Opportunistic infections in transplant patients full details for md exams 10 marks answer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"opportunistic infections" AND "solid organ transplant"
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Excellent - I now have comprehensive, detailed content from multiple authoritative sources. Let me compile the complete MD exam answer.
Opportunistic Infections in Transplant Patients
Introduction
Transplant recipients are a unique immunocompromised population in whom the intentional suppression of immunity to prevent allograft rejection creates a sustained vulnerability to a wide spectrum of infections. These range from common bacteria to rare opportunistic pathogens that would not cause disease in immunocompetent hosts. The pattern, timing, and severity of infections are directly related to the net state of immunosuppression.
The "net state of immunosuppression" is determined by:
- Type and dose of immunosuppressive drugs (induction agents vs. maintenance)
- Prior and current exposure to immunosuppressive therapy
- Underlying disease (diabetes, chronic renal failure)
- Pre-existing infections (CMV, EBV, HBV)
- Mucosal barrier integrity
- Neutropenia
- Anatomical disruption from surgery
Temporal Classification (Timeline of Infections)
The most important framework for understanding opportunistic infections in transplant patients is the time-based model introduced by Fishman (N Engl J Med 2007). Infections follow a predictable temporal pattern that guides both prophylaxis and differential diagnosis.
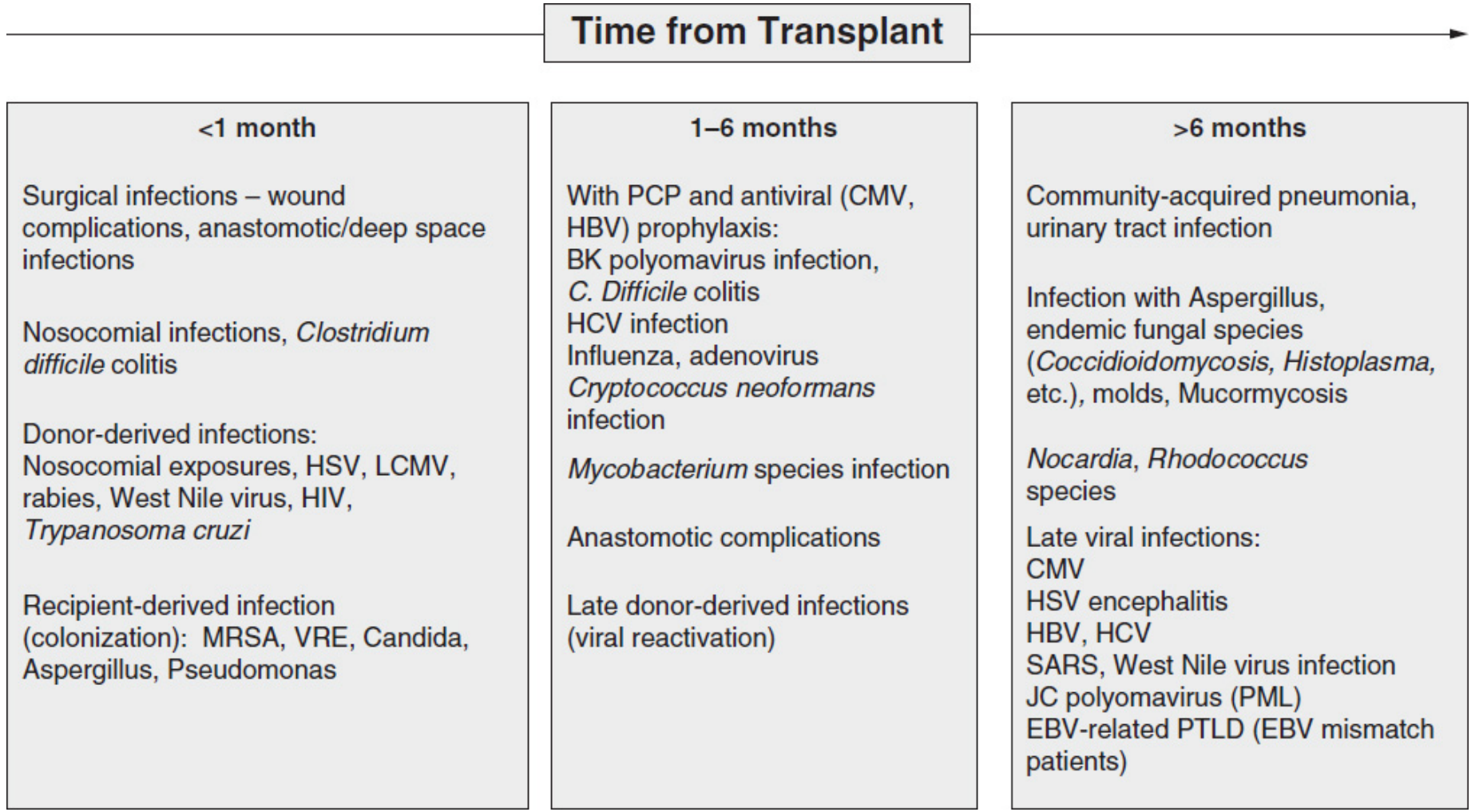
Period 1: First Month Post-Transplant (<1 month)
Infections in this period are primarily nosocomial and surgical in origin. True classic opportunistic infections are uncommon unless the patient was immunocompromised before transplant.
Organisms:
- Bacteria: MRSA, VRE, gram-negative bacilli (E. coli, Pseudomonas, Klebsiella), CRE, extended-spectrum beta-lactamase (ESBL) producers
- Candida species (wound, catheter, urinary sites)
- Herpes simplex virus (HSV) - most common viral infection in this period
- Donor-derived unexpected infections: HIV, West Nile virus, rabies, LCMV, Trypanosoma cruzi
Sites: Surgical wounds, urinary catheters, vascular catheters, anastomotic sites, respiratory tract (ventilator-associated pneumonia)
Key point: Development of classic opportunistic infections (PCP, CMV disease) in this early period should raise suspicion of donor-transmitted infection or pre-existing immunodeficiency.
Period 2: Months 1-6 Post-Transplant (Classic Opportunistic Period)
This is the period of maximum immunosuppression and is characterized by the classic opportunistic infections. Without prophylaxis, this period is dominated by:
Viral:
- CMV (most important) - primary or reactivation
- EBV - risk of PTLD
- BK polyomavirus (renal allograft loss)
- Adenovirus
- RSV and other community respiratory viruses
- HBV, HCV (reactivation or new infection)
Fungal:
- Pneumocystis jirovecii (PCP/PJP) - if not on TMP-SMX prophylaxis
- Aspergillus spp. and other molds
- Cryptococcus neoformans
- Candida spp.
Bacterial:
- Listeria monocytogenes
- Nocardia spp.
- Mycobacterium tuberculosis (reactivation)
Parasitic:
- Toxoplasma gondii (esp. heart transplant, donor+/recipient-)
- Strongyloides stercoralis (hyperinfection syndrome)
- Trypanosoma cruzi, Leishmania spp. (reactivation in endemic regions)
Reactivation of endemic mycoses: Histoplasma capsulatum, Coccidioides spp., Blastomyces, Paracoccidioides
Period 3: After 6 Months
Risk is determined by the balance of graft function and immunosuppression intensity. Three subgroups exist:
| Group | Population | Infection Risk |
|---|---|---|
| Group 1 (~70-80%) | Good graft function, low-dose maintenance | Community-acquired infections (pneumococcus, influenza); opportunistic infections unusual |
| Group 2 (~10%) | Chronic viral infections (CMV, EBV, BK, HBV/HCV) | Risk of PTLD, BK nephropathy, progressive liver disease |
| Group 3 (~10%) | Repeated rejection episodes, heavy immunosuppression | High risk: PCP, Cryptococcus, Nocardia, Listeria, endemic mycoses, CMV, HSV encephalitis, JC virus (PML) |
Key Opportunistic Pathogens - In Detail
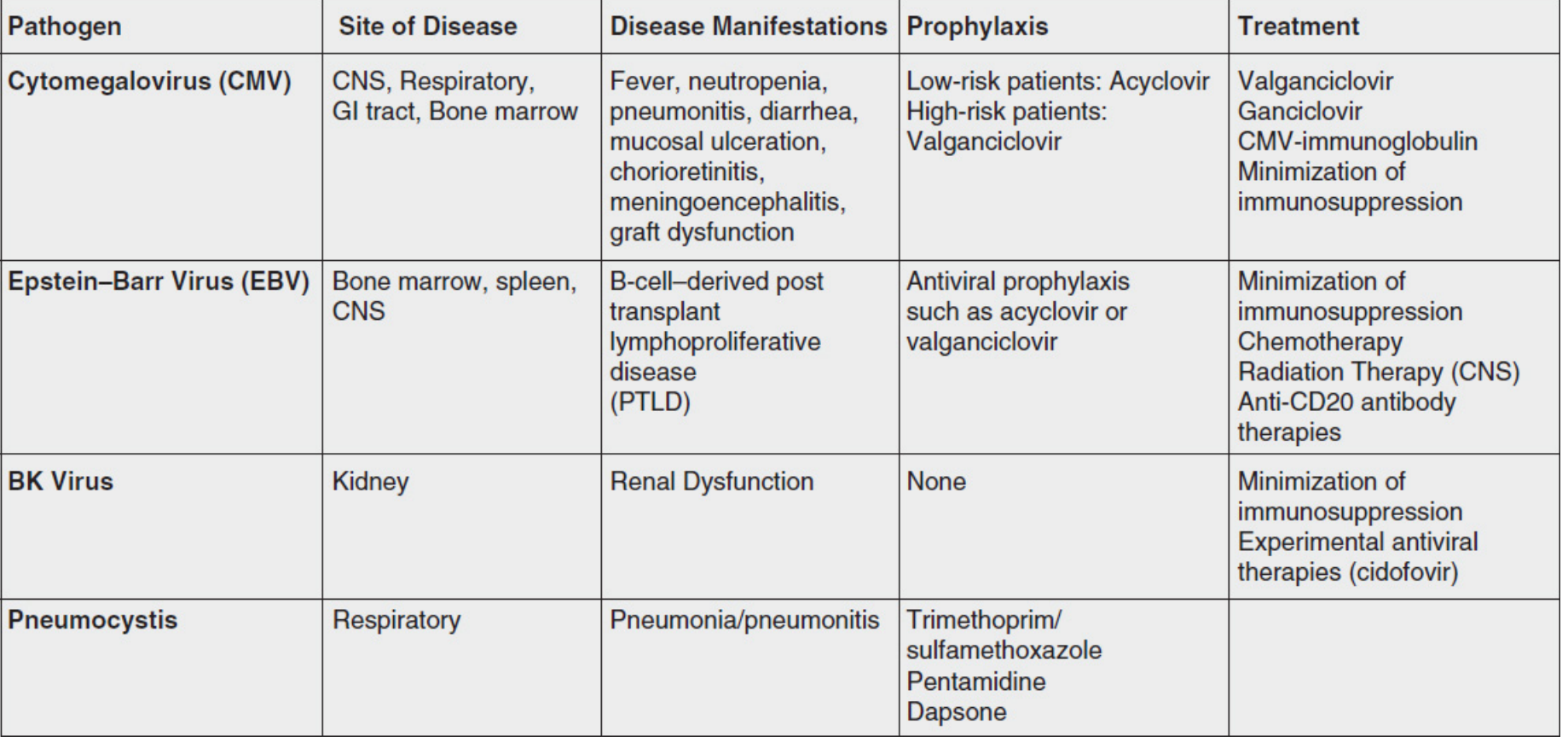
1. Cytomegalovirus (CMV)
The most important opportunistic infection in solid organ transplant recipients.
- Sites: CNS, respiratory tract, GI tract, bone marrow, retina
- Manifestations: CMV syndrome (fever, malaise, neutropenia, thrombocytopenia) OR tissue-invasive disease (CMV pneumonitis, CMV colitis/enteritis, CMV retinitis, CMV hepatitis, meningoencephalitis, graft dysfunction)
- Risk stratification:
- Highest risk: Donor seropositive (D+) / Recipient seronegative (R-) - primary infection
- Intermediate: D+/R+ or D-/R+ - reactivation or superinfection
- Lowest: D-/R-
- Indirect effects: CMV infection itself enhances immunosuppression, increasing risk of bacterial and fungal superinfections; associated with accelerated graft rejection
- Diagnosis: Quantitative PCR for CMV DNA in blood (viral load); pp65 antigenemia assay; tissue biopsy showing CMV inclusion bodies ("owl's eye" intranuclear inclusions)
- Prophylaxis:
- Low-risk: Acyclovir
- High-risk (D+/R-): Valganciclovir orally (drug of choice) for 3-6 months post-transplant
- Treatment: IV Ganciclovir or oral Valganciclovir (first line); Foscarnet (second line, nephrotoxic); Cidofovir (nephrotoxic, reserve); CMV immunoglobulin as adjunct; reduce immunosuppression
2. Pneumocystis jirovecii Pneumonia (PJP/PCP)
- Previously called PCP (Pneumocystis carinii pneumonia); causative organism reclassified as P. jirovecii in humans
- Manifestations: Subacute progressive dyspnea, non-productive cough, fever; bilateral interstitial infiltrates on CXR; "ground-glass" opacification on HRCT
- Diagnosis: Bronchoalveolar lavage (BAL) with Gomori methenamine silver (GMS) stain or DIF; serum beta-D-glucan elevated; PCR on BAL
- Prophylaxis (standard of care):
- First line: TMP-SMX (single or double strength) daily or 3x/week for 6-12 months post-transplant; restart after any pulse of corticosteroids or antilymphocyte therapy
- Alternatives (sulfa allergy): Dapsone (check G6PD first), Atovaquone, Aerosolized pentamidine
- TMP-SMX also covers: Toxoplasma, Listeria monocytogenes, Nocardia, and reduces UTI risk in renal transplant
- Treatment: High-dose TMP-SMX IV (drug of choice); adjunctive corticosteroids if PaO2 <70 mmHg; Pentamidine for TMP-SMX intolerance
3. Epstein-Barr Virus (EBV) and PTLD
- Post-Transplant Lymphoproliferative Disorder (PTLD) is the most important complication
- Driven by EBV-driven uncontrolled B-cell proliferation in the absence of T-cell surveillance
- Risk: Highest in EBV-seronegative recipients receiving organs from EBV-seropositive donors (mismatch); pediatric recipients at highest risk
- Spectrum: Ranges from infectious mononucleosis-like illness to polymorphic PTLD to monomorphic B-cell lymphoma (most common) or T-cell lymphoma
- Sites: Bone marrow, spleen, CNS, allograft itself
- Diagnosis: EBV viral load monitoring by PCR; tissue biopsy with immunohistochemistry (CD20+ B cells)
- Treatment:
- First step: Reduction of immunosuppression (often leads to regression in early lesions)
- Rituximab (anti-CD20 monoclonal antibody) for CD20+ PTLD
- Chemotherapy (CHOP-like regimens) for aggressive/monomorphic PTLD
- CNS radiation therapy for CNS involvement
- Prophylaxis: Acyclovir or valganciclovir can reduce EBV replication
4. BK Polyomavirus (BKPyV)
- Unique to kidney transplant recipients (causes BK virus-associated nephropathy, BKVAN)
- Ubiquitous latent virus in the urinary tract; reactivates under immunosuppression
- Manifestations: Asymptomatic viruria → viremia → BKVAN → graft loss (in up to 5% of infected patients); less commonly hemorrhagic cystitis
- Diagnosis: Urine cytology (decoy cells - large cells with intranuclear inclusions); urine and plasma quantitative PCR; renal biopsy (intranuclear inclusions in tubular cells, interstitial nephritis)
- Screening: Regular plasma PCR monitoring post-transplant (monthly for first 6-12 months)
- Treatment: No proven antiviral; reduction of immunosuppression is cornerstone
- Experimental: Cidofovir (nephrotoxic), Leflunomide (has antiviral activity via metabolite A77 1726), fluoroquinolones (reduce viral load in urine)
- No established prophylaxis
5. Fungal Infections
Invasive Candidiasis:
- Most common in first month post-transplant
- Primarily C. albicans; increasingly non-albicans species (C. glabrata, C. krusei - fluconazole resistant)
- Prophylaxis: Fluconazole or Nystatin swish-and-swallow (especially liver, pancreas-kidney recipients)
- Treatment: Fluconazole (for susceptible strains); Echinocandins (anidulafungin, caspofungin, micafungin) for resistant strains; Amphotericin B for severe/resistant cases
Invasive Aspergillosis:
- Primarily Aspergillus fumigatus; most common in lung transplant recipients
- Risk: Neutropenia, corticosteroid pulses, CMV infection, environmental exposure, single-lung transplant
- Manifestations: Pulmonary nodules with halo sign on CT, cavitation; angioinvasion with vascular thrombosis
- Prophylaxis: Voriconazole or inhaled Amphotericin B in high-risk recipients (lung transplant)
- Treatment: Voriconazole (first line); Isavuconazole; Liposomal Amphotericin B; Echinocandins (for voriconazole-refractory)
Cryptococcosis:
- Cryptococcus neoformans - typically 1-6 months post-transplant; can be late
- Manifestations: Subacute meningitis, meningoencephalitis, pulmonary disease, skin lesions (umbilicated papules); cryptococcemia
- Diagnosis: India ink stain, cryptococcal antigen (CrAg) in serum/CSF, fungal culture
- Treatment: Induction - Liposomal Amphotericin B + Flucytosine (2 weeks); Consolidation - Fluconazole; reduce immunosuppression; monitor ICP (serial LPs)
Endemic Mycoses (geographically restricted):
- Histoplasma capsulatum (Mississippi/Ohio River Valley), Coccidioides immitis (Southwestern USA/Latin America), Blastomyces, Paracoccidioides
- Can be primary or reactivation of latent disease
- Screen recipients from endemic areas; fluconazole prophylaxis for high-risk patients
- Treatment: Itraconazole (mild-moderate); Liposomal Amphotericin B (severe/disseminated)
Pneumocystis (see above)
6. Bacterial Opportunistic Infections
Listeria monocytogenes:
- Gram-positive rod; foodborne transmission
- Manifestations: Bacteremia, meningitis (CNS), febrile gastroenteritis
- Treatment: High-dose Ampicillin (± Gentamicin); TMP-SMX prophylaxis prevents this infection
Nocardia spp.:
- Aerobic gram-positive filamentous bacterium, weakly acid-fast
- Manifestations: Pulmonary nocardiosis (nodules, cavities, consolidation); cutaneous/subcutaneous disease; CNS nocardiosis (brain abscess)
- Treatment: TMP-SMX (high dose); Imipenem + Amikacin for severe/disseminated; duration 6-12 months
- TMP-SMX prophylaxis prevents Nocardia infection
Mycobacterium tuberculosis:
- Reactivation of latent TB most common (1-6 months post-transplant, but can be any time)
- Risk 20-74x higher than general population
- Manifestations: Often extrapulmonary and disseminated (lymphadenopathy, hepatic, CNS, bone marrow)
- Screening: Pre-transplant TST (tuberculin skin test) or IGRA; chest X-ray
- Prophylaxis: Isoniazid (INH) 9 months for LTBI (latent TB infection) pre- or post-transplant
- Treatment: Standard 4-drug RHEZ (Rifampicin, INH, Ethambutol, Pyrazinamide) - drug interactions with calcineurin inhibitors (rifampicin is a potent CYP3A4 inducer, drastically reduces tacrolimus/cyclosporine levels)
7. Toxoplasma gondii
- Most common and severe in cardiac transplant (risk: D+/R-)
- Encephalitis is the most common manifestation; myocarditis, disseminated disease
- TMP-SMX prophylaxis prevents Toxoplasma infection
- Treatment: Pyrimethamine + Sulfadiazine + Folinic acid; TMP-SMX as alternative
8. Strongyloides stercoralis (Hyperinfection Syndrome)
- Life-threatening in immunosuppressed hosts due to hyperinfection/dissemination
- Larvae penetrate gut wall, carry enteric bacteria, causing gram-negative bacteremia/meningitis
- Screen pre-transplant in patients from endemic areas (serology)
- Treatment/Prevention: Ivermectin
Organ-Specific Infection Risks
| Organ Transplant | Specific Infection Risk |
|---|---|
| Kidney | UTIs, BK virus nephropathy, CMV |
| Liver | Biliary/GI anastomotic bacterial/fungal infections, HBV/HCV recurrence |
| Heart | Toxoplasma (D+/R-), Aspergillus, CMV myocarditis |
| Lung | Aspergillus (anastomotic), PCP, CMV pneumonitis, bacterial pneumonia |
| Small bowel | Norovirus, viral gastroenteritis, Candida |
| Kidney-Pancreas | High Candida risk, CMV |
Standard Prophylaxis Protocols
| Target Pathogen | First-Line Prophylaxis | Alternative | Duration |
|---|---|---|---|
| Pneumocystis | TMP-SMX (SS or DS daily) | Dapsone, Atovaquone, Aerosolized pentamidine | 6-12 months (lifelong for lung Tx) |
| CMV (high risk D+/R-) | Valganciclovir | IV Ganciclovir | 3-6 months |
| CMV (low risk) | Acyclovir | Valacyclovir | 3-6 months |
| Candida | Fluconazole or Nystatin S&S | - | 1-3 months |
| HSV/VZV | Acyclovir/Valacyclovir | - | 3-6 months |
| TB (LTBI) | Isoniazid 9 months | - | Pre or post-transplant |
| Toxoplasma | TMP-SMX (covered by PCP prophylaxis) | Pyrimethamine | Per PCP duration |
Diagnostic Approach
When evaluating a transplant recipient with suspected infection:
- Time post-transplant - determines differential (the timeline above)
- Net state of immunosuppression - induction agents? recent rejection treatment?
- Type of organ transplanted - organ-specific risks
- Epidemiologic exposure - travel, endemic fungi, TB contacts, foodborne pathogens
- Donor/recipient serostatus - CMV, EBV, Toxo, HBV, HCV
- Current prophylaxis - on TMP-SMX? On valganciclovir?
Investigations:
- Blood cultures (bacterial, fungal)
- CMV/EBV/BK PCR (quantitative)
- BAL + silver stain (PJP)
- Serology: Cryptococcal antigen, Histoplasma antigen (urine/serum)
- Skin biopsy, CSF analysis as appropriate
- High-resolution CT chest (fungal infections)
General Management Principles
- Reduce immunosuppression when life-threatening opportunistic infection occurs (critical for CMV, BK virus, fungal infections, PJP, PTLD)
- Antimicrobial prophylaxis is the cornerstone of prevention (TMP-SMX, valganciclovir, antifungals)
- Pre-transplant screening of donor and recipient for CMV, EBV, TB, HBV, HCV, HIV, Strongyloides, endemic fungi
- Immunization before transplant (live vaccines contraindicated after transplant; inactivated vaccines recommended)
- Multidisciplinary approach - transplant team + infectious disease specialist
- Restart prophylaxis after any episode of acute rejection treatment with pulse steroids or antilymphocyte agents
Recent Evidence (2024-2026)
- CMV pre-emptive therapy vs. prophylaxis: A 2025 Cochrane systematic review (PMID 39807668) compared pre-emptive treatment (treating when CMV PCR rises) vs. universal prophylaxis in solid organ transplant recipients - both strategies remain valid with prophylaxis preferred in highest-risk (D+/R-) patients.
- CMV and rejection: A 2025 systematic review and meta-analysis (PMID 41023683) confirmed that CMV infection independently contributes to acute rejection - reinforcing the importance of aggressive CMV prevention.
Summary for Examination
The key points examiners expect:
- Time-based classification of infections (3 phases) with specific organisms for each
- The concept of "net state of immunosuppression"
- CMV as the most important opportunistic infection - D+/R- as highest risk, valganciclovir prophylaxis, ganciclovir treatment, indirect immunosuppressive effects
- TMP-SMX prophylaxis - covers PJP, Toxoplasma, Listeria, Nocardia, UTIs
- BK virus - unique to renal transplant, BKVAN, reduce immunosuppression (no proven antiviral)
- EBV/PTLD - reduce immunosuppression + Rituximab
- Organ-specific risk patterns (lung = Aspergillus; heart = Toxoplasma; kidney = BK virus)
- Drug interactions: Rifampicin drastically lowers tacrolimus/cyclosporine levels (CYP3A4 induction)
- Pre-transplant screening to prevent reactivation (TB-IGRA, Strongyloides serology, endemic mycosis serology, CMV/EBV status)
- Prophylaxis reset after every rejection episode treated with pulse steroids
Sources: Harrison's Principles of Internal Medicine 22E (2025); Comprehensive Clinical Nephrology 7th Ed.; Mulholland & Greenfield's Surgery 7th Ed.; National Kidney Foundation Primer on Kidney Diseases 8th Ed.; Fishman's Pulmonary Diseases & Disorders
This is a shared conversation. Sign in to Orris to start your own chat.