Tracheobronchial tree anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks plus excellent anatomical images. Let me compile a thorough, well-organized answer.
Tracheobronchial Tree Anatomy
The tracheobronchial tree is the conducting airway from the trachea to the terminal bronchioles. It is the lower airway, distinct from the upper airway (nasal cavity, oral cavity, pharynx, larynx).
Respiratory Passages Overview
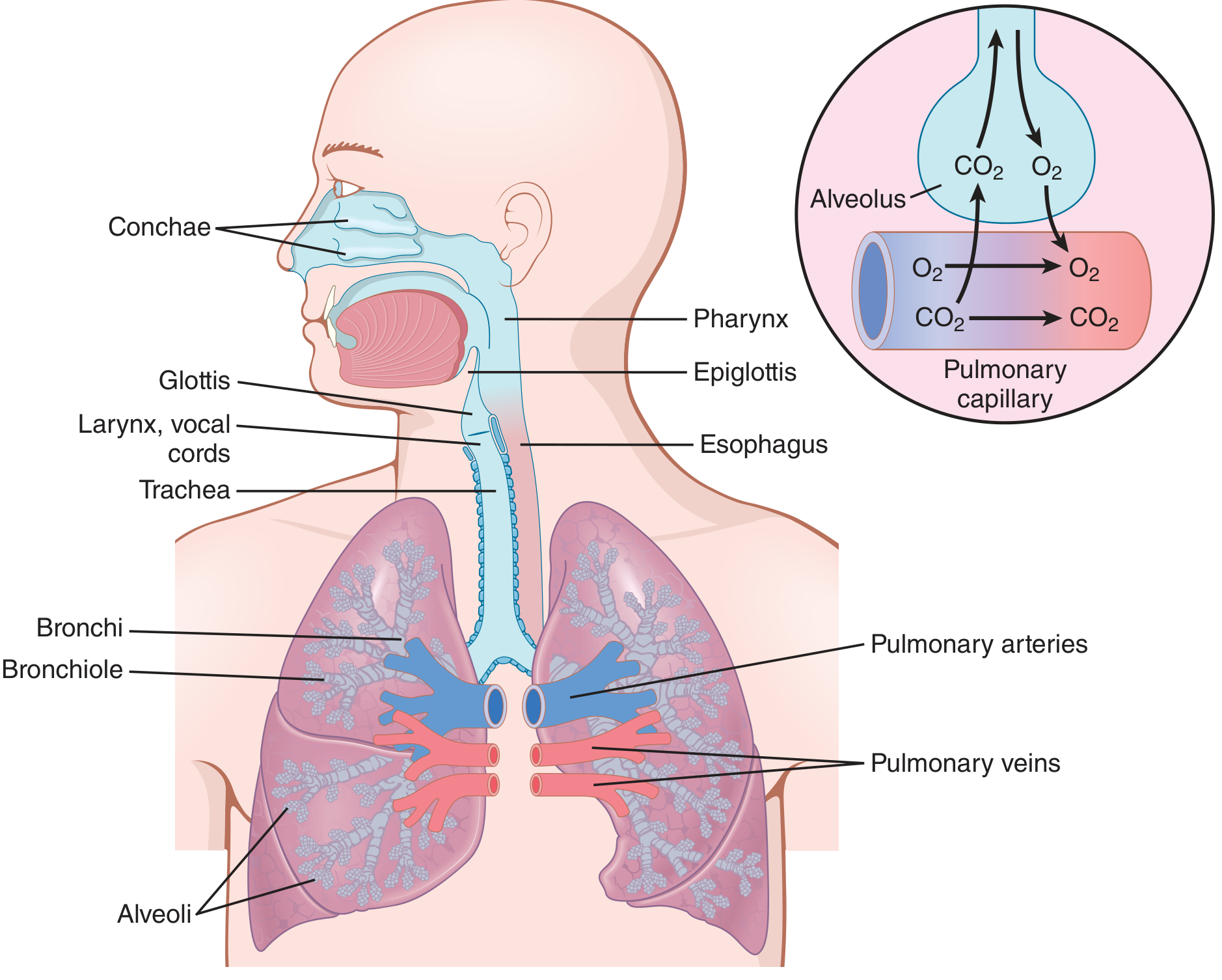
Guyton and Hall Textbook of Medical Physiology, Fig. 38.8 - Respiratory passages
1. Trachea
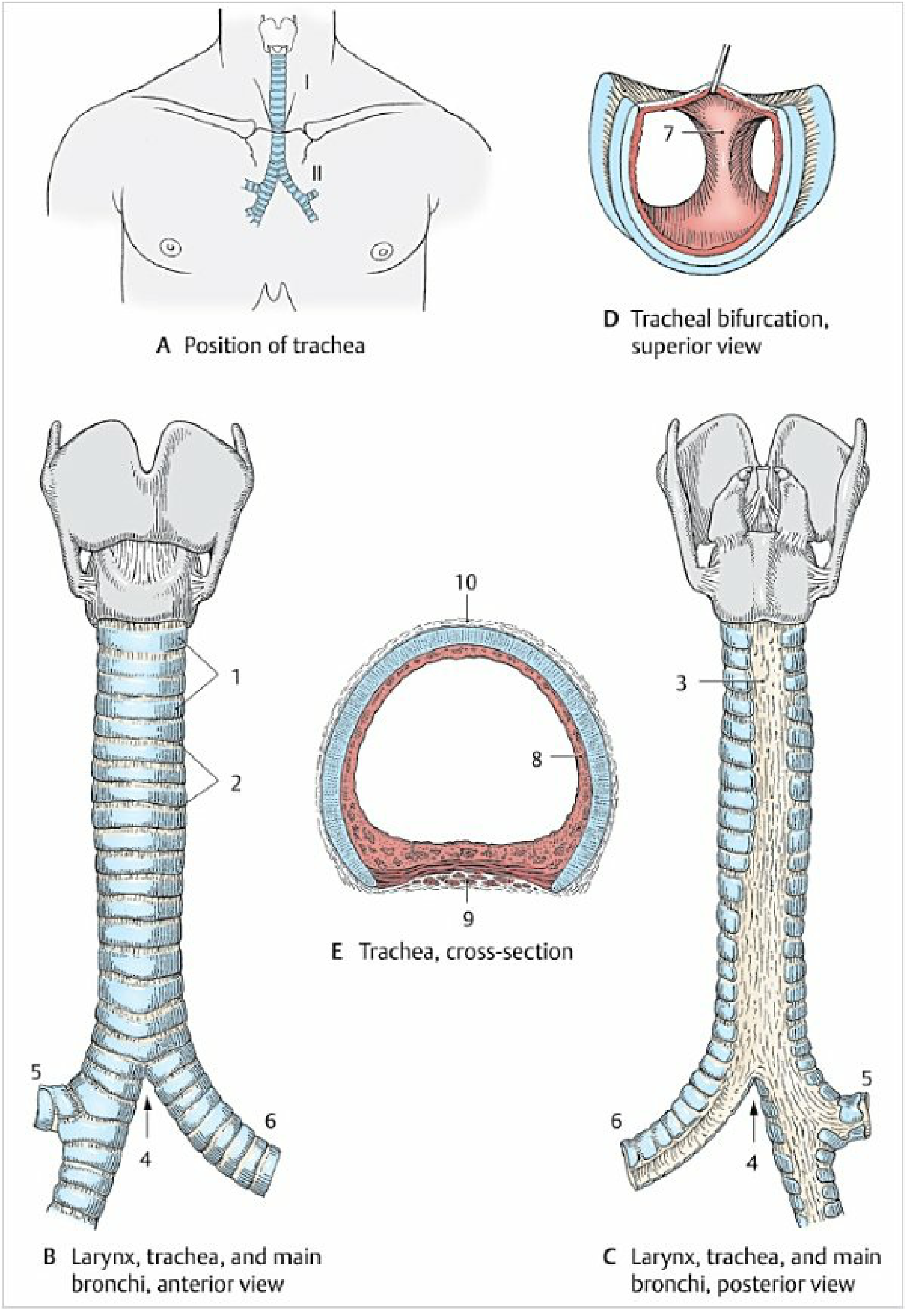
Color Atlas of Human Anatomy, Fig. 3.13 - Trachea and extrapulmonary main bronchi
Position and Extent
- Begins at the cricoid cartilage (C6) and extends to the carina at T4-T5
- Length: 10-15 cm in adults (some sources cite 10-12 cm)
- Divided into a cervical part (C6-C7) and a thoracic part (T1-T4)
- The esophagus lies posterior to the trachea; the thyroid gland lies anterior in the neck
Structure
- 16-20 C-shaped (horseshoe-shaped) hyaline cartilage rings - open posteriorly
- Cartilage rings reinforce the anterior and lateral walls
- Trachealis muscle (smooth muscle): forms the posterior membranous wall - closes the "C"
- Rings connected by annular (fibroelastic) ligaments rich in collagen and elastic fibers
- Transverse diameter > sagittal diameter
Wall Layers (microscopy)
Three concentric layers:
- Mucosa - stratified respiratory (pseudostratified ciliated columnar) epithelium with mixed tracheal glands; mucus and ciliary action = mucociliary clearance
- Fibromuscular-cartilaginous layer - cartilage rings + annular ligaments anterolaterally; trachealis smooth muscle posteriorly
- Adventitia - outer sliding layer
Blood Supply, Nerves, and Lymphatics
- Arterial supply: tracheal branches of the inferior thyroid artery (cervical part); bronchial branches (thoracic part)
- Innervation: recurrent laryngeal nerve (branch of vagus) - motor to trachealis, sensory and secretory innervation
- Lymphatics: drain to paratracheal lymph nodes and superior/inferior tracheobronchial lymph nodes near the carina
2. Carina
- The carina of the trachea is a sagittally oriented cartilaginous ridge projecting into the lumen at the tracheal bifurcation
- It divides the airstream during inspiration
- Located at approximately T4-T5 (angle of Louis / sternal angle level)
- Clinically important: carina is highly sensitive - stimulation triggers the cough reflex; carina widening on CXR suggests subcarinal lymphadenopathy
3. Main (Primary) Bronchi
Right Main Bronchus
- Shorter, wider lumen
- Departs at an angle of only ~20-25° from the tracheal axis (more vertical)
- Continues in nearly the same direction as the trachea
- Consequence: foreign bodies, aspirated material, and malpositioned ETTs preferentially enter the right bronchus
Left Main Bronchus
- Longer, narrower lumen
- Departs at a steeper angle of ~35-45° from tracheal axis
- Must pass under the aortic arch and in front of the esophagus/descending aorta
4. Lobar (Secondary) Bronchi
Each main bronchus divides into lobar bronchi supplying individual lobes:
| Side | Lobar Bronchi |
|---|---|
| Right | Right upper lobe (RUL), right middle lobe (RML), right lower lobe (RLL) |
| Left | Left upper lobe (LUL), left lower lobe (LLL) |
The right lung has 3 lobes separated by the oblique and horizontal fissures. The left has 2 lobes separated by the oblique fissure only (with the lingula as the homologue of the middle lobe).
- The oblique fissures run from T2 posteriorly to the 6th costal cartilage anteriorly
- The horizontal fissure (right lung only) runs along the 4th rib anteriorly
5. Segmental (Tertiary) Bronchi and Bronchopulmonary Segments
Each lobar bronchus divides into segmental bronchi, each supplying a bronchopulmonary segment - the functional unit of the lung (independent arterial supply, can be surgically resected).
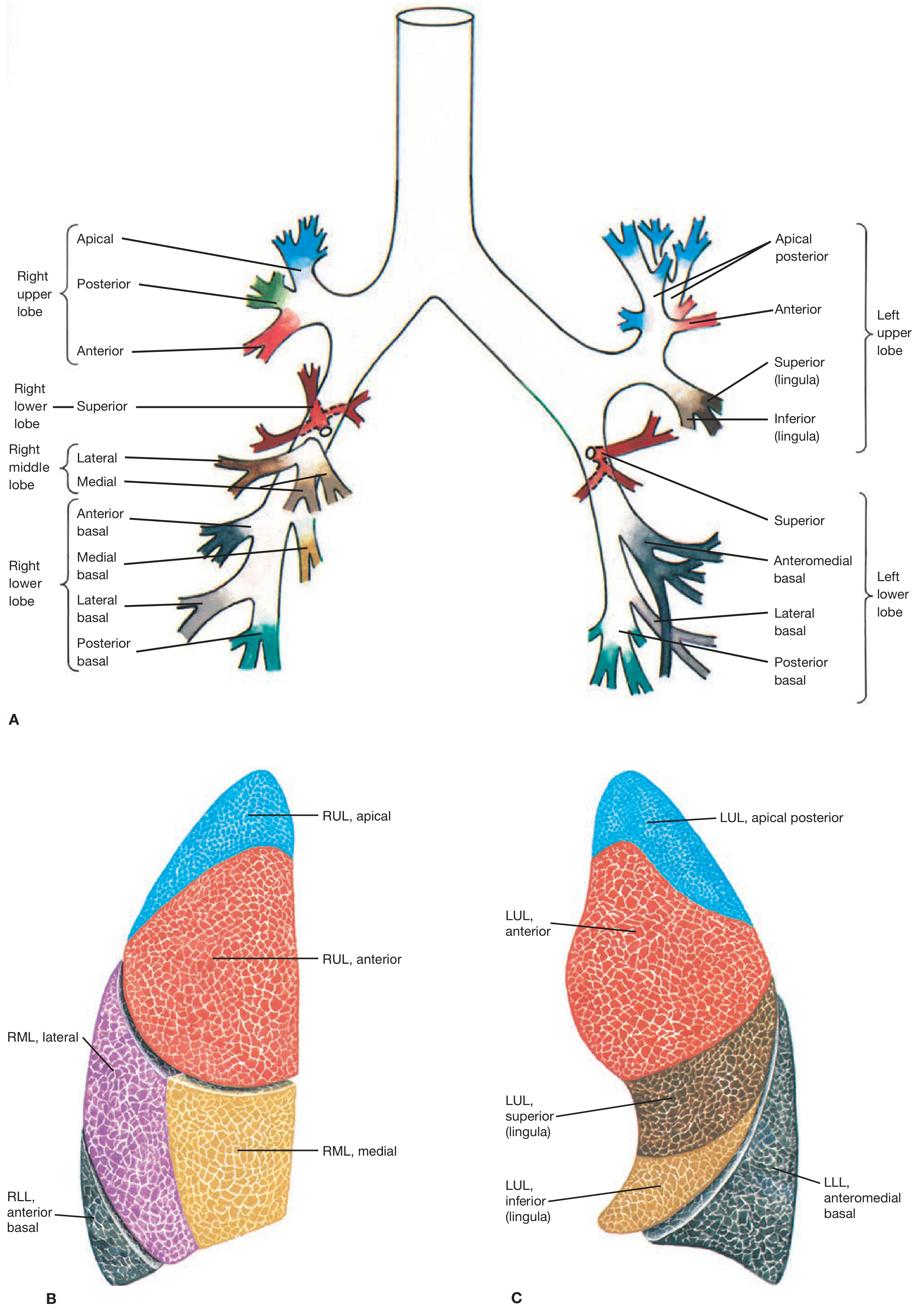
Fishman's Pulmonary Diseases and Disorders, Fig. 28-5 - Topographic anatomy of the tracheobronchial tree and bronchopulmonary segments
Right Lung (10 segments)
| Lobe | Segments |
|---|---|
| RUL | Apical, Posterior, Anterior |
| RML | Lateral, Medial |
| RLL | Superior, Anterior basal, Medial basal, Lateral basal, Posterior basal |
Left Lung (8-10 segments)
| Lobe | Segments |
|---|---|
| LUL | Apical-posterior, Anterior, Superior lingula, Inferior lingula |
| LLL | Superior, Anteromedial basal, Lateral basal, Posterior basal |
(On the left, the apical and posterior segments are fused into apico-posterior; the medial basal and anterior basal often fuse into anteromedial basal - accounting for the 8 vs 10 difference)
6. Bronchioles
Beyond the segmental bronchi, the airway generations continue without cartilaginous support:
| Structure | Key Features |
|---|---|
| Conducting bronchioles | No cartilage; walls almost entirely smooth muscle + elastic tissue |
| Terminal bronchioles | Last purely conducting generation; diameter < 1 mm |
| Respiratory bronchioles | First gas-exchanging generation; alveoli bud from walls |
| Alveolar ducts & sacs | Final gas exchange surfaces |
- Bronchioles (diameter <1.5 mm) lack cartilage and are kept open by transpulmonary pressure - they expand with the alveoli during inspiration
- Their walls are almost entirely smooth muscle (except the respiratory bronchiole, which is mainly pulmonary epithelium)
- This makes them highly susceptible to bronchoconstriction (asthma, COPD)
7. Bronchial Wall - Smooth Muscle and Autonomic Control
- In all areas not occupied by cartilage, the wall is predominantly smooth muscle
- Sympathetic (beta-2): bronchodilation via circulating epinephrine/norepinephrine (direct sympathetic fibers are sparse in the lung)
- Parasympathetic (vagus): bronchoconstriction + mucus secretion
- Local factors: histamine, leukotrienes (bronchoconstriction); CO2, prostaglandins (variable)
8. Airflow Resistance
- Under normal conditions, airflow resistance is low - less than 1 cmH₂O gradient drives quiet breathing
- Counterintuitively, greatest resistance is in the larger bronchi near the trachea, not the small bronchioles, because few large bronchi exist in parallel vs. ~65,000 parallel terminal bronchioles
- In disease, small bronchioles dominate resistance because they are easily occluded by: smooth muscle contraction, mucosal edema, and luminal mucus
9. CT Image of Tracheobronchial Tree
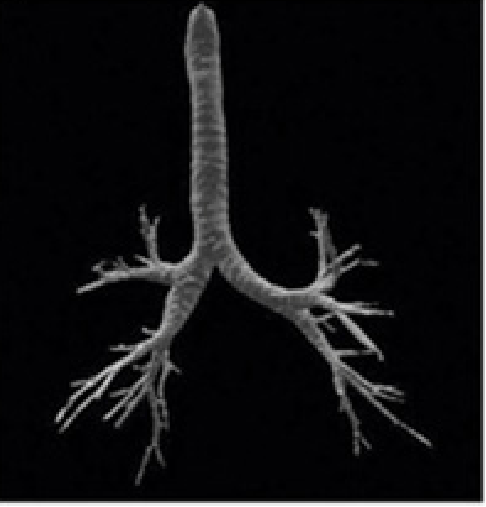
Miller's Anesthesia 10e - Normal tracheobronchial anatomy on CT
Clinical Correlates
| Point | Significance |
|---|---|
| Right bronchus more vertical | Foreign body aspiration, ETT misplacement - both favor right side |
| Carina sensitivity | Intubation trauma at carina = severe bronchospasm; subcarinal nodes widen carina angle on CXR |
| Trachealis muscle | Posterior wall is soft - palpable landmark for flexible bronchoscopy orientation |
| Mucociliary clearance | Disrupted by smoking (squamous metaplasia + cilia paralysis) - impairs innate defense |
| Cricothyroid membrane / tracheostomy | Emergent airway access below the larynx uses these landmarks (cricothyrotomy, high/low tracheostomy) |
| Bronchopulmonary segments | Independent vascular supply allows segmentectomy without affecting adjacent segments |
Sources: Color Atlas of Human Anatomy Vol. 2 (Internal Organs), p. 205-206 | Guyton and Hall Textbook of Medical Physiology | Miller's Anesthesia 10e, p. 5835 | Fishman's Pulmonary Diseases and Disorders | Fischer's Mastery of Surgery 8e
This is a shared conversation. Sign in to Orris to start your own chat.