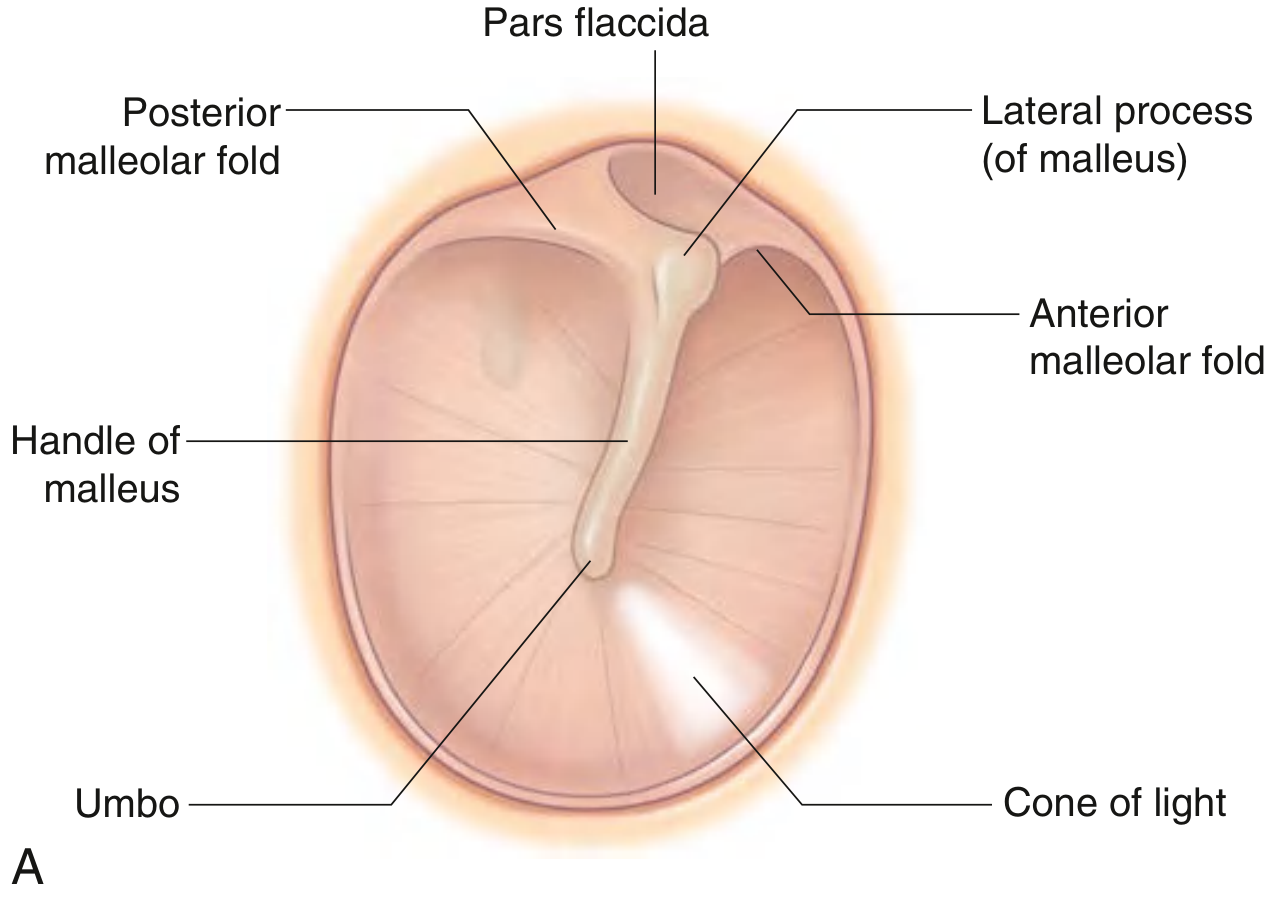
Fig: Right tympanic membrane - (A) Diagram showing key landmarks, (B) Otoscopic view
The membrane is divided into two parts by the anterior and posterior malleolar folds:
a) Pars Tensa (lower, larger part)
- Constitutes the majority of the membrane area.
- Contains all three layers (trilaminar structure).
- Taut and firm.
- Lamina propria is thin and strong, mainly type II collagen.
- Attached to the fibrous annulus in the tympanic sulcus.
b) Pars Flaccida (Shrapnell's membrane - upper, smaller part)
- Located superiorly, above the malleolar folds.
- Lacks the prominent middle fibrous layer (only 2 layers - squamous epithelium + mucosal epithelium).
- Loose and slack.
- Sits in the notch of Rivinus (a deficiency in the bony tympanic ring).
- Contains thicker, loosely arranged type I collagen - more elastic.
- Clinically important: Medial to it is Prussak's space - the most common site of primary cholesteatoma formation.
5. Key Surface Landmarks
| Landmark | Description |
|---|---|
| Umbo | Central concavity; the point where the tip of the handle (manubrium) of malleus attaches on the inner surface |
| Handle of malleus | Visible through the membrane running supero-inferiorly |
| Lateral process of malleus | Small bulge at the upper end of the handle, producing the malleolar prominence |
| Cone of light | Bright triangular light reflex visible anteroinferior to the umbo (at the 5 o'clock position in the right ear) on otoscopic examination |
| Anterior malleolar fold | Runs from lateral process of malleus anteriorly |
| Posterior malleolar fold | Runs from lateral process of malleus posteriorly |
6. Nerve Supply
Outer (lateral) surface:
- Primarily by the auriculotemporal nerve (branch of V3, mandibular division of trigeminal) - supplies the posterior and inferior region
- Auricular branch of the vagus nerve (Arnold's nerve / CN X) - supplies the anterior and superior aspect
- Small contribution from the facial nerve (CN VII) via the auricular branch of vagus
- Possibly a small contribution from glossopharyngeal nerve (CN IX)
Inner (medial) surface:
- Tympanic branch of glossopharyngeal nerve (Jacobson's nerve, CN IX)
Clinical point: Because the vagus nerve (CN X) supplies part of the tympanic membrane, stimulation (e.g., by syringing or inserting an otoscope) can trigger a cough reflex (Arnold's ear-cough reflex).
7. Blood Supply
Lateral surface (outer):
- Deep auricular branch of the internal maxillary (first part) artery forms a peripheral ring, from which branches supply the lateral surface.
Medial surface (inner):
- Anterior tympanic branch of the internal maxillary artery.
Venous drainage follows corresponding arterial anatomy (parallel venous channels).
Surgical note: The posterior aspect of the tympanic membrane has a richer blood supply - therefore the standard surgical incision is made in the posteroinferior quadrant.
8. Applied Anatomy / Clinical Importance
-
Otoscopic examination: Normal TM is relatively translucent with a gray-reddish tinge. The handle of malleus is visible at center; the cone of light is at 5 o'clock (right ear) or 7 o'clock (left ear).
-
Perforation: Most commonly caused by trauma or infection (otitis media). Perforations tend to heal spontaneously; surgical repair (myringoplasty/tympanoplasty) may be needed for large ones.
-
Myringotomy (paracentesis): Incision into the TM to drain middle ear fluid. Always made in the anteroinferior or posteroinferior quadrant to avoid:
- The chorda tympani nerve (runs in the upper one-third of the TM)
- The richer posterior blood supply is used for the standard surgical approach
-
Cholesteatoma: Originates from Prussak's space (immediately medial to pars flaccida). Presents as a pearly white mass with progressive bone erosion and conductive hearing loss.
-
Otitis media: Infection behind TM via the Eustachian tube. The TM appears red, bulging, and loses its light reflex. Can perforate if untreated, leading to hearing loss, meningitis, or brain abscess.
-
Arnold's ear-cough reflex: Stimulation of the auricular branch of vagus on the TM/external meatus causes reflex coughing - clinically relevant during otoscopy or ear syringing.
-
Referred otalgia: Due to multiple nerve supplies (V3, VII, IX, X), pain can be referred to the ear from the throat, tongue, teeth, tonsils, and larynx.
Sources: - Gray's Anatomy for Students, pp. 1096-1097 | Shambaugh Surgery of the Ear, p. 405 | Cummings Otolaryngology Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.