Content rupture in mi
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough answer. Let me compile it.
Cardiac Rupture (Content Rupture) Complicating Myocardial Infarction
Rupture of cardiac structures is one of the most feared mechanical complications of acute MI, complicating 1-5% of all MIs and carrying high mortality. There are three distinct types, each involving a different anatomical structure.
Pathological Basis
Rupture occurs most often 3-7 days after MI - the period when lysis of necrotic myocardium is maximal and the infarct has been converted to soft, friable granulation tissue. At this point the structural integrity of the myocardial wall is at its weakest.
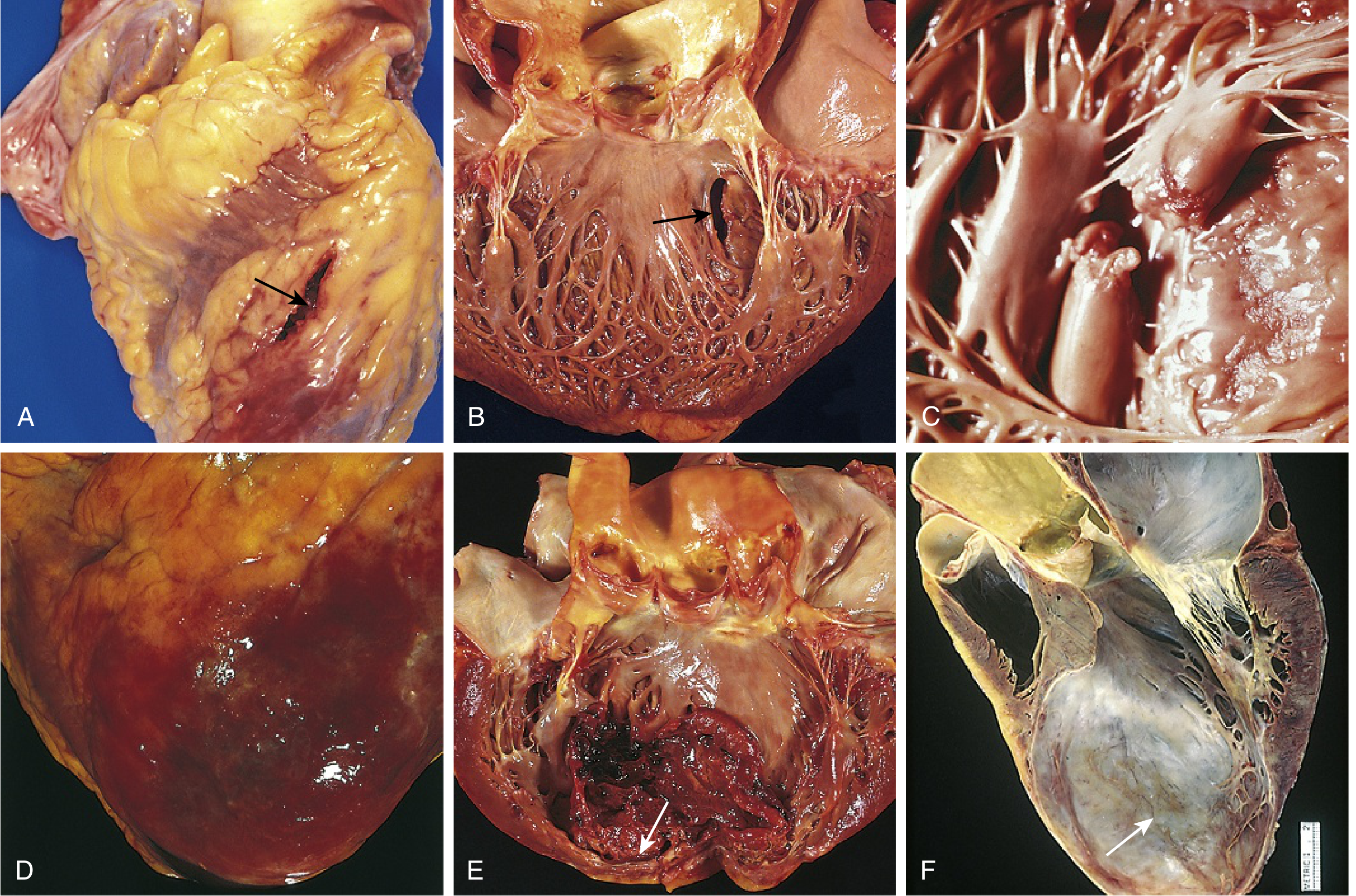
FIG. 9.14 - Robbins & Kumar Basic Pathology: Gross pathological specimens showing the spectrum of cardiac rupture and complications after MI.
Three Types of Cardiac Rupture
1. Ventricular Free Wall Rupture
- Frequency: Least common of the three rupture types, but the most lethal. Accounts for ~10% of AMI fatalities.
- Timing: Usually 1-5 days after infarction.
- Mechanism: Transmural infarction of the left ventricular free wall leads to perforation - blood enters the pericardial space (hemopericardium) causing cardiac tamponade.
- Clinical features: Sudden tearing pain, rapid hemodynamic collapse - hypotension, tachycardia, elevated JVP, muffled heart sounds, pulsus paradoxus (Beck's triad).
- Diagnosis: Echocardiography is the test of choice in the ED; pulmonary artery catheterization shows near-equalization of right atrial, RV mid-diastolic, and RV systolic pressures.
- Outcome: Fatal in >90% of cases.
- Treatment: Emergency surgical repair.
2. Ventricular Septal Rupture (Post-MI VSD)
- Frequency: Most common of the three rupture types (though more often detected clinically than free wall rupture).
- Associated infarct: More common with anterior wall MI and extensive three-vessel coronary artery disease.
- Mechanism: Septal perforation creates a left-to-right shunt (VSD), leading to right heart volume overload and pulmonary edema.
- Clinical features: Chest pain, dyspnea, sudden new holosystolic murmur best heard at the lower left sternal border, often with a palpable thrill.
- Diagnosis:
- Doppler echocardiography (procedure of choice)
- Pulmonary artery catheter: O₂ step-up >10% from right atrium to right ventricle is diagnostic
- Treatment: Surgical. The size of the defect determines the degree of left-to-right shunt and overall prognosis.
3. Papillary Muscle Rupture
- Frequency: ~1% of AMI patients. Follows ventricular septal rupture in frequency.
- Associated infarct: More common with inferior MI; typically with a small- to modest-sized infarct (unlike free wall/septal rupture).
- Timing: Usually 3-5 days after AMI.
- Mechanism: The posteromedial papillary muscle is most commonly ruptured because it has a single blood supply (usually from the right coronary artery), making it vulnerable. The anterolateral papillary muscle has dual supply and is affected 6-10 times less frequently. Rupture causes acute severe mitral regurgitation.
- Clinical features: Acute onset dyspnea, pulmonary edema, new holosystolic murmur of MR (distinguished from VSD murmur - VSD has thrill at left sternal border, papillary muscle rupture murmur may radiate differently).
- Diagnosis: Echocardiography (can distinguish partial papillary muscle rupture from other causes of MR).
- Treatment: Surgical (mitral valve repair or replacement). Intra-aortic balloon pump as bridge.
Summary Comparison
| Feature | Free Wall Rupture | Septal Rupture | Papillary Muscle Rupture |
|---|---|---|---|
| Frequency (of 3 types) | Least common | Most common | Intermediate |
| Associated MI | Transmural, anterior | Anterior, 3-vessel disease | Inferior |
| Timing | 1-5 days | 3-7 days | 3-5 days |
| Result | Hemopericardium + tamponade | Left-to-right shunt (VSD) | Acute severe MR |
| Murmur | None (tamponade) | Holosystolic + thrill, LLSB | Holosystolic MR (no thrill) |
| Key diagnosis | Echo, pulsus paradoxus | Echo, O₂ step-up on cath | Echo |
| Mortality if untreated | >90% | High | High |
| Treatment | Emergency surgery | Surgery | Surgery ± IABP |
Key Points
- All three forms represent mechanical complications of MI caused by rupture of infarcted tissue.
- The window of highest risk is 3-7 days post-MI, when enzymatic lysis peaks.
- Early reperfusion therapy (PCI) has significantly reduced the incidence of all rupture complications.
- Echocardiography is the cornerstone of rapid diagnosis for all three.
- All require surgical intervention - medical therapy alone is insufficient.
Sources: Robbins & Kumar Basic Pathology, p. 360; Tintinalli's Emergency Medicine, p. 3748-3754; Harrison's Principles of Internal Medicine 22E, p. 1937
This is a shared conversation. Sign in to Orris to start your own chat.