Help me build concepts of corticospinal tract
Reading File
Finding Sources
Finding Sources
Searching Images
corticospinal tract anatomy diagram
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information to build a full concept map of the corticospinal tract. Let me compile the complete response:
Corticospinal Tract — Complete Conceptual Guide
1. Overview & Significance
The lateral corticospinal tract (CST) is the most clinically important descending motor pathway in the nervous system. It controls movement of the extremities, and lesions along its course produce characteristic deficits that enable precise clinical localization. It is synonymous with the pyramidal tract (though the pyramids also contain some reticulospinal fibers, making this terminology slightly imprecise).
"The corticospinal tract...is the most clinically important descending motor pathway in the nervous system." — Neuroanatomy through Clinical Cases, 3rd ed.
2. Cortical Origins (Upper Motor Neuron)
The CST does NOT arise solely from primary motor cortex. Fibers originate from multiple cortical areas:
| Cortical Area | Brodmann Area | % Contribution |
|---|---|---|
| Primary motor cortex (M1), precentral gyrus | Area 4 | ~31% |
| Premotor cortex + Supplementary Motor Area (SMA) | Area 6 | ~29% |
| Primary somatosensory cortex, postcentral gyrus | Areas 3, 1, 2 | ~40% combined from parietal lobe |
| Superior parietal lobule | Areas 5, 7 | (part of the 40% above) |
| Cingulate gyrus (medial surface) | — | small contribution |
Key cell type: Layer V pyramidal neurons (large neurons in cortical layer V). About 3% are giant Betz cells — the largest neurons in the human nervous system — located in M1.
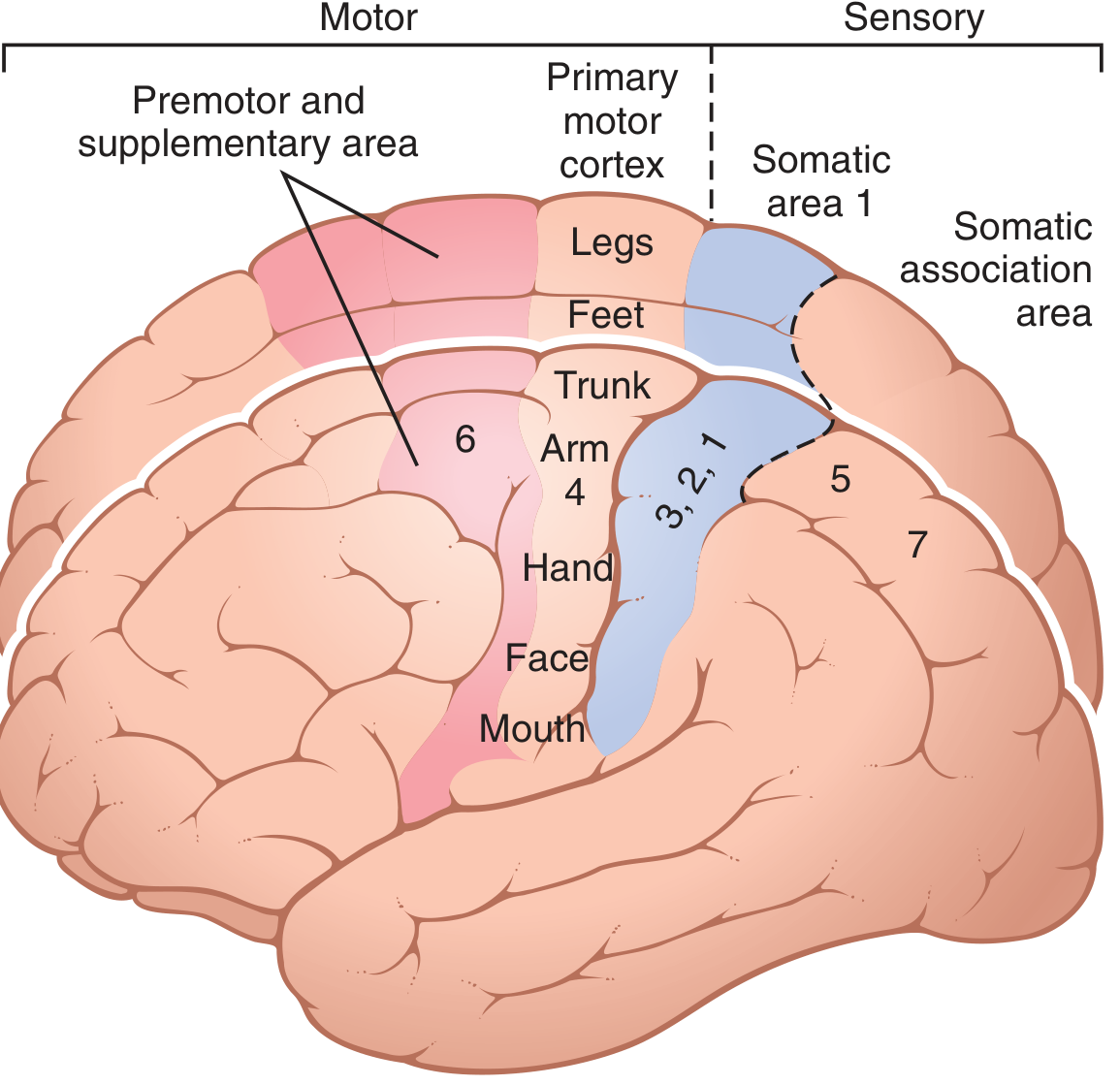
Primary motor cortex (area 4) with somatotopic organization: face/mouth laterally near sylvian fissure, arm/hand in mid-portion, trunk at apex, legs/feet dipping into longitudinal fissure (Guyton & Hall)
3. Somatotopic Organization (Homunculus)
The motor cortex is somatotopically organized:
- Face and mouth → near the sylvian fissure (lateral)
- Hand → large representation (more than half the primary motor cortex controls hands + speech)
- Arm → mid-portion
- Trunk → apex
- Leg and foot → dips into the longitudinal fissure (medial)
This disproportionate representation reflects the degree of fine motor control required — the hand and face have the largest cortical representation.
4. Course of the Tract — Level by Level
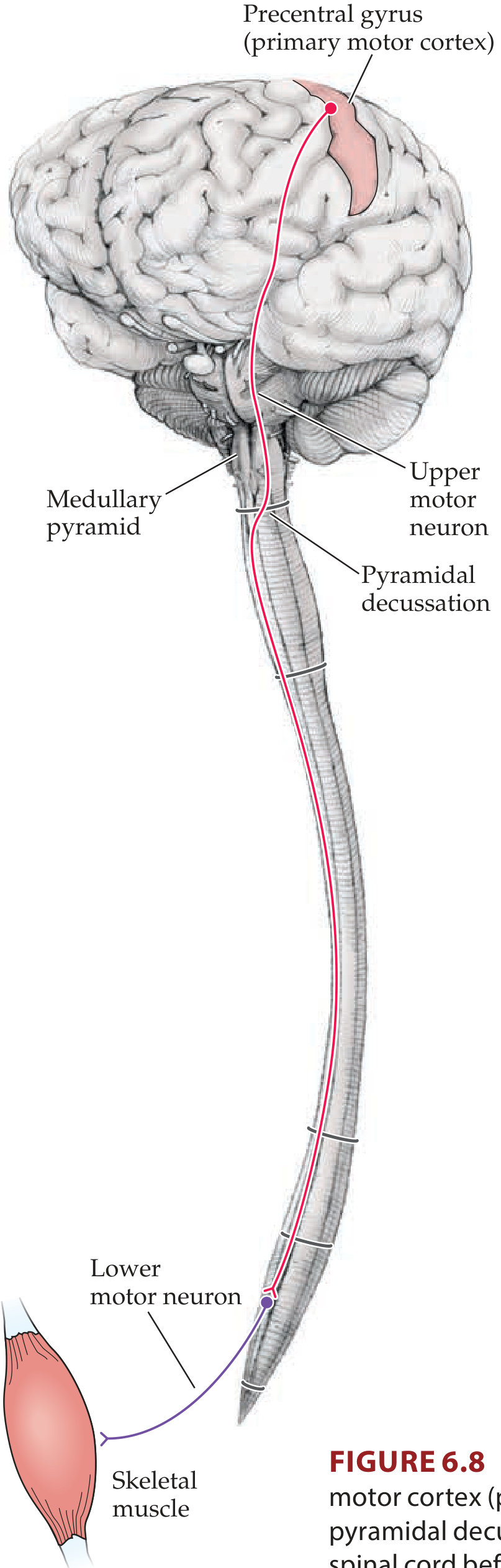
Figure 6.8 — Full course of the lateral corticospinal tract (Neuroanatomy through Clinical Cases, 3rd ed.)
Step-by-Step Descent:
① Cerebral Cortex → Corona Radiata
- Axons from cortex enter the corona radiata (fanlike white matter)
② Internal Capsule
- Fibers converge and pass through the posterior limb of the internal capsule
- Corticobulbar fibers (to cranial nerve nuclei) travel through the genu of the internal capsule
- Somatotopic arrangement: face fibers most anterior in posterior limb → leg fibers most posterior
③ Midbrain
- Fibers travel through the cerebral peduncles (crus cerebri) — in the middle 3/5
④ Pons
- Fibers are broken up into bundles by transverse pontocerebellar fibers
⑤ Medulla — Pyramids
- Fibers re-collect to form the medullary pyramids on the ventral aspect (these pyramids give the tract the name "pyramidal tract")
⑥ Pyramidal Decussation (caudal medulla)
- ~85–90% of fibers cross the midline → form the lateral corticospinal tract in the contralateral lateral funiculus
- ~10–15% do NOT cross → form the anterior (ventral) corticospinal tract in the ipsilateral ventral funiculus (crosses later in the ventral white commissure at the spinal cord level, mainly cervical + upper thoracic)
⑦ Spinal Cord
- Lateral CST: descends through the entire cord in the lateral funiculus, synapsing in laminae IV–IX (especially IX = anterior horn motor neurons)
- Anterior CST: limited to cervical + upper thoracic levels
5. Synaptic Targets in the Spinal Cord
| Target | Function |
|---|---|
| Directly onto α-motor neurons (lamina IX) | Monosynaptic connections for skilled, fine movements (especially in primates) |
| Spinal interneurons (laminae IV–VIII) | Indirect control, coordination of muscle groups |
| Dorsal horn (postcentral/parietal fibers) | Modulation of sensory input |
- Motor neurons innervating distal limb muscles (intrinsic muscles) are in the dorsolateral part of the anterior horn
- Motor neurons for axial/proximal muscles are in the ventromedial part
6. Two Subdivisions
| Feature | Lateral CST | Anterior (Ventral) CST |
|---|---|---|
| % of fibers | 85–90% | 10–15% |
| Decussation site | Pyramidal decussation (caudal medulla) | Ventral white commissure (at cord level) |
| Location in cord | Lateral funiculus | Ventral funiculus |
| Body region controlled | Distal limb muscles | Axial/proximal muscles (cervical + upper thoracic) |
| Clinical importance | Most important | Minor |
7. Upper vs. Lower Motor Neurons
This is the most clinically critical concept related to the CST:
| Feature | Upper Motor Neuron (UMN) Lesion | Lower Motor Neuron (LMN) Lesion |
|---|---|---|
| Tone | Spasticity (↑ tone) | Flaccidity (↓ tone) |
| Reflexes | Hyperreflexia | Hyporeflexia / Areflexia |
| Babinski sign | Present (extensor plantar response) | Absent |
| Atrophy | Mild (disuse) | Severe (denervation atrophy) |
| Fasciculations | Absent | Present |
| Weakness pattern | Pyramidal distribution (extensors in arm, flexors in leg) | Focal / patchy |
| Clonus | May be present | Absent |
UMN = neurons in the cortex/brainstem → entire CST pathway LMN = anterior horn cells (spinal cord) and cranial nerve motor nuclei → muscle
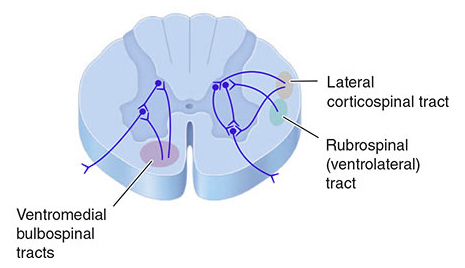
Spinal cord cross-section: lateral corticospinal tract (lateral white matter), rubrospinal tract, and ventromedial bulbospinal tracts — Harrison's Principles of Internal Medicine, p. 745
8. Related Descending Motor Pathways
| Tract | Origin | Function |
|---|---|---|
| Lateral CST | Motor/somatosensory cortex | Skilled voluntary movements, distal limbs |
| Corticobulbar | Motor cortex | Cranial nerve motor nuclei (face, tongue) |
| Rubrospinal (corticorubrospinal) | Red nucleus (midbrain tegmentum) | Supplements CST for limb movements |
| Lateral reticulospinal | Medullary reticular formation | Modulates tone/reflexes |
| Medial reticulospinal | Pontine reticular formation | Posture and gait |
| Vestibulospinal | Lateral vestibular nucleus | Balance, postural reflexes, extensor tone |
9. Internal Capsule Localization — Clinical Importance
The internal capsule is a critical bottleneck. Small lesions here (e.g., lacunar infarcts from lenticulostriate or anterior choroidal arteries) can cause:
- Pure motor hemiparesis — contralateral face + arm + leg weakness
- Dysarthria-clumsy hand syndrome
- Ataxic hemiparesis (if corticopontine fibers involved too)
The lesion is contralateral to the weakness because the CST decussates at the medullary pyramid.
10. Localization Rules — Key Principles
| Lesion Level | Deficits |
|---|---|
| Cortex (M1) | Contralateral weakness, often focal (face or arm or leg); UMN signs |
| Internal capsule / corona radiata | Contralateral face + arm + leg (hemiparesis); UMN signs |
| Cerebral peduncle | Contralateral hemiparesis + ipsilateral CN III palsy (Weber syndrome) |
| Pons | Contralateral hemiparesis + ipsilateral CN VI/VII palsy |
| Medulla (above decussation) | Contralateral hemiparesis + ipsilateral CN XII palsy (medial medullary syndrome) |
| Spinal cord (below decussation) | Ipsilateral hemiparesis (same side as lesion) + ipsilateral dorsal column loss |
11. Common Diseases Affecting the CST
| Disease | Level Affected |
|---|---|
| Stroke (MCA territory) | Cortex, internal capsule → contralateral hemiparesis |
| Lacunar infarct | Internal capsule (posterior limb), pons → pure motor hemiparesis |
| ALS | Both UMN (CST) and LMN (anterior horn) → mixed UMN+LMN signs |
| Multiple sclerosis | White matter (CST anywhere) → spastic paraparesis |
| Spinal cord injury | Below decussation → ipsilateral spastic paralysis |
| Cerebral palsy | CST during development |
| Hereditary spastic paraplegia | Bilateral CST degeneration |
12. Quick Memory Framework
Cortex (Layer V pyramidal neurons, areas 4, 6, 3,1,2, 5, 7)
↓ Corona Radiata
↓ Posterior limb of Internal Capsule ← CRITICAL BOTTLENECK
↓ Cerebral Peduncle (midbrain)
↓ Basilar Pons (broken into bundles)
↓ Medullary Pyramids
↓ PYRAMIDAL DECUSSATION (caudal medulla)
├── 85–90% CROSS → Lateral CST (contralateral lateral funiculus)
└── 10–15% stay → Anterior CST (ipsilateral ventral funiculus, cross later)
↓ Anterior Horn (laminae IV–IX) → α-motor neurons → Skeletal muscle
The golden rule: Lesions above the decussation → contralateral deficits. Lesions below the decussation → ipsilateral deficits.
Sources: Neuroanatomy through Clinical Cases, 3rd ed. (Blumenfeld); Guyton & Hall Textbook of Medical Physiology; Ganong's Review of Medical Physiology, 26th ed.; Localization in Clinical Neurology, 8th ed.; Principles of Neural Science, 6th ed. (Kandel)
This is a shared conversation. Sign in to Orris to start your own chat.