Which food is good for patients after prolong starvation
Reading File
Finding Sources
Finding Sources
Searching the Web
refeeding syndrome prolonged starvation food recommendations management
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Here is a thorough, clinically grounded answer on feeding after prolonged starvation:
Nutrition After Prolonged Starvation
The Core Danger: Refeeding Syndrome
Before discussing what to eat, the single most important concept is refeeding syndrome - a potentially fatal condition that occurs when food (especially carbohydrates) is reintroduced too quickly after prolonged starvation (>5 days). It was first reported after World War II when severely malnourished prisoners were rapidly refed and experienced sudden death.
Why does it happen?
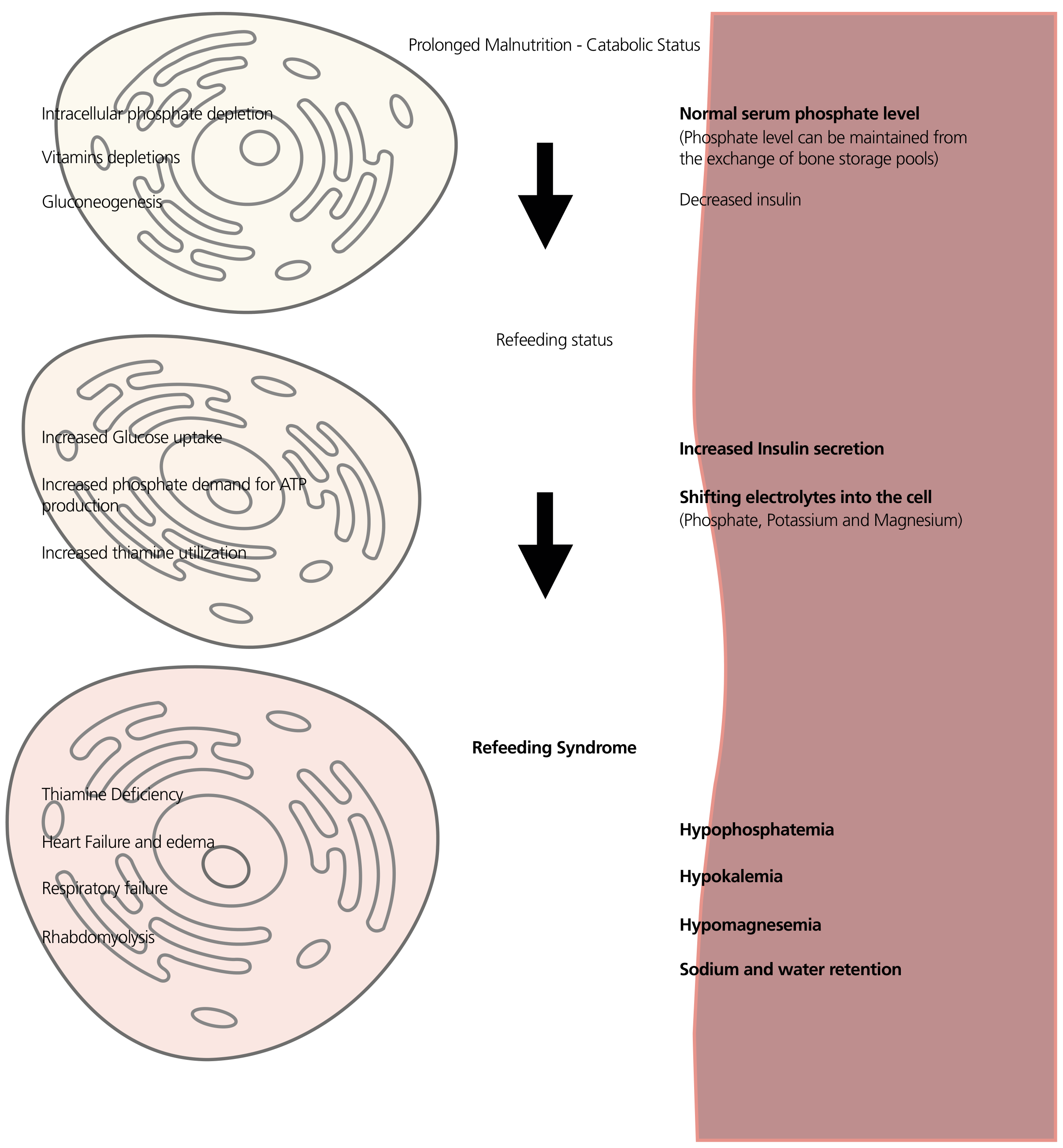
During starvation, the body depletes intracellular electrolytes (phosphate, potassium, magnesium) and shifts to fat and amino acids as fuel. Serum electrolyte levels can appear falsely normal. When carbohydrates are reintroduced:
- Insulin surges
- Phosphate, potassium, and magnesium shift rapidly into cells
- Serum levels drop sharply (hypophosphatemia, hypokalemia, hypomagnesemia)
- Thiamine is rapidly consumed (it's a cofactor for pyruvate dehydrogenase)
- This leads to cardiac arrhythmias, respiratory failure, heart failure, edema, rhabdomyolysis, and confusion (- Yamada's Textbook of Gastroenterology, p. 548; - Schwartz's Principles of Surgery, p. 126)
Step-by-Step Refeeding Approach
Step 1 - Before any food: Correct electrolytes and give thiamine
- Check and correct serum phosphate, potassium, magnesium, and glucose BEFORE starting feeding
- Give thiamine (vitamin B1) BEFORE the first meal - this is mandatory to prevent Wernicke's encephalopathy
- Supplement thiamine 100-300 mg IV/orally
Step 2 - Start very slowly (Days 1-2)
- Begin at 10-20 kcal/kg/day (about 50% of estimated energy needs), or even less than 10 kcal/kg/day for the most severely malnourished (BMI ≤14, or no intake for >2 weeks)
- The ASPEN guidelines recommend starting with 100-150 g of dextrose or 10-20 kcal/kg in the first 24 hours
- Increase by ~33% every 1-2 days as tolerated
- Monitor electrolytes every 12 hours for the first 3 days
Step 3 - Food choices (oral refeeding)
Preferred foods to start with:
| Food Type | Why? |
|---|---|
| Small amounts of complex carbohydrates (oatmeal, rice, bread) | Slower glucose rise vs. simple sugars; avoid triggering a large insulin spike |
| Protein-rich foods (eggs, lentils, fish, chicken) | Help preserve lean mass; lower glycemic effect |
| Phosphate-rich foods (milk, dairy, nuts, whole grains) | Help counteract hypophosphatemia |
| Potassium-rich foods (bananas, potatoes, avocado) | Support potassium repletion |
| Thiamine-rich foods (whole grains, legumes) | Replenish B1 |
| Oral rehydration salts / electrolyte drinks | Correct fluid-electrolyte deficits |
Avoid initially:
- Large sugary meals, sweets, fruit juices - these cause a rapid insulin surge and can precipitate refeeding syndrome
- High-sodium foods (can worsen sodium and fluid retention)
- Very high-calorie meals in the first few days
Step 4 - Gradual increase over 4-7 days
- Advance diet slowly to full caloric needs over the first week
- Monitor vitals, fluid balance, and electrolytes continuously
- In hospital settings, enteral nutrition (tube feeds) is preferred over parenteral (IV) if the gut is functional
Who Is at High Risk?
High-risk groups requiring the most cautious refeeding include:
- BMI < 18.5 with significant weight loss
- Little or no food intake for > 5 days
- Patients with anorexia nervosa, alcoholism, or prolonged illness
- Those with low baseline phosphate, potassium, or magnesium
Key Take-Home Points
- Thiamine first, always - before any carbohydrate is given
- Start low, go slow - 50% of needs on day 1, build up over a week
- Avoid high-sugar foods first - they cause the worst insulin spikes
- Protein + complex carbs + electrolyte-rich foods are the safest initial choices
- Monitor electrolytes closely especially phosphate, potassium, and magnesium
Sources: Schwartz's Principles of Surgery (11th ed.), p. 126; Yamada's Textbook of Gastroenterology (7th ed.), p. 548; NICE refeeding guidelines; ASPEN consensus recommendations
This is a shared conversation. Sign in to Orris to start your own chat.