Cement in eye . What's its management
Reading File
Finding Sources
Finding Sources
Searching PubMed
cement lime alkali ocular chemical injury management
Reading File
Finding Sources
Searching PubMed
"ocular chemical burn" AND treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed. Here is a complete, structured answer.
Cement in the Eye - Management
Cement contains calcium hydroxide (Ca(OH)₂) - a strong alkali (pH ~12-13). This makes it one of the most dangerous ocular chemical injuries. Alkali penetrates more deeply than acids via liquefactive necrosis, causing ongoing damage long after initial contact.
STEP 1 - Immediate Irrigation (Emergency - Do This First)
This is the single most important intervention. The speed and efficacy of irrigation is the most important prognostic factor.
- Start immediately - do not delay for any assessment
- In pre-hospital setting: tap water is ideal - have the patient submerge the eye in running tap water and continuously open/close the eyelid. Turn the head so the affected eye is lower to avoid contaminating the unaffected eye
- In hospital/ED: use sterile normal saline, lactated Ringer's, or balanced salt solution (BSS) - preferred over tap water due to hypotonicity concerns
- Instill topical anaesthetic (e.g. proparacaine) before/during irrigation - dramatically improves compliance and cooperation
- A lid speculum may be helpful to keep the eye open
- Irrigate at least 2 litres over the first 30 minutes continuously
- A Morgan lens can be used; if used, replace between each litre to avoid trapping chemical
Critical additional step: Double-evert the upper eyelid and sweep the fornices with a moist cotton bud to remove any retained cement particles. Cement is particulate and fragments lodge in the fornices, continuing to leach alkali long after irrigation.
-
After 2 L, check conjunctival pH with litmus paper
-
Continue irrigating until pH reaches 7.0-7.4 (neutral)
-
Recheck pH every 15-30 minutes; normalization typically takes 30-60 minutes
-
Debride any necrotic corneal epithelium at the slit lamp to remove residual chemical
-
Harriet Lane Handbook, p. 74; Kanski's Clinical Ophthalmology 10th ed., p. 945; Rosen's Emergency Medicine
STEP 2 - Assessment
| Assessment | Method |
|---|---|
| Visual acuity | Test and trend from outset |
| Conjunctival pH | Litmus paper - before and after irrigation |
| Slit-lamp exam | Corneal clarity, fluorescein staining, limbal ischaemia |
| IOP | Check intraocular pressure |
| Fundus | If penetrating injury suspected |
STEP 3 - Grading (Roper-Hall Classification)
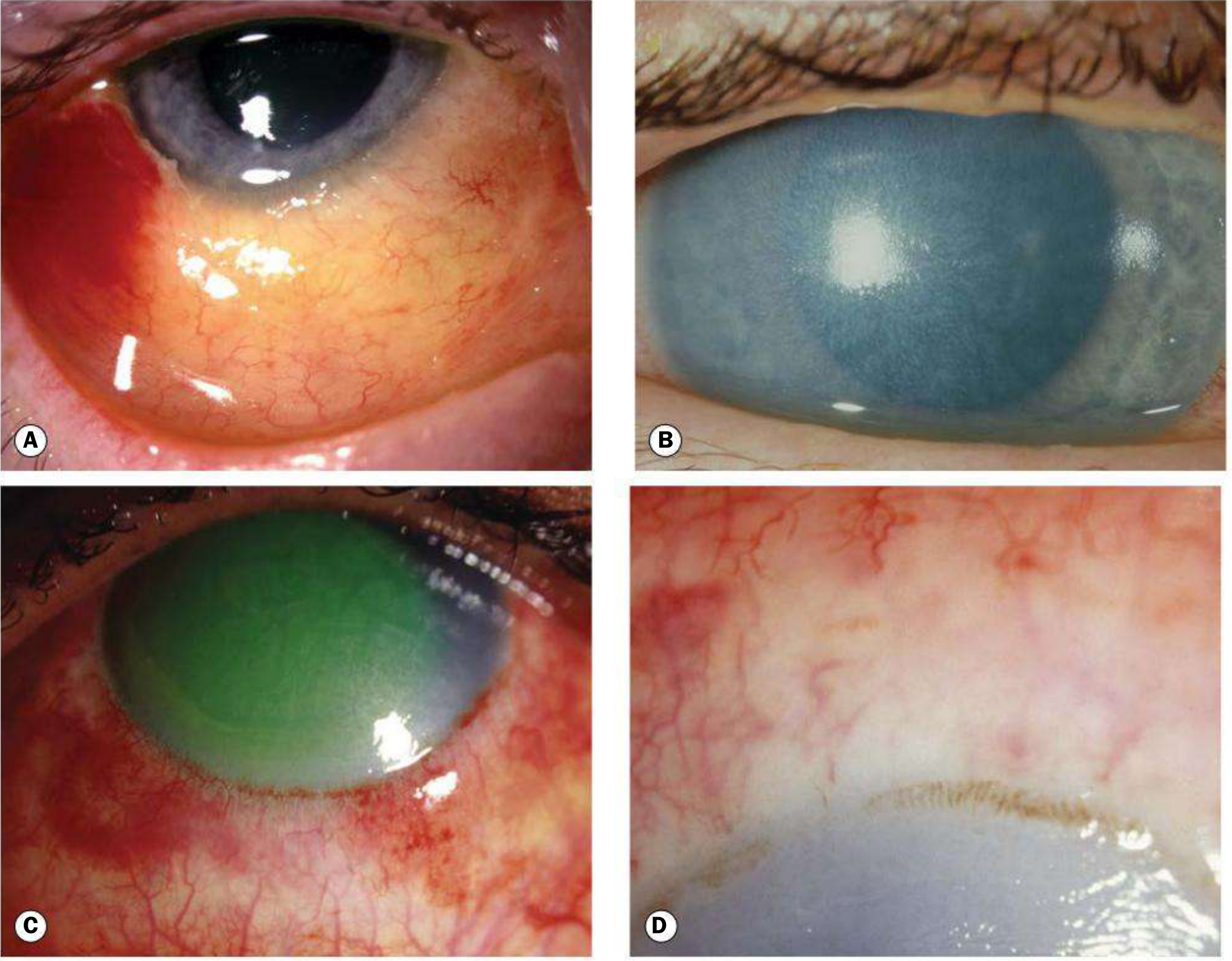
| Grade | Cornea | Limbal Ischaemia | Prognosis |
|---|---|---|---|
| 1 | Clear (epithelial damage only) | None | Excellent |
| 2 | Hazy, iris detail visible | <1/3 | Good |
| 3 | Haze obscures iris detail | 1/3 to 1/2 | Guarded |
| 4 | Opaque | >1/2 | Poor |
The Dua classification (6 grades based on clock hours of limbal involvement + % conjunctival involvement) provides better prognostic discrimination, especially for severe cases.
- Kanski's Clinical Ophthalmology 10th ed., p. 945
STEP 4 - Medical Treatment
Mild injuries (Grade 1-2)
- Topical antibiotic ointment for ~1 week (e.g. chloramphenicol 4x daily)
- Topical steroids + cycloplegics if necessary
Moderate-severe injuries (Grade 3-4) - use preservative-free drops
All the below aim to reduce inflammation, promote re-epithelialisation, and prevent corneal ulceration:
| Drug | Rationale | Regimen |
|---|---|---|
| Topical corticosteroids | Reduce inflammation and neutrophil infiltration; treat anterior uveitis | 4-8x daily initially; taper off at 7-10 days (risk of sterile corneal ulceration) |
| Cycloplegics (e.g. atropine 1%) | Pain relief, prevent posterior synechiae | Twice daily |
| Topical antibiotics (e.g. chloramphenicol) | Prophylaxis against infection | 4x daily |
| Sodium ascorbate 10% topical + oral Vitamin C 1-2 g QID | Promotes mature collagen synthesis by corneal fibroblasts | Every 2 hours topically |
| Sodium citrate 10% topical (Grade 3-4) | Potent neutrophil inhibitor; inhibits collagenase; targets the "second wave" of phagocytes ~7 days post-injury | Every 2 hours for ~10 days; also oral (2 g QID) |
| Tetracyclines / doxycycline | Collagenase inhibitor; reduce corneal melting | Topical ointment 4x/day + oral doxycycline 100 mg BD |
| Acetylcysteine 10% | Alternative anticollagenase | 6x daily topically |
| IOP management (oral acetazolamide if raised) | Raised IOP is common in severe burns | Avoid topical drops to reduce ocular surface burden |
- Prevent symblepharon formation by daily lysis of developing adhesions with a sterile glass rod or damp cotton bud
- Kanski's Clinical Ophthalmology 10th ed., p. 945
STEP 5 - Referral and Admission
- Urgent ophthalmology referral for: significant vision loss, uncontrolled pain, persistent pH abnormality, significant mucosal injury, or Grade 3-4 injuries
- Hospital admission is usually required for Grade 3-4 injuries to ensure adequate drop instillation in the early stages
- Consider dermatology opinion if periocular skin is involved
- Harriet Lane Handbook, p. 74
Key Points to Remember
- Cement = alkali = deeper and more dangerous than acid burns (liquefactive necrosis vs. coagulative)
- Particulate matter (cement fragments) must be physically removed from the fornices - irrigation alone is insufficient
- Steroids must be tapered by day 7-10 to avoid sterile corneal ulceration
- Early ophthalmology involvement is essential for all but the most trivial exposures
This is a shared conversation. Sign in to Orris to start your own chat.