Types of hypersensitivity reaction
Reading File
Finding Sources
Searching the Web
types of hypersensitivity reactions Gell Coombs classification
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
types of hypersensitivity reactions Gell Coombs classification diagram
Loading Image
Loading Image
Here is a comprehensive overview of the four types of hypersensitivity reactions, based on the Gell and Coombs classification (1963).
Hypersensitivity Reactions — Gell & Coombs Classification
Hypersensitivity is an exaggerated or augmented immune response that is harmful to the host. It requires a presensitized state — reactions typically occur on second (or subsequent) exposure to the antigen. Coombs and Gell classified these into four types: Types I–III are antibody-mediated; Type IV is T-cell mediated.
Type I — Immediate (IgE-Mediated) Hypersensitivity
| Feature | Detail |
|---|---|
| Mediator | IgE antibody |
| Cells involved | Mast cells, basophils, eosinophils |
| Onset | Seconds to minutes after antigen exposure |
| Complement | Not involved |
Mechanism
- Sensitization: Antigen (allergen) stimulates B cells → IgE production → IgE binds to high-affinity FcεRI receptors on mast cells and basophils
- Re-exposure: Antigen cross-links surface-bound IgE molecules → degranulation
Mediators Released
- Primary (preformed): Histamine → vasodilation, ↑ capillary permeability, bronchospasm
- Secondary (newly synthesized): Prostaglandins, leukotrienes (from arachidonic acid), TNF-α, IL-4
- LTB4: chemoattractant for leukocytes
- LTC4, LTD4: vasodilation and ↑ vascular permeability
Clinical Examples
- Anaphylaxis (systemic — IV protein administration)
- Atopic disorders: Hay fever, asthma, eczema, urticaria
- Food allergies (shellfish), insect venom allergy
Treatment
Epinephrine, antihistamines, corticosteroids; avoidance of antigen; allergen immunotherapy (tolerance induction)
Type II — Cytotoxic (Antibody-Mediated) Hypersensitivity
| Feature | Detail |
|---|---|
| Mediator | IgG or IgM antibody directed at cell-surface or matrix antigens |
| Cells involved | RBCs, platelets, neutrophils; NK cells (ADCC) |
| Onset | Hours |
| Complement | Activated (MAC-mediated lysis) |
Mechanism
- Antibody binds to cell-surface antigen → complement activation → complement-mediated lysis, opsonization, or ADCC
- Antibodies to surface receptors may alter cell function without lysis (e.g., stimulating or blocking receptors)
Clinical Examples
- Hemolytic anemia (drug-induced, e.g., penicillin adsorption to RBCs)
- ABO transfusion reactions
- Rh hemolytic disease of the newborn
- Goodpasture syndrome (anti-GBM antibodies → kidney + lung damage)
- Graves disease (anti-TSH receptor antibody → receptor stimulation → hyperthyroidism)
- Myasthenia gravis (anti-AChR antibody → receptor blockade)
Type III — Immune Complex Hypersensitivity
| Feature | Detail |
|---|---|
| Mediator | Immune complexes (antigen–IgG/IgM) deposited in tissues |
| Cells involved | Neutrophils, macrophages |
| Onset | 6–12+ hours (local); days (systemic) |
| Complement | Activated → chemotaxis and inflammation |
Mechanism
- Normally immune complexes are removed; when they persist and deposit in tissues → complement activation → neutrophil/macrophage recruitment → proteases and inflammatory mediators → tissue injury
- Arthus reaction (local): Low-dose antigen injected intradermally → IgG + complement activation → local necrosis (12-hour onset)
- Serum sickness (systemic): Antigen–antibody complexes deposit in vessels, joints, kidneys
Clinical Examples
- Acute post-streptococcal glomerulonephritis (lumpy IgG + C3 deposits on GBM on immunofluorescence)
- Serum sickness
- Systemic lupus erythematosus (nephritis, vasculitis, arthritis)
- Hypersensitivity pneumonitis (inhalation of fungal spores/organic dust)
Type IV — Delayed (Cell-Mediated) Hypersensitivity
| Feature | Detail |
|---|---|
| Mediator | T lymphocytes (Th1, Th2, CTLs) — no antibody |
| Cells involved | CD4+ T cells (Th1/Th2), CD8+ CTLs, macrophages, neutrophils, eosinophils |
| Onset | 48–72 hours after antigen contact |
| Complement | Not involved |
Mechanism
Antigen presented by APCs via MHC → T-cell activation and proliferation → cytokine release → sustained inflammation
Modern classification divides Type IV into four subtypes (IVa–IVd):
| Subtype | T-cell Type | Key Cytokines | Effector Cells | Prototype Disease |
|---|---|---|---|---|
| IVa | Th1 | IFN-γ, IL-12 | Macrophages | Tuberculin reaction, contact dermatitis |
| IVb | Th2 | IL-4, IL-5, IL-13 | Eosinophils, mast cells | Allergic contact dermatitis, asthma-like |
| IVc | CTL (CD8+) | Perforin, granzyme B | Cytotoxic T cells | Stevens-Johnson syndrome, DRESS |
| IVd | T cells | CXCL8 (IL-8), GM-CSF | Neutrophils | Pustular drug reactions |
Clinical Examples
- Tuberculin (Mantoux) test — prototypical delayed-type reaction
- Contact dermatitis (nickel, poison ivy, topical neomycin)
- Granulomatous hypersensitivity (TB, leprosy, schistosomiasis — macrophage activation by IFN-γ)
Type IV Subtype Diagrams
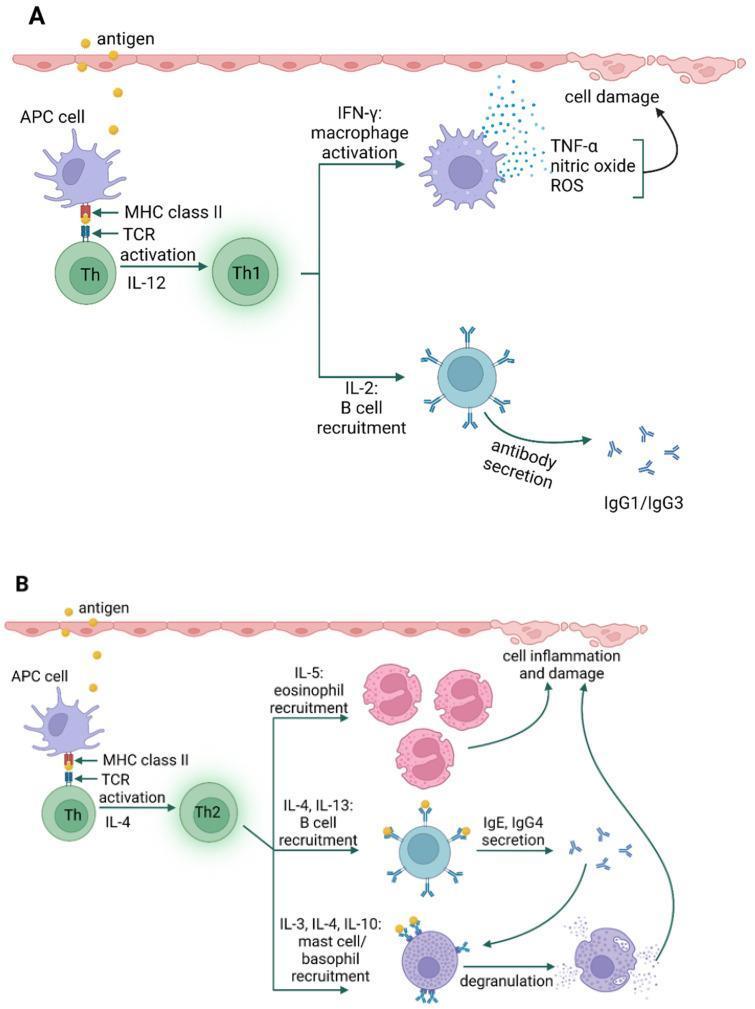
Type IVa: Th1-mediated macrophage activation. Type IVb: Th2-mediated eosinophil/mast cell recruitment.
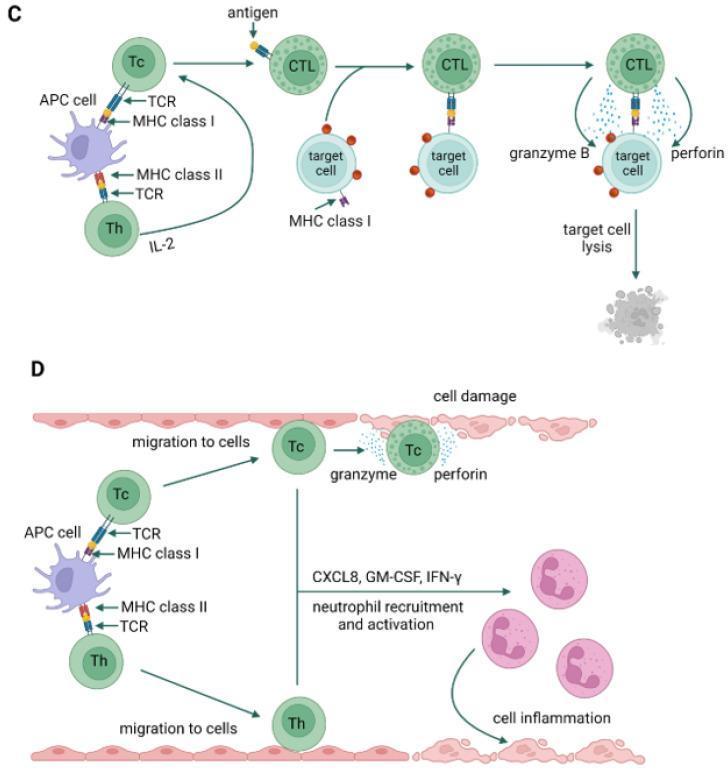
Type IVc: Cytotoxic T cell-mediated lysis via perforin/granzyme. Type IVd: Neutrophil recruitment via CXCL8 and GM-CSF.
Summary Table
| Type | Name | Antibody/Cell | Onset | Complement | Examples |
|---|---|---|---|---|---|
| I | Immediate / Anaphylactic | IgE | Seconds–minutes | No | Anaphylaxis, hay fever, asthma |
| II | Cytotoxic | IgG, IgM (vs. cell surface) | Hours | Yes | Hemolytic anemia, Goodpasture, Graves |
| III | Immune complex | IgG, IgM (soluble complexes) | 6–12 h | Yes | SLE, serum sickness, PSGN |
| IV | Delayed / Cell-mediated | T cells (no Ab) | 48–72 h | No | Contact dermatitis, TB test, granulomas |
Sources: Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.; Goldman-Cecil Medicine, International Edition
Circumcorneal congestion
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
circumcorneal congestion ciliary flush ophthalmology definition causes
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Searching Images
circumcorneal congestion ciliary flush perilimbal injection eye
Loading Image
Finding Sources
I now have all the information needed for a comprehensive answer. Here it is:
Circumcorneal Congestion (Ciliary Flush / Perilimbal Injection)
Definition
Circumcorneal congestion — also called ciliary flush, ciliary injection, or perilimbal injection — is circumcorneal conjunctival hyperaemia with a violaceous (purplish) hue, caused by dilation of the deeper episcleral and anterior ciliary vessels around the limbus. It indicates intraocular inflammation rather than surface disease.
"Ciliary injection is circumcorneal conjunctival hyperaemia with a violaceous (purplish) hue due to involvement of deeper blood vessels and is typically seen in anterior uveitis of acute onset." — Kanski's Clinical Ophthalmology, 10th Ed.
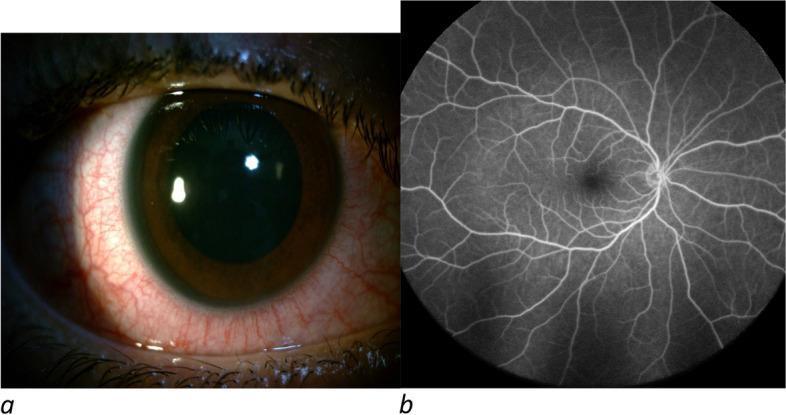
Panel (a): Slit-lamp photo showing circumcorneal injection — deep, violaceous-red ring of dilated episcleral vessels at the limbus. Panel (b): Fluorescein angiography shows no posterior segment involvement.
Anatomy of the Vessels Involved
The anterior ciliary arteries (branches of the ophthalmic artery) travel along the rectus muscles and penetrate the sclera near the limbus to supply the ciliary body, iris, and choroid. When the structures they supply become inflamed, these vessels — and the episcleral vessels at the limbus — become engorged, producing the characteristic perilimbal ring of redness.
Key points:
- Vessels are deep (episcleral and sub-conjunctival)
- They do not move with the conjunctiva when pushed with a cotton swab (unlike superficial conjunctival vessels)
- Redness is maximal at the limbus, fading peripherally toward the fornices (opposite of conjunctivitis)
- Blanching with topical adrenaline (phenylephrine) is absent or incomplete (unlike conjunctival injection)
Clinical Appearance
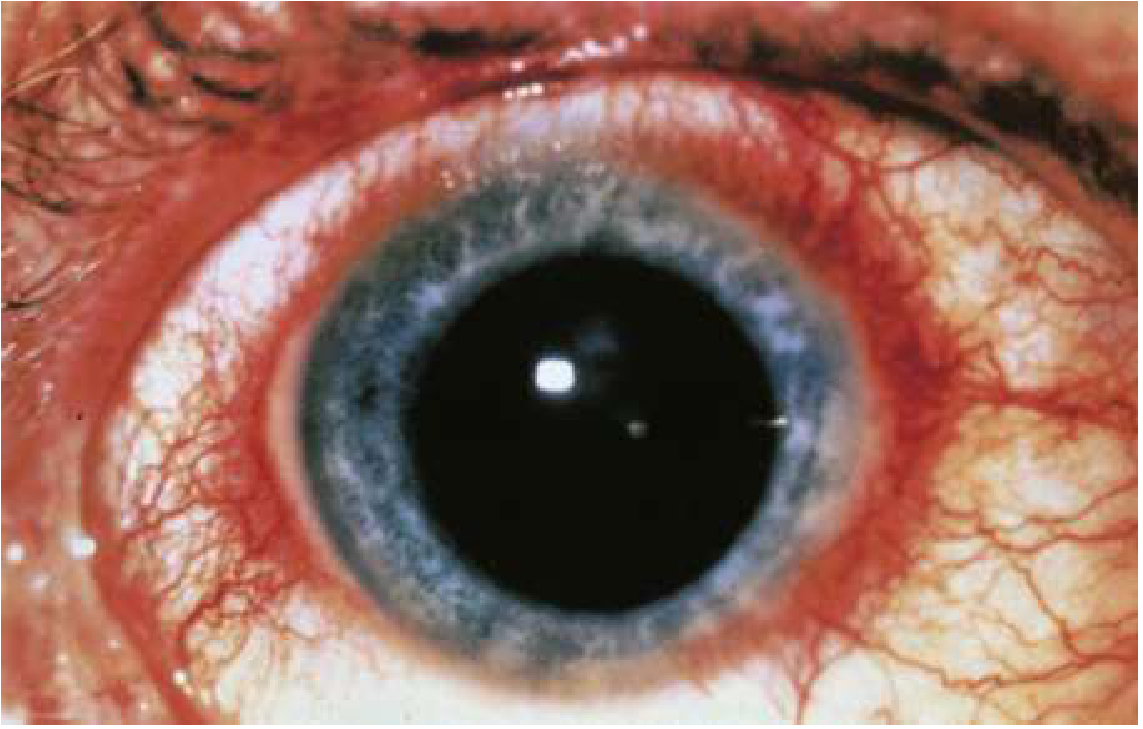
Ciliary flush: conjunctival injection is most prominent immediately around the limbus. (Rosen's Emergency Medicine)
Circumcorneal Congestion vs. Conjunctival Injection
| Feature | Circumcorneal Congestion (Ciliary Flush) | Conjunctival Injection |
|---|---|---|
| Vessels involved | Deep episcleral/anterior ciliary vessels | Superficial conjunctival vessels |
| Colour | Violaceous/purplish-pink | Bright red |
| Distribution | Maximal at limbus, fades peripherally | Maximal at fornix/periphery, fades toward limbus |
| Movement with conjunctiva | Does NOT move | Moves with conjunctiva |
| Blanching with phenylephrine | Absent / incomplete | Complete |
| Significance | Intraocular inflammation | Surface/conjunctival disease |
Causes (Conditions Producing Circumcorneal Congestion)
| Condition | Notes |
|---|---|
| Anterior uveitis / Iridocyclitis | Classic cause; especially HLA-B27-associated AAU. Associated with KPs, cells, flare, posterior synechiae, miosis |
| Acute angle-closure glaucoma | Severe, with corneal oedema, fixed mid-dilated pupil, very high IOP |
| Corneal ulcer / Infectious keratitis | Intense ciliary flush around ulcer; bacterial, fungal, or Acanthamoeba |
| Scleritis | Deep, boring pain; scleral vessel engorgement and ciliary flush |
| Endophthalmitis | Marked circumcorneal injection with hypopyon, proptosis |
| Chemical/UV burns | Limbal ischaemia with perilimbal congestion |
Ciliary flush is characteristically absent in some forms of chronic anterior uveitis (e.g., juvenile idiopathic arthritis-associated uveitis — the "white eye" uveitis) and occasionally absent even in acute anterior uveitis.
Associated Signs (in Anterior Uveitis)
When circumcorneal congestion is seen in anterior uveitis, look for:
- Miosis — pupillary sphincter spasm (predisposes to posterior synechiae)
- Keratic precipitates (KPs) — deposits on corneal endothelium in Arlt's triangle
- Cells and flare in anterior chamber (slit-lamp)
- Posterior synechiae — iris adhesions to lens
- Hypopyon — layered inflammatory cells inferiorly in the AC (common in HLA-B27, Behçet)
- Reduced visual acuity
Clinical Significance
Circumcorneal congestion is an important "red flag" sign indicating intraocular disease requiring urgent slit-lamp examination and ophthalmologic evaluation. Its presence should prompt investigation for anterior uveitis, raised IOP (glaucoma), keratitis, or scleritis — conditions where delayed treatment can lead to permanent vision loss.
Sources: Kanski's Clinical Ophthalmology, A Systematic Approach, 10th Ed.; Rosen's Emergency Medicine; Wills Eye Manual; Rosen's Emergency Medicine, 9th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.