Role of pediatrician in anc
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Now I have enough to provide a comprehensive answer. The textbooks confirmed that antenatal counseling is the first step in neonatal resuscitation planning. Let me now synthesize a thorough answer from my medical knowledge combined with textbook evidence.
Role of the Pediatrician in Antenatal Care (ANC)
The pediatrician — or neonatologist — has a distinct and important role during the antenatal period that is separate from obstetric care. This role centers on preparing for the newborn, counseling the family about anticipated fetal/neonatal conditions, and coordinating delivery-room readiness.
1. Antenatal Counseling (the Primary Role)
As shown in the Neonatal Resuscitation Algorithm, antenatal counseling is the first step before any delivery:
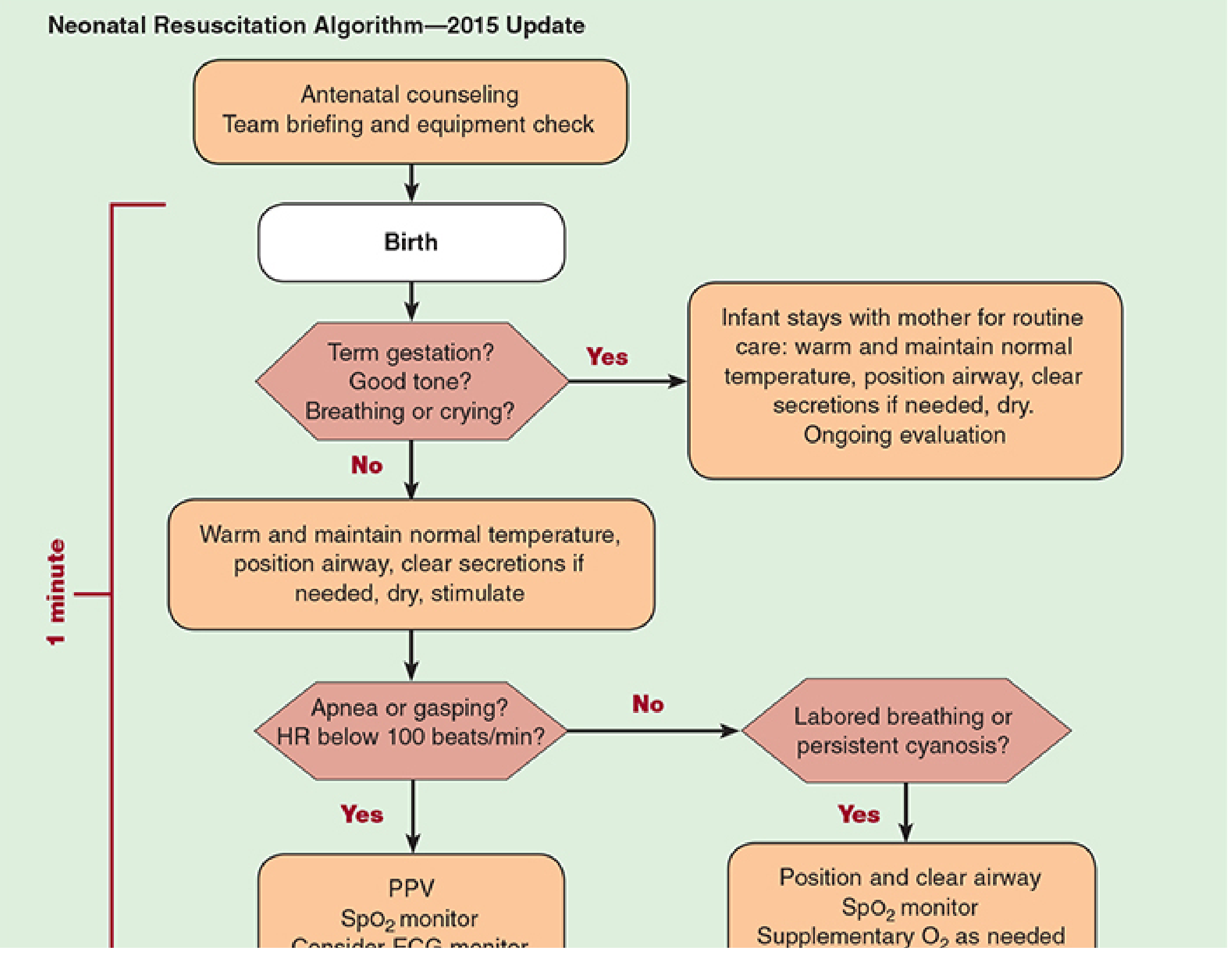
This involves:
- Team briefing and equipment check prior to every high-risk delivery
- Reviewing maternal history, gestational age, fetal anomalies detected on antenatal ultrasound, and expected complications
2. High-Risk Pregnancy Consultation
A pediatrician/neonatologist is specifically called for antenatal consultation when the obstetrician anticipates:
| Maternal Condition | Neonatal Risk Requiring Pediatric Input |
|---|---|
| Pregestational/gestational diabetes | Macrosomia, hypoglycemia, RDS, congenital anomalies |
| Maternal thyroid disease (Graves') | Neonatal hyperthyroidism/hypothyroidism |
| Hypertension / Pre-eclampsia | Preterm birth, IUGR, thrombocytopenia |
| Infections (TORCH, GBS, HIV) | Congenital infection, prophylaxis planning |
| Polyhydramnios/oligohydramnios | GI atresias, renal anomalies |
| Multiple pregnancy | Prematurity, TTTS |
| Substance abuse / medications | Neonatal abstinence syndrome |
3. Counseling Regarding Resuscitation at the Limits of Viability
One of the most critical roles is counseling parents when delivery is anticipated before 25 weeks of gestation. The American Academy of Pediatrics (AAP) recommends:
- Discussion of prognosis at each gestational age (22–25 weeks)
- Parent-centered decision making regarding resuscitation vs. comfort care
- Documentation of antenatal consultation in the chart
- Per Mulholland & Greenfield's Surgery: "Antenatal counseling regarding resuscitation and intensive care before 25 weeks of gestation" is an established standard of care (Cummings J, Committee on Fetus and Newborn. Pediatrics 2015;136(3):588–595)
4. Fetal Anomaly Counseling
When structural anomalies are detected on ultrasound or genetic diagnosis confirms a condition:
- The pediatric surgeon, neonatologist, or relevant subspecialist meets with the family antenatally
- Explains postnatal management plan (e.g., for CDH, orofacial clefts, cardiac defects, renal anomalies)
- Coordinates delivery at an appropriate level of care (tertiary center if needed)
- Example: "Most families find antenatal counseling helpful in planning for care of the child with an orofacial cleft" — Cummings Otolaryngology Head and Neck Surgery
5. Planning for Delivery Room Readiness
Based on the antenatal consultation, the pediatrician/neonatologist:
- Ensures appropriate resuscitation equipment is available and functional
- Assembles the resuscitation team (at least one provider whose sole responsibility is care of the newborn must be present at every delivery)
- Plans for surfactant therapy, intubation, umbilical line placement in anticipated preterm deliveries
- Arranges NICU bed and transport if necessary
6. Anticipatory Guidance to Parents
The pediatrician counsels expectant parents on:
- Breastfeeding preparation and lactation support
- Newborn screening (metabolic, hearing, critical CHD)
- Immunization schedule starting at birth (Hepatitis B, BCG)
- Safe sleep practices (back to sleep, avoiding co-sleeping)
- Neonatal jaundice recognition
- Vitamin K and eye prophylaxis at birth
- Signs of neonatal illness requiring urgent care
7. Antenatal Genetic Counseling (Collaborative)
When chromosomal or genetic conditions are diagnosed prenatally:
- The clinical geneticist and pediatric specialist jointly counsel the family
- Explain natural history, management options, recurrence risks, and prognosis
- Coordinate multidisciplinary team for delivery (Emery's Elements of Medical Genetics and Genomics)
Summary
| Domain | Pediatrician's Role in ANC |
|---|---|
| High-risk cases | Antenatal consultation and risk communication |
| Limits of viability | Counseling on resuscitation decisions (<25 weeks) |
| Fetal anomalies | Subspecialty counseling and delivery planning |
| Delivery room | Team briefing, equipment, resuscitation readiness |
| Parent education | Newborn care, feeding, immunization, safe sleep |
| Genetics | Collaborative counseling for chromosomal conditions |
The overarching principle is that the pediatrician's antenatal role is preventive and preparatory — anticipating neonatal complications, empowering parents with accurate information, and ensuring the team is ready to provide optimal care from the moment of birth.
References:
- Morgan and Mikhail's Clinical Anesthesiology, 7e — Neonatal Resuscitation
- Creasy & Resnik's Maternal-Fetal Medicine — Antenatal Monitoring
- Cummings Otolaryngology — Prenatal Diagnosis
- Mulholland & Greenfield's Surgery — citing AAP Committee on Fetus and Newborn, Pediatrics 2015
Birth asphyxia pediatrics
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have rich, detailed content from multiple authoritative textbooks. Let me compile a comprehensive answer.
Birth Asphyxia (Perinatal/Neonatal Asphyxia)
Definition
Birth asphyxia refers to impaired gas exchange around the time of delivery resulting in hypoxemia (↓O₂), hypercapnia (↑CO₂), and metabolic acidosis. The resulting brain injury is termed Hypoxic-Ischemic Encephalopathy (HIE).
Severe fetal acidemia = umbilical artery pH < 7.00 (associated with increased risk of adverse neurologic outcome).
"Nearly 25% of neonatal deaths worldwide result from birth asphyxia." — Tintinalli's Emergency Medicine
Epidemiology
- Incidence of HIE: 3–5 per 1000 live births in developed countries (stable despite advances in monitoring)
- Mortality: ~20% in the neonatal period
- Neurodevelopmental disability in survivors: ~25%
- Only 10% of all childhood brain injuries are attributable to intrapartum events — the majority are prenatal in origin
(Adams and Victor's Principles of Neurology, 12th Ed; Creasy & Resnik's Maternal-Fetal Medicine)
Etiology / Risk Factors
Antepartum:
- Gestational diabetes mellitus
- Intrauterine growth restriction (IUGR)
- Pre-eclampsia / pregnancy-induced hypertension
- Multiple pregnancy
Intrapartum (Sentinel Events):
- Placental abruption
- Uterine rupture
- Cord accident (prolapse, tight nuchal cord)
- Maternal cardiac arrest
- Non-reassuring fetal heart rate tracing
- Meconium-stained amniotic fluid
At Delivery:
- Need for resuscitation; low Apgar scores
- Medications used during labor (including anesthetic agents)
- Birth trauma
(Bradley and Daroff's Neurology in Clinical Practice; Creasy & Resnik's)
Pathophysiology
The injury occurs in two phases:
Phase 1 — Primary Energy Failure:
- ↓ Cerebral blood flow → Hypoxia → Switch from oxidative phosphorylation to anaerobic metabolism
- Depletion of high-energy phosphates (ATP)
- Lactic acid accumulation → metabolic acidosis
- Cellular dysfunction and death
Phase 2 — Secondary (Reperfusion) Injury:
- Transient return of cerebral metabolism → followed by secondary energy failure
- Excitotoxicity (glutamate release), apoptosis, reactive oxygen species, inflammation
- Intracellular Ca²⁺ influx, lipid peroxidation, nitric oxide accumulation
Most vulnerable regions: Rolandic cortex, thalamus, and basal ganglia (highest metabolic demands)
This secondary phase is the therapeutic window for neuroprotection (targeting it with therapeutic hypothermia).
(Creasy & Resnik's; Bradley and Daroff's Neurology)
Clinical Presentation — Sarnat Staging System (1976)
| Feature | Stage 1 (Mild) | Stage 2 (Moderate) | Stage 3 (Severe) |
|---|---|---|---|
| Level of Consciousness | Hyperalert, irritable, jittery | Lethargic, obtunded | Stupor / Coma |
| Tone | Normal / mild ↑ head lag | Hypotonic | Flaccid |
| Primitive Reflexes | Exaggerated | Suppressed | Absent |
| Seizures | Rare | Common (onset < 24 h) | Uncommon (severe depression) |
| Brain Stem Dysfunction | Rare | Rare | Common |
| Raised ICP | Rare | Rare | Variable |
| Respirations | Normal | May need support | Irregular, needs ventilation |
| Duration | < 24 hours | > 24 hours (variable) | > 5 days |
| Poor outcome (%) | 0% | 20–40% | >80% (death or disability) |
(The Harriet Lane Handbook, 23rd ed.; Adams and Victor's Neurology)
Diagnosis
Clinical criteria (ACOG/AAP, reaffirmed 2020):
- Clinical features of neonatal encephalopathy (↓consciousness, seizures, ↓tone/reflexes, respiratory depression) at ≥ 35 weeks gestation
- Neonatal signs consistent with acute peripartum/intrapartum event:
- Apgar score < 5 at 5 and 10 minutes
- Umbilical artery pH < 7.0 or base deficit ≥ 12 mmol/L
- Acute brain injury on MRI consistent with hypoxia-ischemia (deep gray matter or watershed injury)
- Multisystem organ failure
- Sentinel hypoxic/ischemic event occurring immediately before or during labor
- Developmental outcome: spastic quadriplegia or dyskinetic cerebral palsy
Blood gases:
- Cord pH < 7.0 = severe acidemia; 340-fold increased risk of seizures when combined with 5-min Apgar ≤5 and delivery room intubation
(Creasy & Resnik's)
Neuroimaging
| Modality | Role |
|---|---|
| MRI (Diffusion-weighted) | Gold standard; detects reduced water diffusivity within 24–48 hours; identifies deep gray matter or watershed injury |
| MR Spectroscopy | Detects altered metabolites (↑lactate, ↓N-acetyl aspartate) indicating injury |
| Cranial Ultrasound | Preferred initial study for preterm infants; detects IVH and periventricular injury |
| CT | Alternative initial study for term infants when MRI not feasible |
| EEG/aEEG | Detects subclinical seizures; voltage suppression = poor prognosis |
(Creasy & Resnik's; Adams and Victor's)
Multiorgan Injury
Systemic ischemia causes injury beyond the brain:
| Organ | Consequence |
|---|---|
| Kidney | Acute tubular necrosis → oliguria, azotemia |
| GI tract | Luminal ischemia → ↑risk of NEC |
| Lung | ↓Pulmonary blood flow → PPHN |
| Liver | Hepatocellular injury → hypoglycemia, DIC |
| Electrolytes | SIADH → hyponatremia; ↓PTH → hypocalcemia, hypomagnesemia |
| Heart | Electrolyte abnormalities + direct injury → myocardial dysfunction |
| Muscle | Rhabdomyolysis |
(Creasy & Resnik's Maternal-Fetal Medicine)
Management
A. Immediate — Delivery Room (NRP Algorithm)
- Antenatal counseling + team briefing before high-risk delivery
- Neonatal resuscitation as per NRP: warmth, airway, PPV, chest compressions, medications
- At least one qualified provider whose sole role is neonatal care must be present at every delivery
B. Passive Cooling (while transfer is arranged)
- Turn off the radiant warmer; do NOT actively cool
- Aim rectal temp 33–34°C during transport
C. Therapeutic Hypothermia (TH) — Standard of Care
Indication: Gestational age ≥ 35 weeks + evidence of HIE + within 6 hours of delivery
Criteria for initiating TH (any one of):
- Cord gas or 1-hour blood gas: pH < 7.0 or base deficit > 16
- If pH 7.01–7.15 / BD 10–15.9: need additional criteria (10-min Apgar ≤5 OR need for assisted ventilation ≥10 min)
Protocol:
- Target temperature: 33°C–35°C for 72 hours
- Method: whole-body cooling or selective head cooling
- Must be performed at experienced comprehensive neonatal centers
Evidence: Meta-analysis of 11 RCTs → statistically significant reduction in death or major neurodevelopmental disability at 18 months. Number Needed to Treat (NNT) = 7.
(Harriet Lane Handbook; Creasy & Resnik's; Rosen's Emergency Medicine)
D. Supportive Care
- Treat seizures (phenobarbital first line; phenytoin/levetiracetam second line)
- Correct hypoglycemia (hypoglycemia worsens HIE outcomes)
- Correct hypocalcemia, hyponatremia
- Avoid hyperoxia — titrate oxygen to SpO₂ 91–95%
- Treat PPHN if present (iNO, sildenafil)
- Monitor and support cardiac, renal, hepatic, and GI function
Prognosis
| Sarnat Stage | Outcome |
|---|---|
| Stage 1 (Mild) | Normal in virtually all cases |
| Stage 2 (Moderate) | 20–40% risk of long-term neurologic compromise |
| Stage 3 (Severe) | >80% risk of death or severe disability |
Long-term sequelae: Cerebral palsy (spastic/dyskinetic), epilepsy, intellectual disability, developmental delay, cortical visual impairment.
"Resolution of moderate encephalopathy by day 5 of life is associated with appropriate short-term neurodevelopmental outcome; persistence beyond 7 days is associated with death or severe disability." — Bradley and Daroff's Neurology
Key Points to Remember
- Birth asphyxia = HIE; caused by impaired gas exchange → hypoxia + ischemia + acidosis
- Sarnat staging guides prognosis and management decisions
- Therapeutic hypothermia (33–35°C × 72 h) is the only proven neuroprotective intervention — must start within 6 hours of delivery
- Systemic multi-organ injury always accompanies severe HIE — assess all organ systems
- MRI (DWI) is the gold standard for imaging brain injury
- The secondary (reperfusion) injury phase is the therapeutic target
References:
- Creasy & Resnik's Maternal-Fetal Medicine — Definition, Pathophysiology, Therapeutic Hypothermia
- Adams and Victor's Principles of Neurology, 12th Ed — Sarnat Staging, Neuropathology
- The Harriet Lane Handbook, 23rd Ed — Diagnostic Criteria, TH Protocol
- Bradley and Daroff's Neurology in Clinical Practice — Diagnosis, Prognosis
- Tintinalli's Emergency Medicine — Epidemiology, Resuscitation
- Morgan and Mikhail's Clinical Anesthesiology, 7e — NRP Algorithm
Birth asphyxia pediatrics
The previous response already covered this topic in depth. Here's the complete reference summary from that answer — no need to re-research:
Birth Asphyxia (Perinatal HIE) — Quick Reference
Definition
Impaired gas exchange at/around delivery → hypoxemia + hypercapnia + metabolic acidosis → Hypoxic-Ischemic Encephalopathy (HIE)
Severe fetal acidemia = umbilical artery pH < 7.00
Incidence: 3–5 per 1000 live births | Mortality: ~20% | Disability in survivors: ~25%
Pathophysiology (Two-Phase Injury)
Phase 1 — Primary Energy Failure
- ↓ CBF → anaerobic metabolism → ATP depletion → lactic acidosis → cell death
Phase 2 — Secondary (Reperfusion) Injury ← Therapeutic target
- Excitotoxicity (glutamate), apoptosis, reactive oxygen species, inflammation, intracellular Ca²⁺ influx
Most vulnerable brain regions: Basal ganglia, thalamus, Rolandic cortex
Sarnat Staging & Prognosis
| Feature | Stage 1 (Mild) | Stage 2 (Moderate) | Stage 3 (Severe) |
|---|---|---|---|
| Consciousness | Hyperalert, jittery | Lethargic | Stupor / Coma |
| Tone | Normal / ↑ head lag | Hypotonic | Flaccid |
| Reflexes | Exaggerated | Suppressed | Absent |
| Seizures | Rare | Common (< 24 h) | Uncommon |
| Brainstem Dysfunction | Rare | Rare | Common |
| Duration | < 24 hr | > 24 hr | > 5 days |
| Poor Outcome | 0% | 20–40% | > 80% |
Diagnosis (ACOG/AAP Criteria — reaffirmed 2020)
All four steps required to link intrapartum event to neurologic outcome:
- Neonatal encephalopathy at ≥ 35 weeks gestation (↓consciousness, ↓tone, seizures, respiratory depression)
- Neonatal signs of acute peripartum event:
- Apgar < 5 at 5 and 10 min
- UA pH < 7.0 or base deficit ≥ 12 mmol/L
- MRI showing deep gray matter / watershed injury
- Multisystem organ failure
- Sentinel event during/just before labor (abruption, cord accident, uterine rupture)
- Outcome: Spastic quadriplegia or dyskinetic cerebral palsy
340-fold ↑ risk of seizures when 5-min Apgar ≤5 + delivery-room intubation + UA pH < 7.00 are all present
Multiorgan Injury
| Organ | Consequence |
|---|---|
| Brain | HIE, seizures |
| Kidney | ATN → oliguria, azotemia |
| Lung | PPHN |
| GI | NEC risk ↑ |
| Liver | Hypoglycemia, DIC |
| Electrolytes | Hyponatremia (SIADH), hypocalcemia (↓PTH), hypomagnesemia |
| Heart | Myocardial dysfunction |
| Muscle | Rhabdomyolysis |
Management
1. Delivery Room — NRP Algorithm
- Antenatal counseling + team briefing (first step in NRP)
- Warmth → Airway → Breathing (PPV) → Circulation (chest compressions) → Drugs
- At least one dedicated provider for newborn at every delivery
2. Therapeutic Hypothermia (TH) ← Only proven neuroprotective therapy
Eligibility: GA ≥ 35 weeks + HIE evidence + within 6 hours of birth
Criteria (any one):
- Cord/1-hour blood gas: pH < 7.0 or base deficit > 16
- pH 7.01–7.15 / BD 10–15.9 + additional criterion (10-min Apgar ≤5 OR ventilation ≥10 min)
- Moderate–severe encephalopathy on clinical exam
Protocol: 33–35°C × 72 hours (whole-body or head cooling)
Evidence: 11 RCTs meta-analysis → significant ↓ death or major neurodevelopmental disability at 18 months. NNT = 7
3. Supportive Care
| Problem | Management |
|---|---|
| Seizures | Phenobarbital (1st line) → phenytoin / levetiracetam |
| Hypoglycemia | IV glucose (worsens outcome if untreated) |
| Hypocalcemia | IV calcium gluconate |
| Hyponatremia | Fluid restriction (SIADH) |
| PPHN | iNO, sildenafil, HFOV |
| Oxygenation | Target SpO₂ 91–95%; avoid hyperoxia |
| Cardiac | Inotropes if needed |
Neuroimaging
| Modality | When / Role |
|---|---|
| MRI-DWI | Gold standard; detects injury within 24–48 h; watershed vs. deep gray matter pattern |
| MR Spectroscopy | ↑Lactate, ↓NAA = injury marker |
| Cranial USG | Initial study in preterm; detects IVH, PVL |
| CT | Alternative for term infant when MRI unavailable |
| aEEG/EEG | Subclinical seizures; voltage suppression = poor prognosis |
Long-Term Sequelae
- Cerebral palsy (spastic quadriplegia, dyskinetic CP)
- Epilepsy
- Intellectual disability
- Developmental delay
- Cortical visual impairment
Resolution of moderate encephalopathy by day 5 → favorable short-term outcome; persistence beyond 7 days → death or severe disability (Bradley and Daroff's Neurology)
References: Creasy & Resnik's Maternal-Fetal Medicine | Adams and Victor's Principles of Neurology, 12th Ed | The Harriet Lane Handbook, 23rd Ed | Bradley and Daroff's Neurology in Clinical Practice | Tintinalli's Emergency Medicine | Morgan and Mikhail's Clinical Anesthesiology, 7e
Ntep psm
Finding Sources
Searching the Web
NTEP National Tuberculosis Elimination Programme India PSM 2025
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Ntep psm
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Glomus tumor ENT
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive textbook data. Let me compile the full answer.
Glomus Tumors in ENT (Paragangliomas of the Head and Neck)
Definition & Overview
Glomus tumors (also called paragangliomas or chemodectomas) are benign, highly vascular, slow-growing neoplasms arising from paraganglion (neural crest) tissue associated with the autonomic nervous system. In the temporal bone, they are the most frequently encountered temporal bone neoplasms after acoustic neuromas.
They are named by their anatomical site of origin:
| Name | Site of Origin |
|---|---|
| Glomus tympanicum | Glomus bodies of the middle ear (cochlear promontory, Jacobson's nerve) |
| Glomus jugulare | Jugular bulb adventitia / Arnold's nerve |
| Jugulotympanicum | Combination of the above two |
| Glomus vagale | Along the vagus nerve in the neck |
| Carotid body tumor | Carotid bifurcation |
"Glomus tympanicum paragangliomas are the most common middle ear tumour." — Scott-Brown's Otorhinolaryngology
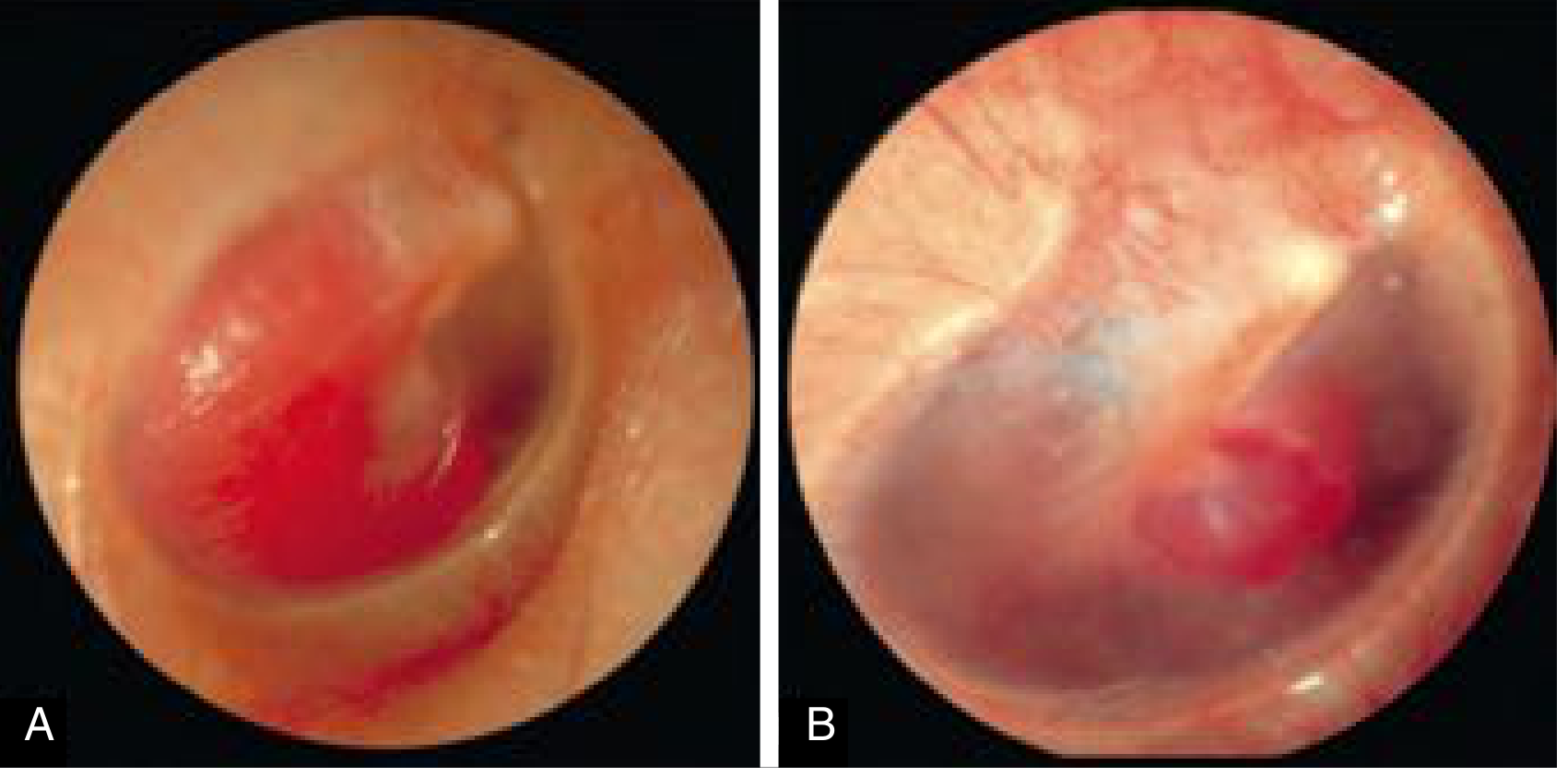
Endoscopic Appearance
The characteristic otoscopic finding — a reddish-blue pulsatile mass behind the tympanic membrane:
Clinical Features
Glomus Tympanicum
- Pulsatile tinnitus (most common presenting symptom)
- Conductive hearing loss
- Small, reddish mass visible behind the tympanic membrane — all borders visible through TM = hallmark
- May be an incidental finding on exam when small
- Causes symptoms early due to proximity to ossicles and TM
Glomus Jugulare
- Pulsatile tinnitus
- Lower cranial nerve palsies (CNs IX, X, XI — "jugular foramen syndrome")
- Dysphagia, hoarseness, shoulder weakness
- CN XII involvement if large
- Facial nerve paresis (extension into mastoid)
- Sensorineural hearing loss (bony erosion of labyrinth)
- Symptoms appear late after considerable growth and bone destruction
- Erosion through TM → bleeding mass in the external auditory canal
Glomus Vagale
- Painless neck mass, vagal neuropathy
Diagnostic Evaluation
1. Otoscopy
- All borders of tumor visible behind TM → glomus tympanicum
- Borders NOT fully visible → may be large tympanicum OR glomus jugulare extending upward
- Associated cranial nerve abnormalities → more likely glomus jugulare
2. CT Scan (High-Resolution)
| Glomus Tympanicum | Glomus Jugulare |
|---|---|
| Soft tissue nodule on cochlear promontory | Permeative bone destruction of the jugulo-carotid spine |
| No ossicular erosion if small | Destroys bony septum between ICA and IJV |
| Well-circumscribed | May extend into middle ear, skull base, posterior fossa |
CT of glomus tympanicum: well-demarcated soft tissue nodule behind TM over the cochlear promontory (Scott-Brown's)
3. MRI (with contrast)
- Classic "salt and pepper" appearance on T1/T2 — combination of:
- Flow voids from intratumoral vessels (pepper)
- Areas of microhemorrhage (salt)
- Gadolinium enhancement is intense
- Defines intracranial extension, relationship to ICA
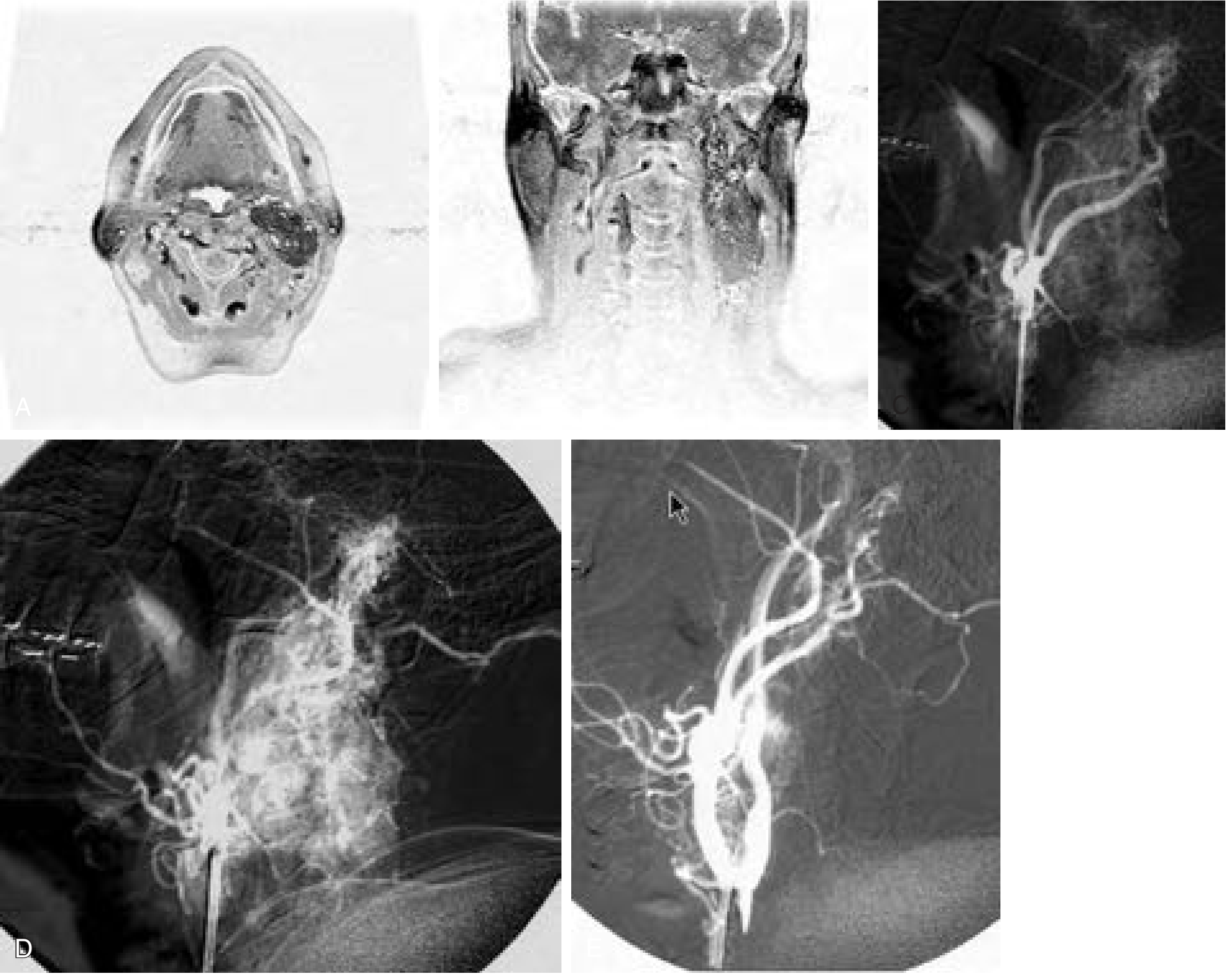
4. Angiography
- Confirms highly vascular nature
- Feeding vessels from external carotid branches: ascending pharyngeal, middle meningeal (posterior division), stylomastoid, posterior auricular
- Performed in the same sitting as preoperative embolization
5. Urine Metanephrines (24-hour urine)
- 1–3% of glomus jugulare tumors are secretory (catecholamine-producing)
- Must be checked before surgery to avoid intraoperative hypertensive crisis
- Careful coordination with anesthesiology required if secreting
Classification Systems
Fisch Classification (Fisch, 1978) — Glomus Jugulare
| Stage | Description |
|---|---|
| A | Limited to the middle ear |
| B | Limited to tympano-mastoid area ± jugular bulb erosion |
| C | Involvement/destruction of infralabyrinthine and apical compartments |
| D1 | Intracranial extension < 2 cm |
| D2 | Intracranial extension > 2 cm |
| D3 | Inoperable intracranial invasion |
Glasscock-Jackson Classification (1982)
| Stage | Description |
|---|---|
| I | Small tumor: jugular bulb, middle ear, mastoid |
| II | Extends under internal auditory canal; possible intracranial extension |
| III | Extends to petrous apex; possible intracranial extension |
| IV | Beyond petrous apex into clivus/infratemporal fossa |
Differential Diagnosis
A "red/blue mass behind the tympanic membrane" must be differentiated from:
- Aberrant ICA (aberrant internal carotid artery — do NOT biopsy!)
- High-riding/dehiscent jugular bulb
- Cholesterol granuloma
- Hemangioma
- Facial nerve schwannoma
- Meningioma
- Metastatic tumors (renal cell, breast, prostate)
Biopsy is contraindicated without prior imaging to exclude vascular lesions.
Treatment
A. Surgical Resection — Primary Treatment
Glomus Tympanicum:
- Small tumors (all borders visible): Transcanal approach
- Larger tumors (borders not fully visible): Endaural or postauricular approach; mastoidectomy with extended facial recess approach
Glomus Jugulare:
- Fisch Type A infratemporal fossa approach — most common
- Staging surgery may be needed for large intracranial extension
- Lower cranial nerve preservation is prioritized — nerve resection may require tracheostomy + gastrostomy
- Preoperative embolization (24–48 hours before surgery) is recommended for any sizeable glomus jugulare tumor:
- Significantly reduces intraoperative blood loss and operative time
- Must be done carefully — some embolization agents can cause cranial neuropathies
B. Radiotherapy — Increasingly Used
- Both conventional radiotherapy (with or without intensity modulation) and stereotactic radiosurgery achieve tumor control rates of 90–100%
- Used for:
- Elderly or medically unfit patients
- Unresectable tumors (Fisch D3)
- Residual or recurrent tumors
- Patient preference
C. Observation ("Watch and Wait")
- For elderly patients with small, slow-growing, asymptomatic tumors
- Serial imaging every 1–2 years
Key Points Summary
| Feature | Glomus Tympanicum | Glomus Jugulare |
|---|---|---|
| Origin | Middle ear glomus bodies | Jugular bulb |
| Most common presentation | Pulsatile tinnitus + CHL | Lower CN palsies + pulsatile tinnitus |
| Symptoms onset | Early (close to TM) | Late (after extensive growth) |
| CT finding | Soft tissue on promontory | Permeative bone destruction |
| MRI | Enhancing mass | Salt-and-pepper pattern |
| Cranial nerve involvement | Rare | CNs IX–XII |
| Surgery | Transcanal / mastoidectomy | Fisch Type A infratemporal fossa |
| Embolization needed | Usually not | Yes, 24–48 h preop |
References:
- Cummings Otolaryngology Head and Neck Surgery — Paraganglioma, Surgical Approach, Radiotherapy
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 2 — Temporal Bone Paragangliomas, Imaging
- Harrison's Principles of Internal Medicine, 22E — Mixed/Conductive Hearing Loss differential
This is a shared conversation. Sign in to Orris to start your own chat.