Cushing syndrome and
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"Cushing syndrome" clinical features signs symptoms
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content and two excellent illustrations. Here is a full, well-organized answer.
Cushing Syndrome - Signs & Symptoms
Cushing syndrome results from chronic excess glucocorticoids, either from endogenous overproduction or exogenous steroid use. All the clinical features flow directly from the known actions of excess cortisol (and, in some causes, excess adrenal androgens).
Classic Body Habitus
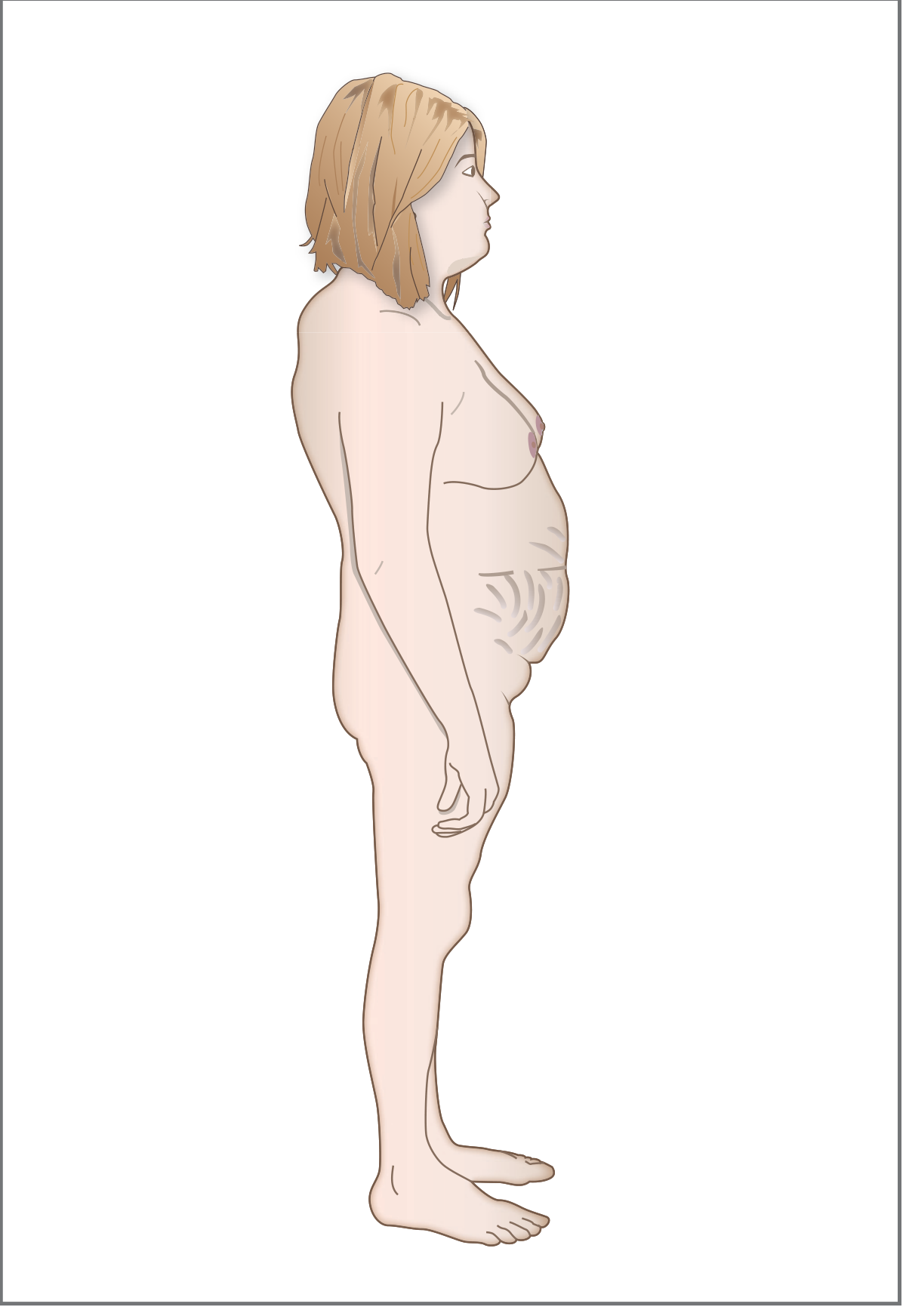
Illustration from Costanzo Physiology 7e showing the characteristic body shape.
- Central obesity - fat accumulates on the face, neck, trunk, and abdomen, while the limbs remain thin (due to increased lipolysis peripherally + muscle wasting)
- Moon face - round, wide, plethoric face with fat deposition
- Buffalo hump - fat pad deposited over the upper back/posterior neck
- Supraclavicular fat pads
- Thin extremities with proximal muscle weakness and wasting
Skin Changes (prominent and diagnostically useful)
These are described in detail by Andrews' Diseases of the Skin:
| Feature | Mechanism |
|---|---|
| Purplish/violaceous striae (abdomen, buttocks, thighs, breasts, upper arms) | Loss of connective tissue from excess cortisol |
| Thin, fragile skin ("cigarette paper" wrinkling) | Protein catabolism, reduced collagen |
| Easy bruising / ecchymoses | Skin and capillary fragility |
| Liddle sign - skin tears off with adhesive tape removal | Extreme skin fragility |
| Hypertrichosis / facial lanugo hair (especially in women) | Excess adrenal androgens |
| Acne | Androgen excess |
| Facial plethora (cheeks, anterior neck, chest V) | Increased RBC mass + skin thinning |
| Poor wound healing | Impaired immune/fibroblast function |
| Scalp hair thinning (women) | Androgen effects |
| Opportunistic fungal infections (dermatophyte, Pityrosporum) | Immunosuppression |
| Occasionally: livedo reticularis, purpura, brownish pigmentation | Variable |
Women are affected 4 times more frequently than men in non-iatrogenic cases. Peak onset is in the 20s and 30s.
Metabolic & Systemic Features
- Hypertension - cortisol has weak mineralocorticoid activity AND upregulates vascular alpha-1 adrenergic receptors, increasing responsiveness to catecholamines
- Hyperglycemia / diabetes mellitus - cortisol promotes gluconeogenesis and insulin resistance; ~20% of patients develop frank DM
- Hypokalemia - more pronounced in ectopic ACTH syndrome (where ACTH levels are very high)
- Hyperlipidemia - central fat redistribution
- Increased susceptibility to infections - immunosuppression
Musculoskeletal
- Proximal myopathy - weakness of hip and shoulder girdle muscles (difficulty rising from a chair, climbing stairs)
- Osteoporosis with back pain, vertebral compression fractures
- Kyphosis of the dorsal spine (which can accentuate the buffalo hump)
- Generalized arteriosclerosis with progressive prostration and limb/abdominal pains
Reproductive / Endocrine
- Menstrual irregularities and amenorrhea in women (from androgen excess and HPA dysregulation)
- Virilization in women - due to excess adrenal androgens
- Loss of libido in both sexes
- Hypogonadism
Neuropsychiatric
- Depression, anxiety, emotional lability
- Cognitive impairment
- Sleep disturbance (loss of normal cortisol circadian rhythm)
Causes at a Glance
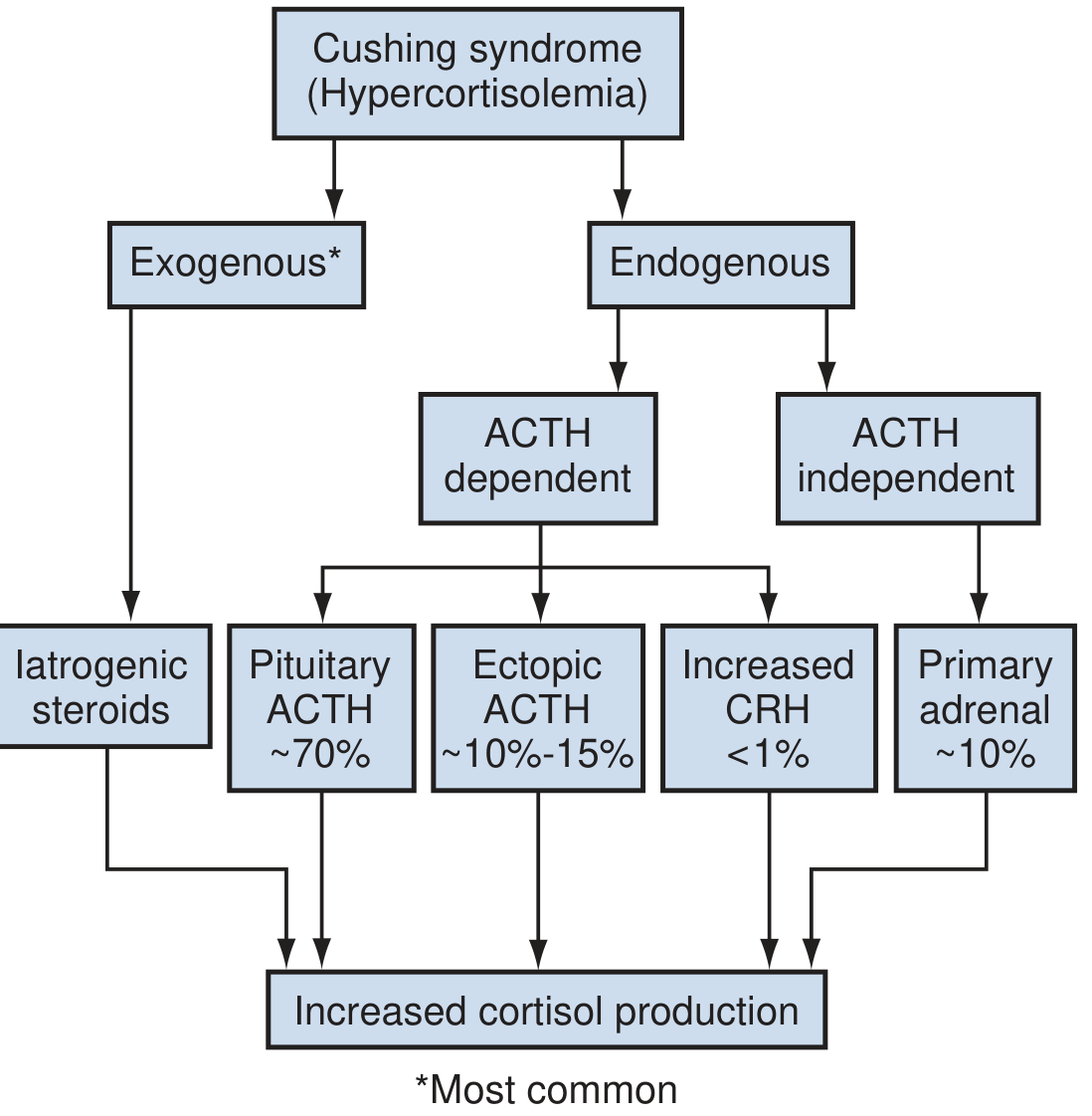
- Exogenous (iatrogenic) steroids - most common overall
- Cushing disease (pituitary ACTH-secreting adenoma) - ~70% of endogenous cases
- Ectopic ACTH (usually malignant tumors, e.g. small cell lung) - ~10-15%
- Primary adrenal (adenoma, carcinoma, PPNAD) - ~10%
- Pseudo-Cushing syndrome - mimicked by alcohol abuse
Note: Cushing disease specifically refers to the pituitary-driven subtype; Cushing syndrome is the broader term for all causes of hypercortisolism.
Quick Diagnostic Clue
The overnight 1 mg dexamethasone suppression test is a rapid screen: cortisol below 50 nmol/L at 8 AM essentially rules out Cushing syndrome (except the iatrogenic form, where cortisol is already low due to adrenocortical suppression).
Sources: Andrews' Diseases of the Skin (9780323547536); Costanzo Physiology 7e (9780323793339); Campbell-Walsh-Wein Urology (9780323546423)
This is a shared conversation. Sign in to Orris to start your own chat.