explain me 10 common heart diseases with ecg changes and ecg changes of those diseases ai orris
Reading File
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram changes common heart diseases
Finding Sources
Finding Sources
Finding Sources
Searching Images
STEMI ST elevation myocardial infarction ECG 12 lead
Finding Sources
Finding Sources
Searching Images
atrial fibrillation ECG irregularly irregular absent P waves
Searching Images
ventricular tachycardia fibrillation ECG wide complex
Searching Images
complete heart block third degree AV block ECG
Searching Images
Wolff-Parkinson-White syndrome delta wave ECG pre-excitation
Searching Images
pericarditis diffuse ST elevation saddle shape ECG
Searching Images
left bundle branch block LBBB ECG QRS morphology
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain
Searching Images
dilated cardiomyopathy heart failure ECG low voltage
I now have comprehensive ECG images and textbook data for all 10 diseases. Let me compile a thorough, well-illustrated response.
10 Common Heart Diseases: ECG Changes
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
Disease: Complete occlusion of a coronary artery → transmural ischemia/infarction. The most time-critical cardiac emergency.
ECG Changes:
| Feature | Finding |
|---|---|
| ST segments | Convex (tombstone) upward ST elevation ≥1 mm in ≥2 contiguous leads |
| Reciprocal changes | ST depression in leads facing the opposite wall |
| Hyperacute T waves | Tall, peaked T waves (very early sign) |
| Q waves | Pathological Q waves develop (>40 ms wide, >25% of R wave height) — indicates necrosis |
| R-wave loss | Progressive loss of R-wave amplitude |
Territorial localization:
- Anterior (LAD): ST elevation in V1–V4
- Inferior (RCA): ST elevation in II, III, aVF; reciprocal depression in I, aVL
- Lateral (LCx): ST elevation in I, aVL, V5–V6
- Posterior: Tall R wave + ST depression in V1–V3 (mirror image)


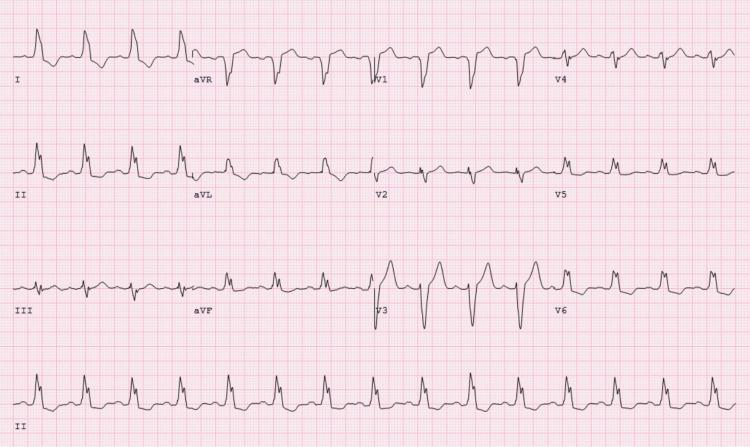
2. 🫀 Atrial Fibrillation (AF)
Disease: Chaotic, disorganized atrial electrical activity (300–600 impulses/min) → irregular ventricular response. Most common sustained arrhythmia.
ECG Changes:
| Feature | Finding |
|---|---|
| P waves | Absent — replaced by irregular fibrillatory (f) waves, best seen in V1 |
| Rhythm | Irregularly irregular R-R intervals (hallmark sign) |
| QRS morphology | Usually narrow (<120 ms) unless aberrant conduction |
| Rate | Ventricular rate varies (often rapid: 100–160 bpm if uncontrolled) |
| Baseline | Chaotic undulating baseline (no identifiable P waves) |
3. 🫀 Complete (Third-Degree) AV Block
Disease: Total failure of conduction from atria to ventricles. Atria and ventricles beat independently. Requires urgent pacing.
ECG Changes:
| Feature | Finding |
|---|---|
| P waves | Present, regular — but bear no relationship to QRS complexes |
| PR interval | Variable (no fixed PR relationship) — AV dissociation |
| QRS complexes | Regular but slow escape rhythm |
| QRS morphology | Narrow (junctional escape, ~40–60 bpm) OR wide (ventricular escape, <40 bpm) |
| Ventricular rate | Bradycardic escape rhythm |
P waves are seen "marching through" QRS complexes and T waves independently.

4. 🫀 Acute Pericarditis
Disease: Inflammation of the pericardium. Usually viral. Chest pain that worsens on lying flat, relieved by leaning forward.
ECG Changes (evolve in 4 stages):
| Feature | Finding |
|---|---|
| ST elevation | Diffuse, concave (saddle-shaped) ST elevation in almost all leads (NOT localized to one territory) |
| PR depression | PR segment depression in most leads — classic distinguishing feature from STEMI |
| aVR | Reciprocal ST depression + PR elevation in aVR |
| Spodick's sign | Downsloping TP segment |
| T waves | Later become inverted (stage 3), then normalize (stage 4) |
Key differentiator from STEMI: diffuse (not territorial), concave (not convex), PR depression, and no reciprocal changes between adjacent leads.

5. 🫀 Pulmonary Embolism (PE)
Disease: Thrombus obstructing pulmonary vasculature → acute right heart strain. ECG changes reflect acute cor pulmonale.
ECG Changes:
| Feature | Finding |
|---|---|
| Sinus tachycardia | Most common ECG finding (~44% of PE cases) |
| S1Q3T3 pattern | Deep S wave in lead I + Q wave in lead III + T-wave inversion in lead III (McGinn-White sign) |
| Right axis deviation | Shift of axis to the right |
| RBBB | Incomplete or complete right bundle branch block (right heart strain) |
| T-wave inversions | V1–V4 (right ventricular strain pattern) |
| P pulmonale | Tall, peaked P waves in II (right atrial strain) |
Note: S1Q3T3 is classic but occurs in only ~20% of PE — sinus tachycardia + T inversions V1–V3 is more common.


6. 🫀 Left Bundle Branch Block (LBBB)
Disease: Delayed/blocked conduction through the left bundle branch → abnormal ventricular depolarization. Often indicates underlying structural heart disease (IHD, cardiomyopathy, hypertension). New LBBB in chest pain = STEMI equivalent until proven otherwise.
ECG Changes:
| Feature | Finding |
|---|---|
| QRS duration | Wide QRS >120 ms |
| V1 | Deep broad S wave (QS or rS pattern) — predominantly negative |
| V5/V6, I, aVL | Broad, notched (M-shaped) monophasic R wave — no septal Q |
| ST/T waves | Discordant — opposite to main QRS deflection (secondary changes) |
| Axis | Often left axis deviation |
| R-wave progression | Loss of normal R-wave progression V1–V3 |
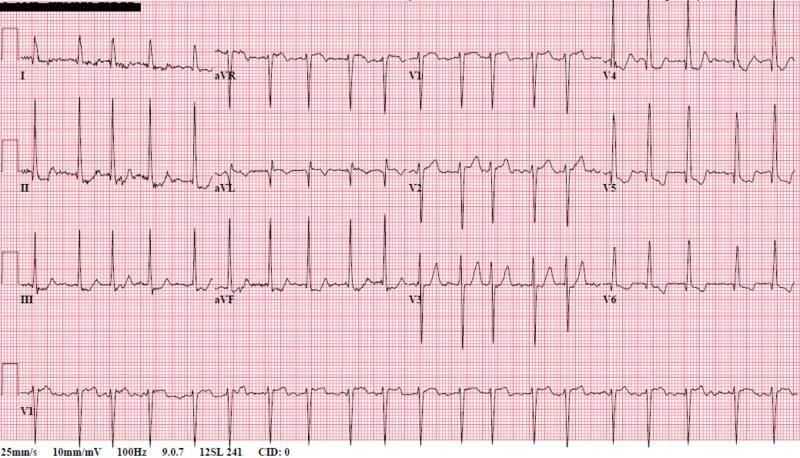
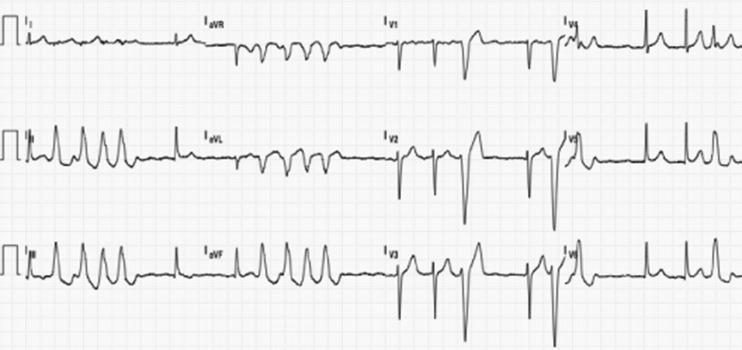
7. 🫀 Wolff-Parkinson-White (WPW) Syndrome
Disease: Accessory pathway (Bundle of Kent) bypasses the AV node → ventricular pre-excitation. Causes paroxysmal SVT and, if AF develops, can cause rapid conduction → ventricular fibrillation.
ECG Changes:
| Feature | Finding |
|---|---|
| PR interval | Short PR <120 ms (accessory pathway bypasses AV node delay) |
| Delta wave | Slurred upstroke at start of QRS (slow conduction via accessory pathway) |
| QRS duration | Widened (>120 ms due to delta wave) |
| ST/T waves | Secondary discordant changes (opposite to delta/QRS direction) |
| Pathway localization | Polarity of delta wave in each lead identifies pathway location |
The pathway location predicts risk: left-sided pathways are lower risk; right-sided/posteroseptal are higher risk.

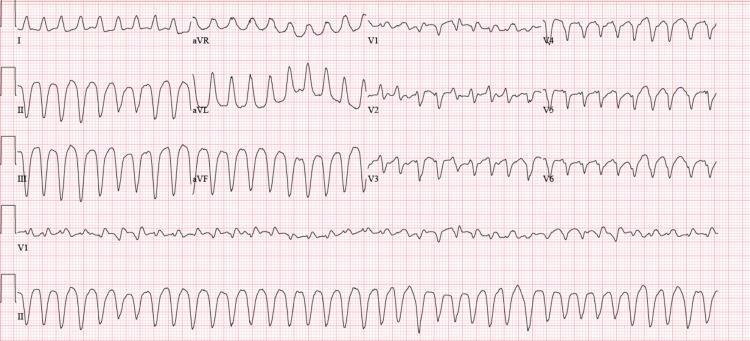
8. 🫀 Ventricular Tachycardia (VT) / Ventricular Fibrillation (VF)
Disease: Life-threatening ventricular arrhythmias. VT: organized rapid ventricular rhythm. VF: chaotic — no effective cardiac output → cardiac arrest.
ECG Changes — Ventricular Tachycardia:
| Feature | Finding |
|---|---|
| Rate | >100 bpm (usually 140–250 bpm) |
| QRS | Wide (>120 ms), bizarre morphology |
| P waves | Usually dissociated (AV dissociation) — key diagnostic sign |
| Fusion beats | Pathognomonic of VT |
| Capture beats | Narrow QRS break — confirms AV dissociation |
| Axis | Often extreme axis deviation ("northwest axis") |
ECG Changes — Ventricular Fibrillation:
| Feature | Finding |
|---|---|
| Rhythm | Chaotic, irregular, rapid deflections |
| QRS | No identifiable QRS complexes — coarse or fine undulating waveform |
| Rate | Indeterminate (300–500/min chaotic) |
Torsades de Pointes (Polymorphic VT):
Twisting of QRS complexes around the isoelectric line — associated with prolonged QT interval.
9. 🫀 Hypertrophic Cardiomyopathy (HCM)
Disease: Genetic disorder (sarcomere mutations) causing asymmetric left ventricular hypertrophy, often with LVOT obstruction. Leading cause of sudden cardiac death in young athletes.
ECG Changes:
| Feature | Finding |
|---|---|
| LVH voltage criteria | Sokolow-Lyon: SV1 + RV5/6 ≥35 mm; Cornell: RaVL + SV3 ≥28 mm (men) |
| Strain pattern | ST depression + T-wave inversion in lateral leads (I, aVL, V4–V6) — "LV strain" |
| Deep Q waves | Pathological Q waves in lateral/inferior leads (II, III, aVF, V4–V6) — from asymmetric septal hypertrophy |
| Left axis deviation | Common |
| P wave | Left atrial enlargement (bifid P wave in II, deep negative in V1) |
| Giant T-wave inversions | Apical HCM (Yamaguchi variant) — massive T-wave inversions V3–V6 |
The combination of LVH + deep lateral Q waves in a young patient should raise suspicion for HCM.
10. 🫀 Dilated Cardiomyopathy (DCM) / Congestive Heart Failure
Disease: Enlarged, poorly contracting LV → reduced ejection fraction. Multiple causes (ischemic, viral, alcohol, idiopathic). ECG findings are non-specific but reflect remodeling.
ECG Changes:
| Feature | Finding |
|---|---|
| LBBB | Common — ventricular remodeling disrupts conduction (present in ~25% DCM) |
| Low voltage | QRS amplitude <5 mm limb leads / <10 mm precordial leads (especially with effusion or amyloid) |
| Sinus tachycardia | Compensatory sympathetic activation |
| LVH criteria | May be present if significant hypertrophy |
| Q waves / poor R progression | Simulating prior MI (pseudoinfarct pattern) in anterior leads |
| AF | Common comorbid arrhythmia |
| ST/T changes | Non-specific ST depression, T-wave inversions in lateral leads |
Quick Reference Summary Table
| Disease | Key ECG Finding | Classic Sign |
|---|---|---|
| STEMI | Convex ST elevation, Q waves, reciprocal depression | Tombstone ST elevation |
| Atrial Fibrillation | Absent P waves, irregularly irregular | Fibrillatory baseline |
| Complete AV Block | AV dissociation, P waves march through QRS | "Marching P waves" |
| Acute Pericarditis | Diffuse concave ST elevation, PR depression | Saddle-shaped ST + PR dip |
| Pulmonary Embolism | S1Q3T3, sinus tachycardia, RBBB | McGinn-White sign |
| LBBB | Wide QRS, deep S in V1, notched R in V5–V6 | Discordant ST/T waves |
| WPW Syndrome | Short PR, delta wave, wide QRS | Delta wave pre-excitation |
| VT / VF | Wide complex tachycardia / chaotic waveform | AV dissociation / no QRS |
| HCM | LVH + deep lateral Q waves, strain pattern | Young patient + Q waves |
| DCM / Heart Failure | LBBB, low voltage, non-specific ST changes | Poor R progression |
Sources: Braunwald's Heart Disease, Harrison's Principles of Internal Medicine 22E, ROSEN's Emergency Medicine, Tintinalli's Emergency Medicine, Goldman-Cecil Medicine, Guyton & Hall Medical Physiology, Robbins Basic Pathology.
This is a shared conversation. Sign in to Orris to start your own chat.