
IMG-20260706-WA0038(1).jpg
Diagnosis life cycle epidemiology pathophysiology differential diagnosis signs and symptoms treatment prevention conclusion
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Entamoeba histolytica" AND "liver abscess"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full, structured answer.
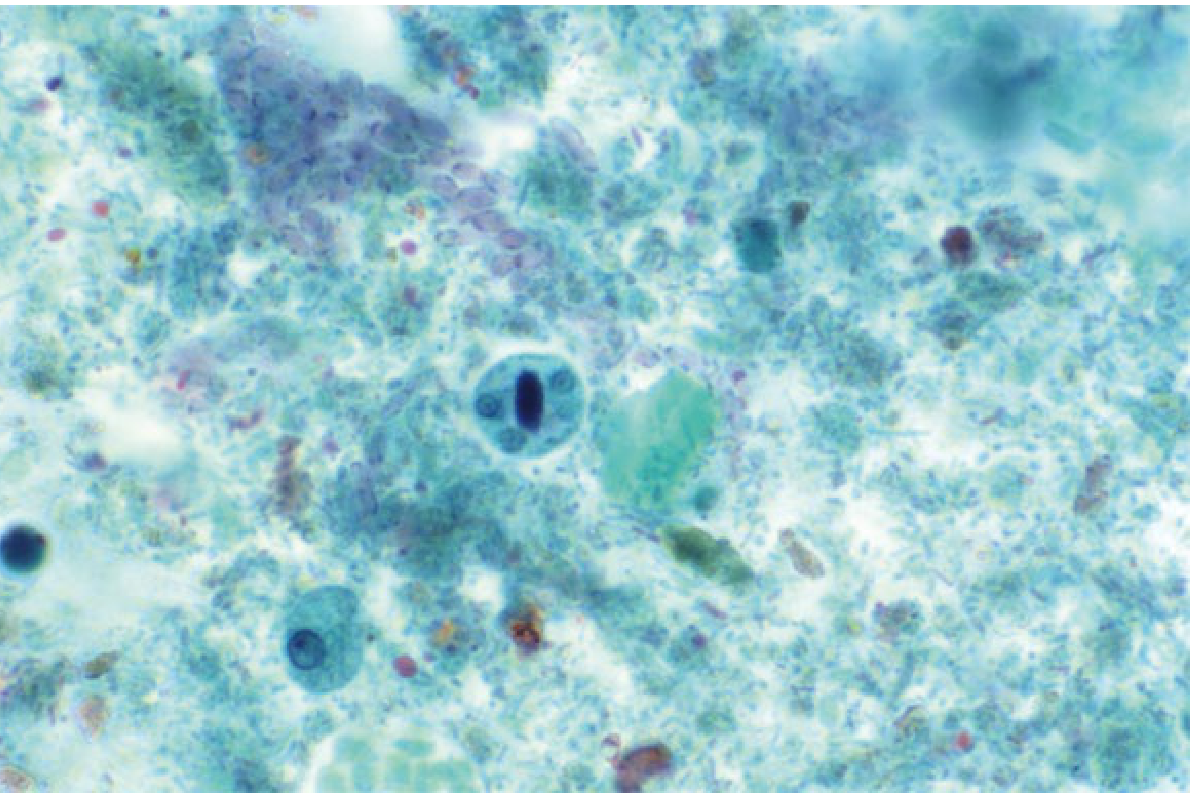
Case Study 2 - Diagnosis: Amoebic Liver Abscess (Hepatic Amoebiasis)
Causative agent: Entamoeba histolytica
The clues in the case are: Fijian soldier (endemic region traveler), fever unresponsive to antibiotics, multiple liver abscesses on CT, negative bacterial cultures, parasite detected by PCR of abscess material, clinical response to metronidazole + paromomycin, and negative post-treatment stool antigen/PCR confirming eradication.
1. Diagnosis
The definitive diagnosis is amoebic liver abscess (ALA), the most common extraintestinal manifestation of Entamoeba histolytica infection.
Diagnostic workup:
-
Imaging: Ultrasound or CT scan - shows single (80%) or multiple hypoechoic lesions, predominantly in the right lobe. In this case, CT confirmed multiple liver abscesses.
-
Serology: Indirect haemagglutination (IHA) and ELISA are highly sensitive (>90%) for extraintestinal amoebiasis. Serology is often negative in purely intestinal disease.
-
PCR of abscess material: As in this case, PCR is the most sensitive method when cultures are negative and serology inconclusive - it confirmed the diagnosis here.
-
Stool antigen detection: ELISA-based antigen kits are specific for E. histolytica (not the non-pathogenic E. dispar). Post-treatment stool antigen and PCR were negative, confirming eradication.
-
Aspiration: Yields the classic "anchovy sauce" (chocolate-brown, odourless) fluid - a mixture of necrotic liver and blood. Trophozoites are found in the abscess wall (not the pus) in only a minority of cases.
-
Blood cultures: Negative (as in this patient) - distinguishing ALA from pyogenic liver abscess.
-
Yamada's Textbook of Gastroenterology, 7th ed.
-
Bailey and Love's Short Practice of Surgery, 28th ed.
2. Life Cycle of Entamoeba histolytica
The life cycle consists of two stages:
- Cyst (infective stage): Quadrinucleate cysts are excreted in faeces and are stable in the environment - resistant to chlorine at normal water disinfection doses, but killed by heat (>55°C), drying, or freezing.
- Excystation: Ingested cysts pass through the stomach (resistant to gastric acid) and excyst in the small intestine, undergoing nuclear and cytoplasmic division to release 8 trophozoites.
- Trophozoite (tissue-invasive stage): The motile feeding form with a single nucleus and pseudopodia. Trophozoites colonize the large intestine, invade the submucosa to form flask-shaped ulcers, multiply by binary fission, and produce uninucleate cysts.
- Portal dissemination: Trophozoites enter the portal circulation, become trapped in interlobular veins of the liver, multiply in portal triads, and cause focal hepatocyte infarction and liquefactive necrosis via proteolytic enzymes - forming the abscess.
- Transmission: Only cysts (not trophozoites) transmit the disease. Trophozoites rapidly degenerate outside the body and are destroyed by gastric acid. Humans are the only reservoir.
- Yamada's Textbook of Gastroenterology, 7th ed., p. 3091
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 88
- Park's Textbook of Preventive and Social Medicine
3. Epidemiology
- Global burden: ~500 million people infected with Entamoeba spp. worldwide; ~40 million develop invasive colitis or extraintestinal abscesses; ~50,000 deaths annually. Among parasitic diseases, only cryptosporidiosis, malaria, and schistosomiasis cause comparable mortality.
- Geographic distribution: Most prevalent in Central and South America (especially Mexico), the Indian subcontinent, Indonesia, sub-Saharan and tropical Africa, and South East Asia. Prevalence of E. histolytica in stool samples in high-endemic zones averages ~10%; incidence of ALA can reach 21 per 100,000 population.
- High-risk groups in non-endemic countries: Travelers, immigrants, institutionalized individuals, and men who have sex with men (MSM).
- Sex difference: The prevalence of colonic disease is equal between sexes, but ALA and other extraintestinal disease is 3-10 times more common in men. This case (48-year-old male) fits this pattern exactly.
- Other risk factors for severe disease: Children (especially neonates), pregnant women, malignancy, malnutrition, corticosteroid therapy.
- Socioeconomic link: More closely tied to poor sanitation and low socioeconomic status than to climate. In areas with wet-dry seasons, transmission increases during rains due to cyst survival in water.
A 2025 systematic review and meta-analysis (PMID: 39979548) from India confirmed the epidemiological profile, risk factors, and clinical characteristics of ALA.
- Yamada's Textbook of Gastroenterology, 7th ed.
- Park's Textbook of Preventive and Social Medicine, p. 283-284
4. Pathophysiology
- Ingestion: Contaminated food/water introduces cysts via the faecal-oral route.
- Intestinal invasion: Trophozoites invade the colonic submucosa, producing flask-shaped ulcers (wide base, narrow neck) - predominantly in the caecum and ascending colon, then rectum and sigmoid. This stage may be asymptomatic in up to 90% of infected individuals.
- Portal entry: Trophozoites gain access to the mesenteric venules and are carried via the portal vein to the liver.
- Hepatic trapping: Trophozoites are filtered and trapped in the interlobular veins and multiply in portal triads.
- Liquefactive necrosis: Trophozoites produce proteolytic enzymes (cysteine proteases, amoebapores) causing focal infarction and coalescent liquefactive necrosis. The necrotic cavity fills with the characteristic anchovy-sauce fluid.
- Right lobe predominance (80%): Blood from the superior mesenteric vein flows more directly into the larger right lobe via the portal vein, explaining this anatomical predilection. Left lobe involvement accounts for ~10%; multiple abscesses (as in this case) are the remainder.
- Chest complications: Abscesses high on the diaphragmatic surface of the right lobe can cause reactive pleural effusion, basal pneumonitis, and even transdiaphragmatic rupture into the pleural space - explaining this patient's dyspnoea and pulmonary infiltrates on initial presentation.
- Secondary infection: Sterile unless secondarily infected (which causes the pus to become malodorous).
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 88
5. Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Pyogenic liver abscess | Positive bacterial blood/pus cultures, often Gram-negative rods (Klebsiella, E. coli), older patients, biliary/GI source, septate lesions |
| Hydatid cyst (Echinococcus) | Cystic lesion with daughter cysts on imaging, serology positive, eosinophilia, history of sheep/dog contact |
| Hepatocellular carcinoma | AFP elevated, cirrhotic background, solid mass with arterial enhancement on CT |
| Pyogenic pneumonia / lung abscess | Productive purulent cough, sputum cultures positive, no liver lesion |
| Typhoid fever | Rose spots, positive blood/bone marrow culture for Salmonella typhi, splenomegaly, relative bradycardia |
| Visceral leishmaniasis | Massive splenomegaly, pancytopenia, positive rK39 antigen, bone marrow aspirate |
| Hepatic tuberculosis | Calcified granulomas, positive Mantoux/IGRA, chronic course, constitutional symptoms |
In this case, negative bacterial cultures of both blood and abscess, combined with positive PCR for the parasite, excluded pyogenic abscess and confirmed amoebic aetiology.
6. Signs and Symptoms
Typical patient: Young adult male with insidious onset progressing over days to weeks.
Systemic symptoms:
- Fever (often swinging, as in this patient - 39.5°C)
- Night sweats and rigors
- Anorexia, malaise, weight loss
Localizing symptoms:
- Right upper quadrant / right hypochondrial pain (progresses to right shoulder tip pain - diaphragmatic irritation)
- Non-productive cough and dyspnoea (from diaphragmatic elevation/reactive effusion)
- Hiccoughs (diaphragmatic involvement)
Signs on examination:
- Toxic, ill-appearing, anaemic patient
- Tender hepatomegaly (most consistent finding)
- Tender and bulging intercostal spaces with overlying skin oedema
- Upper abdominal rigidity
- Pleural effusion and basal pneumonitis (late)
- Occasionally jaundice or ascites
Complications:
- Rupture into pleural cavity (empyema), peritoneal cavity (peritonitis), or pericardial cavity (tamponade - most feared)
- Secondary infection of the abscess
- Amoeboma (chronic granuloma in large bowel from incomplete treatment)
Laboratory findings:
-
Leukocytosis with neutrophilia (as in this patient: 25,000/mm³, 84%)
-
Elevated ESR and CRP
-
Mildly elevated liver enzymes (ALP most consistently raised)
-
Anaemia in chronic cases
-
Bailey and Love's Short Practice of Surgery, 28th ed.
7. Treatment
Medical (first-line)
- Metronidazole 400-800 mg three times daily for 5-10 days (or tinidazole as an alternative) - this is the tissue amoebicide that kills trophozoites.
- Followed by a luminal amoebicide to eradicate residual cysts in the gut: Paromomycin (500 mg three times daily for 7 days) or diloxanide furoate (500 mg three times daily for 10 days). This step prevents relapse and ongoing transmission.
- In this case: metronidazole + paromomycin - the textbook regimen. Ceftriaxone was added initially for presumed secondary bacterial infection and was discontinued once cultures were negative.
Drainage indications
- Large abscesses (>5 cm): percutaneous needle aspiration or pigtail catheter drainage combined with drug treatment.
- Drainage is recommended when: the abscess is large and at high risk of rupture; there is inadequate response to medical therapy within 72 hours; left lobe abscess (risk of pericardial rupture); suspected secondary infection.
- In this patient, a drain was placed and removed on day 21 as the discharge transitioned from purulent to serosanguinous.
Surgical treatment
Reserved for complications:
-
Rupture into pleural, peritoneal, or pericardial cavity
-
Acute toxic megacolon (intestinal amoebiasis)
-
Severe haemorrhage
-
Bailey and Love's Short Practice of Surgery, 28th ed.
-
Maingot's Abdominal Operations
8. Prevention
Primary Prevention
- Sanitation: Safe disposal of human excreta; hand washing after defecation and before eating. This is the single most effective measure.
- Water supply: Protection from faecal contamination. Note - chlorine at normal doses does NOT kill amoebic cysts. Sand filtration and boiling are more effective. Iodine-based purification tablets (used in military settings) are also effective.
- Food hygiene: Thorough washing of raw vegetables with detergent in running water; alternatively, soaking in 5-10% acetic acid or full-strength vinegar removes cysts. Uncooked vegetables from fields irrigated with sewage water are a major risk. Food handlers should be screened, treated, and educated.
- Vector control: Control of flies, cockroaches, and rodents that mechanically transmit cysts.
- Health education: Long-term community education on personal hygiene.
- Military-specific: Soldiers deployed to endemic regions should receive pre-deployment health briefings, use water purification beyond chlorination alone, and practice strict food/hand hygiene.
Secondary Prevention
-
Early diagnosis of symptomatic and carrier individuals.
-
Treatment of asymptomatic carriers (luminal agents like paromomycin) to interrupt transmission.
-
Periodic screening of food handlers in endemic areas.
-
Contact tracing within households (amoebiasis is frequently a household infection - when one member is infected, others may also be affected).
-
Park's Textbook of Preventive and Social Medicine, p. 284
9. Conclusion
This case of a 48-year-old Fijian soldier illustrates several teaching points about amoebic liver abscess:
- Delayed diagnosis is common because initial presentation with fever, dyspnoea, and interstitial infiltrates mimics community-acquired pneumonia. ALA should be considered in any patient from or traveling to an endemic region who does not respond to standard antibiotics for CAP.
- PCR of abscess material is the key diagnostic tool when cultures are negative - it was diagnostic in this case.
- Medical therapy is highly effective: metronidazole as the tissue agent followed by paromomycin as the luminal agent is the standard regimen. This patient was successfully treated without surgery.
- Drainage is needed for large/complex abscesses - this patient required percutaneous drainage with drain removal on day 21.
- Post-treatment negative stool antigen and PCR confirmed microbiological cure.
- Prevention in military/travel settings hinges on water boiling/filtration (not chlorination alone), food hygiene, and sanitation - all critical for deployed personnel in endemic zones.
Sources: Bailey and Love's Short Practice of Surgery, 28th ed. | Yamada's Textbook of Gastroenterology, 7th ed. | Park's Textbook of Preventive and Social Medicine | Maingot's Abdominal Operations | Ghalib et al. 2025, Int Microbiol [PMID: 39979548]
This is a shared conversation. Sign in to Orris to start your own chat.