Bedside Pulmonary function tests
Reading File
Finding Sources
Finding Sources
Searching PubMed
bedside pulmonary function tests
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive information to write a thorough answer. Let me compile it:
Bedside Pulmonary Function Tests (PFTs)
Bedside pulmonary function tests are simple, portable assessments of respiratory mechanics that can be performed at the patient's bedside without requiring specialized laboratory facilities. They range from handheld peak-flow meters to spirometers, and their clinical role spans the emergency department, ward, and neurology settings.
1. Why Bedside PFTs Matter
Physical examination and history have wide variability in accurately detecting airflow obstruction. A significant proportion of patients with marked airflow obstruction present without dyspnea, and patients may report subjective improvement after therapy even when severe obstruction persists. Objective measurement fills this gap. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
2. Key Bedside Tests
A. Peak Expiratory Flow Rate (PEFR)
-
Device: Mini-Wright peak-flow meter (or similar handheld gauge)
-
What it measures: Maximum airflow velocity achieved during a forced expiration from total lung capacity
-
How to perform: Patient stands or sits upright, extends the neck slightly, takes a maximal inspiration, seals lips around mouthpiece, then performs a rapid and forceful expiration. Obtain 3 measurements and record the best.
-
Key feature: Effort-dependent - pain from abdominal or thoracic wounds can falsely lower values
-
Clinical uses: Monitoring asthma severity, guiding treatment response, and follow-up
-
Limitations: PEFR alone cannot make accurate clinical decisions on admission or discharge - trends are more important than individual values since individual baselines vary widely
-
Bailey and Love's Short Practice of Surgery, Roberts and Hedges' Clinical Procedures in Emergency Medicine
B. Spirometry (Bedside / Handheld)
Small handheld devices allow convenient spirometric evaluation at the bedside and in the ED.
Key parameters:
| Parameter | Definition | Normal Values |
|---|---|---|
| FVC (Forced Vital Capacity) | Total volume exhaled during a forced expiratory maneuver | Male: ~4.8 L, Female: ~3.7 L |
| FEV₁ (Forced Expiratory Volume in 1s) | Volume forcibly expired in the first second | Male: ~3.0-4.0 L, Female: ~2.5-3.0 L |
| FEV₁/FVC ratio | Proportion of FVC expelled in 1 second | >70% (normal) |
| PEFR | Max flow during forced expiration | Effort-dependent |
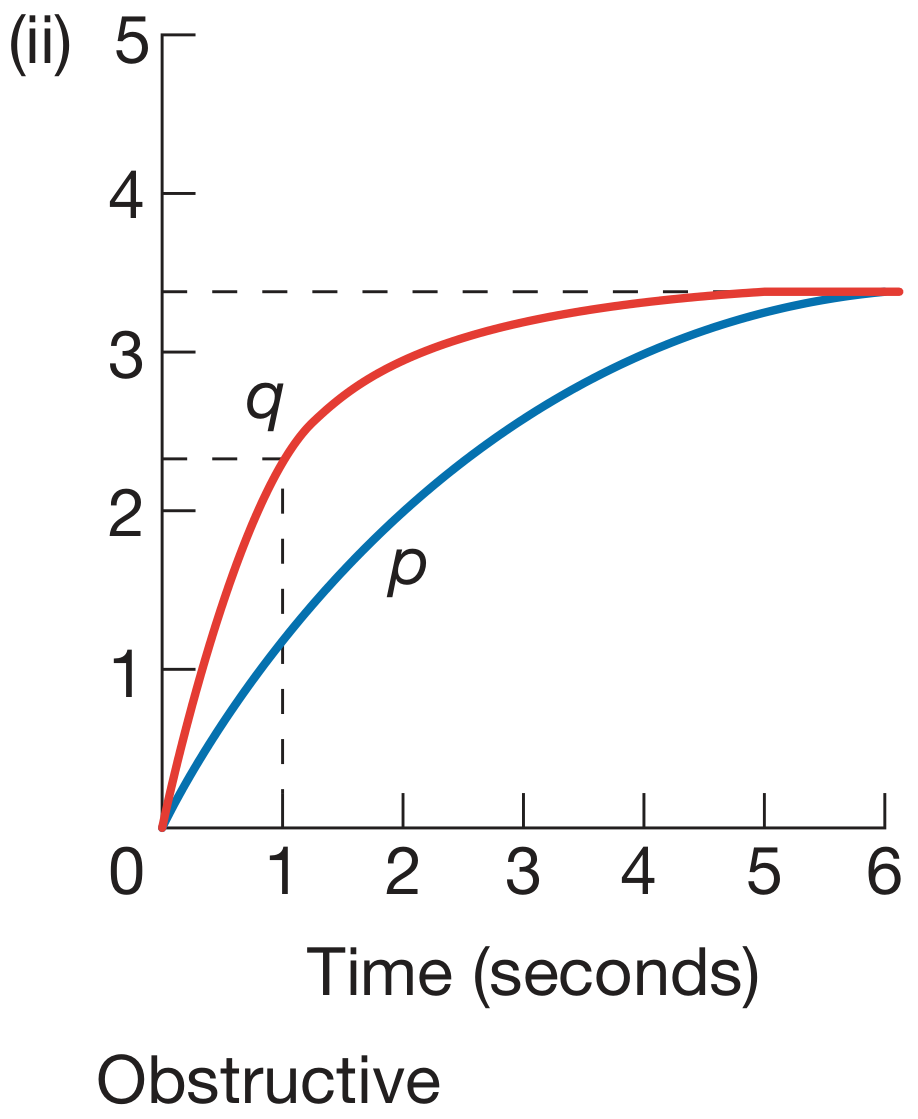
Interpreting patterns:
| Finding | Obstructive Pattern | Restrictive Pattern |
|---|---|---|
| PEFR | Markedly decreased (↓↓) | Normal or mildly decreased |
| FEV₁ | Markedly decreased (↓↓) | Normal or mildly decreased |
| FVC | Normal or mildly decreased | Markedly decreased (↓↓) |
| FEV₁/FVC | < 70% | > 80% |
- Bailey and Love's Short Practice of Surgery, p. 998-999
Obstructive diseases: Asthma, COPD, emphysema - airflow in/out of lungs is impaired
Restrictive diseases: Pulmonary fibrosis, chest wall disease - lungs lose size/elasticity and become stiff
Spirometry is the most commonly performed PFT. Normal values vary with gender, race, age, and height.
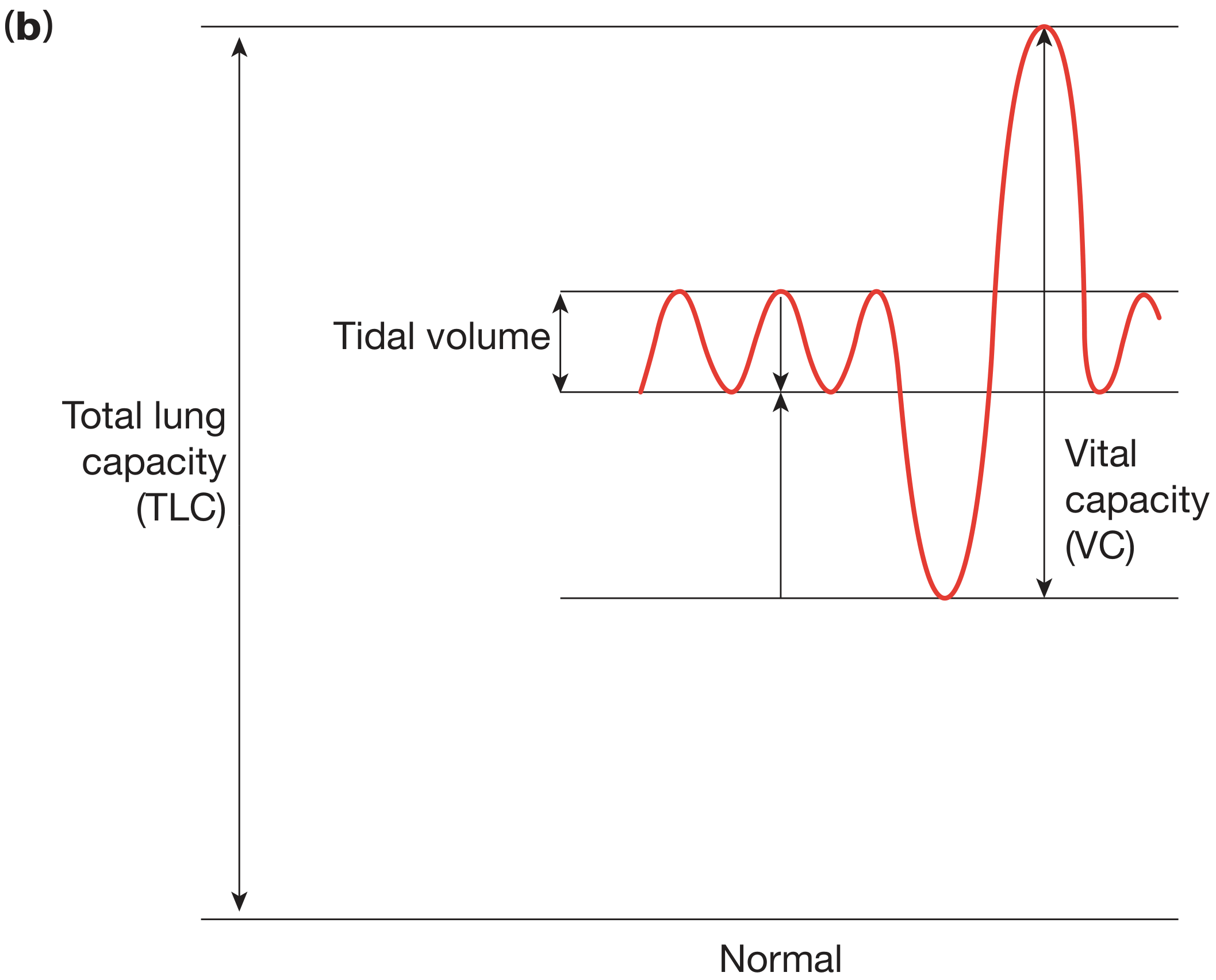
C. Vital Capacity (VC) - Bedside
- The slow vital capacity can be measured at the bedside with a simple spirometer
- Normal: >3.5 L in adult females, >4.5 L in adult males
- Particularly important in neuromuscular disease monitoring
D. Negative Inspiratory Force (NIF) / Maximum Inspiratory Pressure (MIP)
- Measures inspiratory muscle strength
- Normal: More negative than -80 cm H₂O (i.e., the patient can generate -80 or greater)
- Performed by occluding the airway at functional residual capacity and measuring maximal inspiratory effort
3. Special Use: Neuromuscular Disease Monitoring ("20/30 Rule")
In conditions like Guillain-Barré syndrome (GBS) or myasthenia gravis, bedside VC and NIF are the most important serial measurements to detect impending respiratory failure:
The "20/30 Rule" - Intubation is indicated when:
- FVC < 20 mL/kg (approximately 1.5 L in an average adult), OR
- NIF > -30 cm H₂O (i.e., less than 30 cm H₂O of negative pressure)
These parameters are more sensitive for impending respiratory failure than hypoxia, dyspnea, or acidosis - which often appear late. The threshold for elective intubation should be kept low.
Quick bedside substitute (if NIF/FVC unavailable): Ask the patient to count numbers on one breath. Each number ≈ 100 mL of VC (count to 10 = approximately 1 L VC).
- Washington Manual of Medical Therapeutics; Neuroanatomy through Clinical Cases
4. Indications for Bedside PFTs
| Clinical Scenario | Recommended Test | Purpose |
|---|---|---|
| Acute asthma exacerbation | PEFR (at arrival, after treatment, and periodically) | Quantify severity, guide discharge |
| COPD exacerbation | PEFR / spirometry (not routinely recommended by consensus guidelines) | Objective airflow data |
| Differentiating COPD vs CHF | PEFR (insufficient data for routine use) | Adjunctive tool |
| Neuromuscular/chest wall disease | VC + NIF (serially) | Detect impending respiratory failure |
5. Contraindications
- Active severe respiratory compromise - do not delay therapy for testing
- Pneumothorax / pneumomediastinum - forced expiratory maneuvers raise intrathoracic pressure and may worsen
- Aortic or cerebral aneurysm - elevated pressures from forced expiration are a relative contraindication
- Formal PFTs have limited value for acute exacerbations and are most predictive at baseline functional status
6. What Bedside Tests Cannot Do
- DLCO (Diffusing Capacity) - requires specialist equipment; cannot be performed at the bedside. It measures the lung's ability to transfer gases and is important in emphysema, fibrosis, and pre-surgical lung resection assessment.
- Blood gases (CO₂, pH, bicarbonate) - require arterial sampling; pulse oximetry only measures oxygenation, not ventilation.
Summary Table
| Test | Device | Effort-dependent | Bedside Feasible | Primary Use |
|---|---|---|---|---|
| PEFR | Mini-Wright meter | Yes | Yes | Asthma monitoring |
| FEV₁ / FVC | Handheld spirometer | Yes | Yes | Obstructive vs restrictive |
| Vital Capacity | Simple spirometer | Moderate | Yes | Neuromuscular disease |
| NIF / MIP | Pressure gauge | Yes | Yes | Neuromuscular disease |
| DLCO | Lab equipment | No | No | Gas exchange, pre-op |
| Pulse oximetry | Pulse oximeter | No | Yes | Oxygenation only |
Sources: Bailey and Love's Short Practice of Surgery 28th Ed. | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Washington Manual of Medical Therapeutics | Neuroanatomy through Clinical Cases 3rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.