radial no compression at the forarm in lateral sidehow to treatment because of fat small nodule in middle of brachioradialis muscle
Reading File
Finding Sources
Finding Sources
Searching PubMed
radial nerve lipoma brachioradialis treatment
Reading File
Reading File
Searching PubMed
radial nerve lipoma forearm compression treatment
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive answer synthesizing the textbook and literature findings:
Radial Nerve - No True Compression at Lateral Forearm: Small Fat Nodule (Lipoma) in Brachioradialis
Anatomy Overview
The brachioradialis is the most lateral muscle of the forearm, forming the "mobile wad" compartment along with the extensor carpi radialis longus and brevis. It originates from the lateral supracondylar ridge of the humerus and is supplied by branches of the radial nerve BEFORE the nerve divides into its deep (posterior interosseous nerve, PIN) and superficial branches.
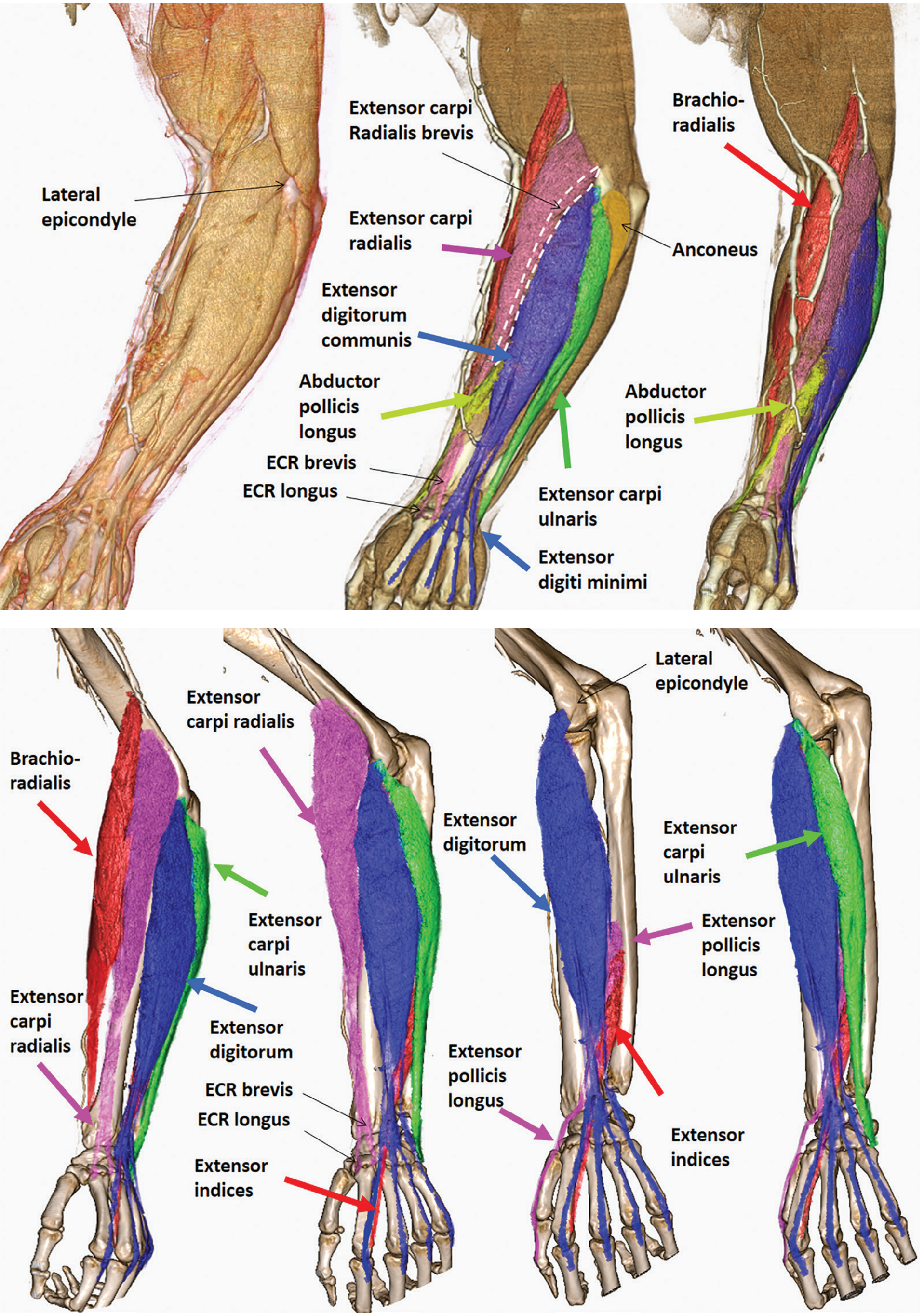
The radial nerve courses past the brachioradialis, and radial nerve compression at the humeral origin of the brachioradialis has been reported (though rare). More commonly, radial nerve entrapment in the forearm occurs at the arcade of Frohse near the supinator origin (radial tunnel), not within the brachioradialis belly itself.
- Imaging Anatomy Text and Atlas Vol. 3, p. 131
The Specific Situation: Fat Nodule (Lipoma) in Brachioradialis with No True Nerve Compression
This is an intramuscular lipoma - a benign fatty tumor within the brachioradialis muscle belly - that is causing symptoms in the lateral forearm distribution of the radial nerve WITHOUT confirmed electrodiagnostic nerve compression. Lipomas are listed among the causes of radial nerve irritation in the forearm.
"Other sources of compression that can injure the radial nerve along its course include lipoma, fibroma, and new or previous (from callus) humerus fracture." - Textbook of Family Medicine 9e
Literature also documents cases of posterior interosseous nerve syndrome caused by an intermuscular lipoma (PMID: 4015361) and delayed-diagnosed intermuscular lipomas causing PIN palsy (PMID: 27142825).
Symptoms to Expect
Depending on which radial nerve branch is affected by proximity to the lipoma:
| Branch | Symptoms |
|---|---|
| Superficial branch (SBRN) | Pain, numbness, paresthesias over dorso-radial hand/thumb, no motor loss |
| Posterior interosseous nerve (PIN) | Weakness of finger/wrist extension, radial forearm pain |
| Radial tunnel (local irritation) | Lateral elbow/radial forearm pain, point of max tenderness several cm distal to lateral epicondyle |
Since you state there is no true compression (presumably normal or near-normal electrodiagnostics), the picture is more consistent with local irritation from the mass rather than axonotmesis.
Treatment
Step 1 - Conservative (First-line, if symptoms are mild)
- Activity modification - avoid repetitive forearm pronation/supination and gripping
- NSAIDs (ibuprofen 400-600 mg TID or naproxen 500 mg BID) for pain/inflammation
- Splinting - a neutral wrist/forearm splint for 4-6 weeks to offload irritation
- Physical therapy - gentle stretching of the lateral forearm, ergonomic correction
- Observation - small, asymptomatic lipomas can be watched; many remain stable for years
Step 2 - Surgical Excision (Definitive, if symptomatic or growing)
- Miller's Review of Orthopaedics is direct: "If the mass is growing or causing symptoms, excision with a marginal resection performed."
- For intramuscular lipomas, marginal (shell-out) excision through a longitudinal forearm incision is standard
- The radial nerve and its branches must be identified and protected intraoperatively
- In the reported cases of lipoma-induced PIN palsy, surgical removal of the lipoma led to nerve recovery
Surgical decompression of anatomic radial nerve sites provides good to excellent results in 85% of patients (PIN syndrome); results for radial tunnel pain are good-to-excellent in 50-80% cases.
- Miller's Review of Orthopaedics 9th Ed.
Step 3 - Pre-op Workup Before Surgery
- MRI of the forearm - confirms lipoma vs. liposarcoma; lipoma shows uniformly low signal on fat-suppression sequences, well-demarcated from surrounding muscle. If the lesion is heterogeneous, atypical, or >5 cm, consider liposarcoma and biopsy before excision.
- EMG/Nerve conduction studies - baseline documentation even if currently normal; if abnormal, aids surgical planning and prognosis
- Ultrasound - cost-effective initial imaging; shows echogenic fatty mass within muscle
Key Points Summary
| Issue | Management |
|---|---|
| Small, asymptomatic lipoma | Watch and wait, no treatment needed |
| Mild symptoms (pain/paresthesias) | NSAIDs, splinting, activity modification x 3-6 months |
| Growing or persistent symptoms | MRI confirmation, then surgical marginal excision |
| True nerve palsy (motor loss) | Urgent MRI + surgical decompression + lipoma excision |
| Suspected malignancy (atypical MRI) | Core needle biopsy before excision |
The key principle: the lipoma itself is the problem, not an external compressive structure, so if conservative measures fail, removing the lipoma resolves the nerve irritation without need for separate nerve decompression in most cases.
Sources:
- Imaging Anatomy Text and Atlas Vol. 3 (Bones, Joints, Vessels and Nerves), p. 130-131
- Miller's Review of Orthopaedics 9th Ed., Lipomas section and Radial Nerve section
- Sabiston Textbook of Surgery 11th Ed., Radial Nerve Compression
- Textbook of Family Medicine 9e, Median/Radial Neuropathy chapter
- PMID: 4015361 - Posterior interosseous nerve syndrome caused by intermuscular lipoma
- PMID: 27142825 - Delayed-diagnosed intermuscular lipoma causing PIN palsy
I am physiotherapy 2nd year student
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
radial nerve physiotherapy rehabilitation exercise
Reading File
Finding Sources
Searching PubMed
neural mobilization neurodynamics peripheral nerve entrapment upper limb
Reading File
Finding Sources
Finding Sources
I now have enough high-quality textbook content to build a thorough, student-appropriate physiotherapy treatment plan. Here it is:
Physiotherapy Treatment Plan
Radial Nerve Irritation - Small Intramuscular Lipoma in Brachioradialis (No True Compression, Lateral Forearm)
Tailored for a 2nd-year physiotherapy student
First - Understand the Clinical Picture
Before treating, you need to know which structure of the radial nerve is affected. The radial nerve divides in the forearm into:
| Branch | Type | Supplies |
|---|---|---|
| Superficial Radial Nerve (SBRN) | Sensory only | Dorsoradial hand, thumb, index, middle finger dorsum |
| Posterior Interosseous Nerve (PIN) | Motor only | All wrist/finger extensors (except ECRL, brachioradialis) |
| Radial Tunnel | Combined area | Source of pain without weakness |
Since there is no true compression (your case), the lipoma in the brachioradialis belly is causing local irritation rather than axonal damage. This means your PT goals are to:
- Reduce pain and irritation around the nerve
- Maintain/restore full movement
- Prevent progression to actual compression
- Address the underlying mass (liaison with surgeon if needed)
Phase 1 - Acute/Protective Phase (Weeks 1-3)
Goal: Reduce irritation, protect the nerve
1. Splinting
- Apply a cock-up wrist splint (wrist neutral to 20-30° extension) to rest the forearm extensors and reduce mechanical stress on the brachioradialis/radial nerve territory
- Wear during activity and at night initially; wean off as symptoms settle
- This is standard first-line for radial nerve irritation - Miller's Review of Orthopaedics 9th Ed.
2. Activity Modification
- Avoid repeated pronation/supination of the forearm (these stretch and compress the radial nerve through the brachioradialis)
- Avoid forceful gripping and resisted wrist extension
- Ergonomic advice - keyboard/mouse posture, lifting technique
3. Pain Management Modalities
- TENS (Transcutaneous Electrical Nerve Stimulation): Place electrodes along the lateral forearm/radial nerve distribution for pain gate effect
- Therapeutic Ultrasound: Over the brachioradialis belly (1 MHz, pulsed mode 1:4, 0.5-1.0 W/cm² for 5-7 min) to reduce local inflammation around the lipoma without heating it excessively
- Cryotherapy: Ice pack to lateral forearm 10-15 min after activity if acutely tender
- NSAIDs (as prescribed by the doctor - your role is to reinforce compliance)
Phase 2 - Sub-acute/Recovery Phase (Weeks 3-8)
Goal: Restore nerve mobility, improve muscle function
4. Neural Mobilization (Neurodynamics) - KEY PT TECHNIQUE
This is one of the most important physiotherapy contributions for nerve irritation. The goal is to restore the nerve's ability to slide and glide freely within its tissue bed.
Radial Nerve Neurodynamic Test/Slider (Upper Limb Tension Test 2b - ULTT2b):
- Patient sitting or supine
- Depress the shoulder girdle
- Extend the elbow fully
- Pronate the forearm
- Flex the wrist and fingers
- Internally rotate the shoulder
- This loads the radial nerve; use this as BOTH an assessment AND treatment tool
Technique options:
- Slider (gentler, early phase): Move one end of the nerve while slackening the other (e.g., flex wrist + release shoulder depression simultaneously). 10-15 reps, 2-3 sets.
- Tensioner (later phase): Move both ends to tension the nerve. Use only when sliders are well tolerated.
Evidence: Neuromobilization techniques have been shown to reduce pain in lateral elbow/forearm entrapment conditions (PMID: 33563509 - RCT on neuromobilization in lateral epicondylitis, 2022, J Hand Ther)
5. Gentle Stretching
- Brachioradialis stretch: Elbow extended, forearm pronated, wrist flexed + ulnar deviated. Hold 30 seconds, 3 reps. This gently elongates the muscle around the lipoma without aggressive compression.
- Forearm flexor/extensor balance stretches
6. Soft Tissue Techniques
- Gentle transverse frictions around (not directly over) the lipoma nodule to improve tissue mobility
- Myofascial release of the lateral forearm and mobile wad muscles
Phase 3 - Strengthening & Return to Function (Weeks 6-12)
Goal: Full strength, prevent recurrence
7. Progressive Strengthening
Start with low resistance, high reps and progress gradually:
| Exercise | Purpose |
|---|---|
| Wrist extension with light theraband | Strengthen ECRL/ECRB, brachioradialis |
| Forearm supination/pronation with stick | Restore pronation-supination range |
| Grip strengthening (putty/ball squeezes) | Overall hand/forearm endurance |
| Wrist radial/ulnar deviation | Balance lateral vs. medial forearm |
- Progress from gravity-eliminated → against gravity → resistance band → functional activities
- Monitor for symptom reproduction - if symptoms increase, step back one level
8. Proprioception & Function
- Fine motor coordination exercises (picking up objects, writing)
- Sport/occupation-specific retraining in the final stage
When to Refer Back / Red Flags
As a physiotherapy student, know when PT alone is NOT enough:
| Red Flag | Action |
|---|---|
| Lipoma growing rapidly | Refer for MRI - rule out liposarcoma |
| Wrist/finger drop develops (motor loss) | Urgent ortho/neuro referral - surgical decompression needed |
| Progressive weakness after 3 months of PT | Review - surgical lipoma excision may be needed |
| No improvement after 6 months | Escalate management |
| Abnormal EMG/NCS findings | Confirms nerve damage; surgical planning required |
"If the mass is growing or causing symptoms, excision with marginal resection [is the treatment]." - Miller's Review of Orthopaedics 9th Ed.
Summary for Your Notes
PHASE 1 (0-3 wks): Splint + activity mod + TENS/US + ice
PHASE 2 (3-8 wks): Neural mobilization (ULTT2b sliders)
+ brachioradialis stretching + soft tissue
PHASE 3 (6-12 wks): Progressive strengthening (theraband)
+ proprioception + return to function
THROUGHOUT: Monitor for red flags - refer if motor loss, growth, or no improvement
Key textbook sources used:
- Bradley and Daroff's Neurology in Clinical Practice - Radial Nerve section
- Miller's Review of Orthopaedics 9th Ed. - Radial nerve/Lipoma sections
- Sabiston Textbook of Surgery 11th Ed. - Radial Nerve Compression
Create a PT assessment checklist for radial nerve testing
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.