Preterm labour
Reading File
Finding Sources
Finding Sources
Searching PubMed
"preterm labor" OR "preterm labour"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Here is the full structured answer:
Preterm Labour
Definition: Uterine contractions producing cervical change occurring between 20 and 37 weeks of gestation. Cervical change is defined as a cervix at least 2 cm dilated or 80% effaced, or documented progression on serial examination. Contractions without cervical change do not constitute preterm labour and do not require intervention.
- Textbook of Family Medicine 9e; Morgan and Mikhail's Clinical Anesthesiology 7e
Epidemiology
- Affects approximately 8% of live-born infants in the United States
- Accounts for the majority of neonatal morbidity and mortality
- Racial disparities are significant: Black women have persistently higher rates of preterm birth than White women, even when controlling for socioeconomic factors
Risk Factors
Strongest predictors
| Factor | Relative Risk |
|---|---|
| Prior spontaneous preterm birth | ~2-5x |
| Multiple gestation / polyhydramnios (increased uterine volume) | RR ≥ 6 |
| Short cervix by TVU ≤25 mm at 22-24 weeks | RR 6.5 for PTB <35 wks |
| Uterine anomaly | Elevated |
Maternal factors
- Extremes of age
- Low BMI or, at very early gestations (<28 wks), obesity
- Inadequate prenatal care
- Smoking (RR ~1.3-1.5 for preterm birth)
- Infections: urinary tract, bacterial vaginosis (BV), chorioamnionitis
- African American race
- Short interpregnancy interval
- Prior cervical procedures (LEEP, cone biopsy)
- Stress, physical overexertion
Fetal/uterine factors
- Multiple gestation
- Polyhydramnios
- Uterine malformation
- Fetal anomaly or aneuploidy
- Placental abruption
Creasy & Resnik's Maternal-Fetal Medicine
Prediction
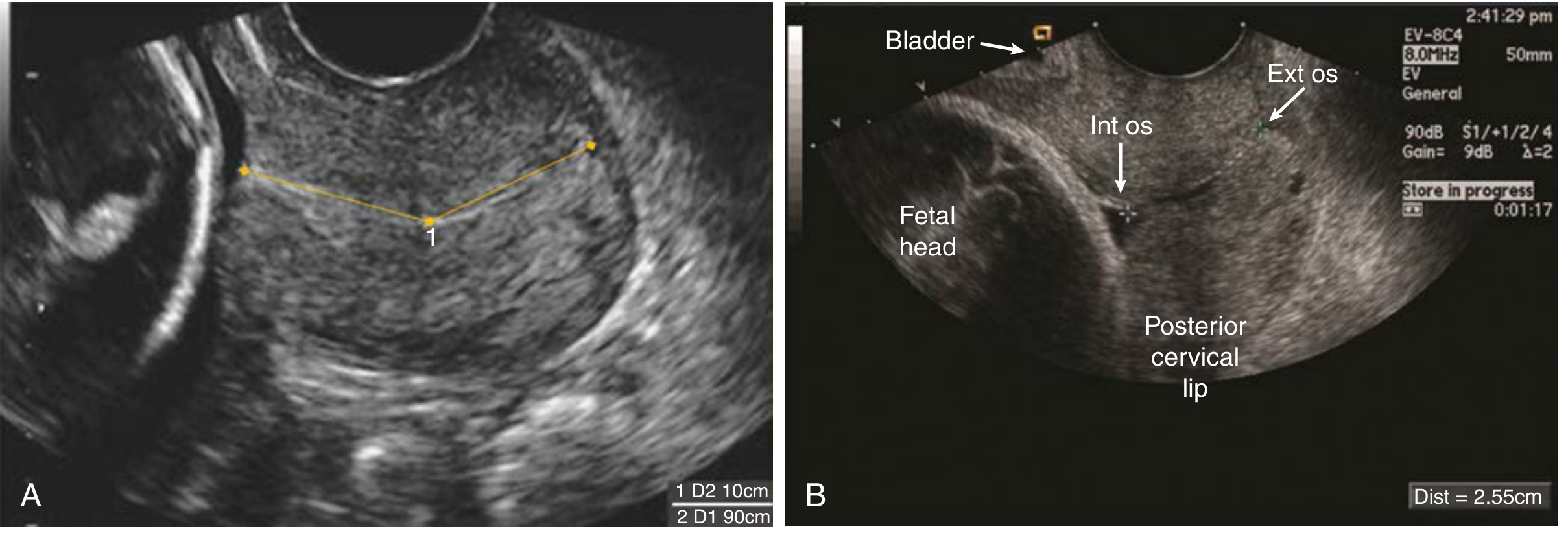
1. Transvaginal Ultrasound (TVU) Cervical Length
The single most useful predictor of spontaneous preterm birth.
Key cut-offs (16-22 weeks, singletons without prior PTB):
- 50th percentile: ~40 mm
- 10th percentile: ~30 mm
- 3rd percentile: ~25 mm
A cervical length ≤25 mm at 22-24 weeks = RR 6.5 for delivery before 35 weeks.
2. Fetal Fibronectin (fFN)
- Collected from cervicovaginal secretions at 22-35 weeks
- Negative result (most clinically useful): Predicts the woman will NOT deliver for at least 7-10 days - high negative predictive value (~99%)
- Positive result warrants closer surveillance or tocolytic consideration
- Contamination from digital exam, intercourse, or blood renders the test invalid - always collect BEFORE digital exam
Textbook of Family Medicine 9e; Creasy & Resnik's
Assessment of a Woman with Suspected Preterm Labour
- Monitoring: Continuous CTG for contractions + FHR in left lateral position
- History and exam: Identify treatable causes; check contraindications to tocolysis
- Speculum exam if membrane rupture suspected - nitrazine test, ferning, GBS/chlamydia/GC cultures
- fFN swab before digital exam (at 22-35 weeks)
- Urinalysis + culture - treat UTI if present
- Digital cervical exam for dilation, effacement, consistency
- Rule out chorioamnionitis: maternal fever, uterine tenderness, leukocytosis, fetal tachycardia
Management
Step 1 - Corticosteroids (the most important intervention)
Betamethasone 12 mg IM every 24 hours x 2 doses (or dexamethasone 6 mg IM every 12 hours x 4 doses)
- Indicated at 24-34 weeks of gestation when preterm delivery is anticipated
- Enhances fetal lung maturity by stimulating surfactant production
- Reduces: RDS (respiratory distress syndrome), intraventricular hemorrhage, necrotizing enterocolitis, neonatal death
- A single rescue course may be given if >2 weeks since original course and <34 weeks
Step 2 - GBS Prophylaxis
Antibiotic prophylaxis for GBS should be administered if preterm delivery is a possibility.
Step 3 - Tocolysis
Goal: Delay delivery by 48-72 hours to allow corticosteroids to take effect. Tocolysis successfully delays birth by 48 hours in ~75% of patients but does not reliably prevent eventual preterm delivery.
Contraindications to tocolysis:
- Chorioamnionitis
- Abruptio placentae / heavy vaginal bleeding
- Fetal demise or severe fetal compromise
- Severe or uncontrolled hypertension
- Maternal haemodynamic instability
| Agent | Mechanism | Dosing | Key Side Effects |
|---|---|---|---|
| Nifedipine (calcium channel blocker) - preferred first-line | Blocks calcium entry into myometrium | 20 mg oral load, then 10-20 mg every 4-6h | Maternal hypotension, flushing, tachycardia. Avoid in hypotension. |
| Indomethacin (COX inhibitor / NSAID) | Reduces prostaglandin synthesis | 50-100 mg loading, then 25-50 mg every 4-6h | Premature closure of ductus arteriosus (use <32 weeks only), oligohydramnios from fetal renal impairment |
| Magnesium sulfate (MgSO4) | Antagonises calcium-mediated myometrial contraction | 6 g IV loading dose, then 2-4 g/h IV | Maternal: flushing, nausea, respiratory depression at toxic levels; potentiates muscle relaxants |
| Terbutaline (β2-agonist) | Stimulates β2 receptors, relaxes myometrium | 0.25 mg SQ every 20-30 min (acute) | Tachycardia, arrhythmias, myocardial ischaemia, hyperglycaemia, hypokalaemia, pulmonary oedema (avoid prolonged use; FDA warned against oral/SQ maintenance terbutaline) |
| Atosiban (oxytocin receptor antagonist) | Blocks oxytocin/vasopressin receptors | IV bolus + infusion | Minimal maternal side effects; not available in USA |
Important notes:
- Indomethacin risk of ductal constriction is mostly reversible on stopping the drug; generally avoid after 32 weeks
- Hypokalaemia with β-agonists is usually due to intracellular shift and rarely requires treatment, but increases sensitivity to muscle relaxants
- Maintenance tocolysis beyond the initial 48-hour window does not improve outcomes and is not recommended
Morgan and Mikhail's Clinical Anesthesiology 7e; Textbook of Family Medicine 9e; Creasy & Resnik's
Step 4 - Magnesium for Neuroprotection (separate from tocolysis)
MgSO4 given for fetal neuroprotection at <32 weeks of gestation reduces risk of cerebral palsy in surviving preterm infants. Dosing is institution-specific (typically 4-6 g IV bolus + 1-2 g/h infusion until delivery).
Prevention
Progesterone therapy
- Vaginal progesterone (200 mg/night or 90 mg gel daily): Recommended for singletons with short cervix ≤25 mm at 16-24 weeks without prior PTB. Reduces rate of PTB by ~40-45%.
- 17-hydroxyprogesterone caproate (17-OHPC) IM: Previously recommended for patients with prior spontaneous PTB. Recent large trial (PROLONG) failed to show benefit; use is now debated. Notably, 17-OHPC is less effective in women with BMI ≥30 kg/m².
- Neither formulation is recommended for multifetal gestations.
Cervical cerclage
Indicated in:
- History-indicated cerclage: 3+ second-trimester pregnancy losses or prior PTBs due to cervical insufficiency - placed at 12-14 weeks
- Ultrasound-indicated cerclage: Singleton + prior PTB + current cervical length <25 mm at 16-23+6 weeks
- Physical/emergency cerclage: Dilated, prolapsing membranes on speculum exam
Contraindications: Active labour, chorioamnionitis, abruption, pPROM, fetal compromise.
Lifestyle / Screening
- Smoking cessation
- Treatment of asymptomatic bacteriuria
- Routine screening and treatment for BV in low-risk women does not reliably reduce PTB
- Activity restriction / bed rest: Evidence does NOT support benefit and may increase risk of PTB
Creasy & Resnik's Maternal-Fetal Medicine
Complications of Prematurity
| System | Complication |
|---|---|
| Pulmonary | RDS (hyaline membrane disease) - inadequate surfactant; mainly <35 weeks |
| Neurological | Intraventricular haemorrhage (IVH); periventricular leukomalacia; cerebral palsy |
| GI | Necrotising enterocolitis (NEC) |
| Ophthalmologic | Retinopathy of prematurity |
| Thermal | Hypothermia (poor subcutaneous fat) |
| Metabolic | Hypoglycaemia, hypocalcaemia |
| Haematologic | Anaemia, jaundice |
| Obstetric | Umbilical cord prolapse (especially with breech + PROM); soft cranium predisposes to ICH during vaginal delivery |
Infants <30 weeks or <1500 g experience the greatest burden of complications.
Preterm Premature Rupture of Membranes (PPROM)
PPROM complicates ~1/3 of premature deliveries. The combination of PPROM + preterm labour increases risk of cord compression, fetal hypoxaemia, and ascending infection. Management is modified based on gestational age:
- <34 weeks: Expectant management, corticosteroids, antibiotics (latency antibiotics - ampicillin + erythromycin/azithromycin), GBS prophylaxis, MgSO4 neuroprotection if <32 weeks
- ≥34 weeks: Delivery generally preferred
- Tocolysis in PPROM is generally not recommended beyond allowing corticosteroid effect
Anesthesia Considerations in Preterm Labour
- Epidural/spinal anesthesia promotes pelvic relaxation and is preferred for vaginal delivery
- Aim for slow, controlled delivery with minimal maternal expulsive effort; episiotomy and low forceps may assist
- Residual β-agonist effects may complicate general anaesthesia: use ketamine, ephedrine, and isoflurane cautiously
- Magnesium potentiates non-depolarising muscle relaxants - reduce doses accordingly
- Hypokalaemia from β-agonists increases muscle relaxant sensitivity
Morgan and Mikhail's Clinical Anesthesiology 7e; Barash Clinical Anesthesia 9e
Principle in management of preterm labour
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have rich, detailed content. Let me compile the full answer on principles in management of preterm labour.
Principles in Management of Preterm Labour
The management of preterm labour rests on a small number of core principles, each targeting a specific and measurable goal. These principles apply from the moment preterm labour is confirmed through to delivery planning.
Principle 1: Confirm the Diagnosis Before Intervening
Before any treatment is started, active preterm labour must be confirmed. Over-treatment of women who are not in true preterm labour is a real clinical problem.
- Diagnosis requires: Regular uterine contractions plus documented cervical change (≥2 cm dilation, ≥80% effacement, or progression on serial exams)
- Contractions without cervical change do not warrant tocolytic therapy; initiating tocolysis for unconfirmed preterm labour is actively discouraged
- Assess with: CTG, digital cervical exam (after excluding PROM), and fetal fibronectin (fFN) swab at 22-35 weeks before digital exam
- Negative fFN = delivery within 7-10 days extremely unlikely (very high NPV) - can safely avoid treatment
- Exclude PROM with sterile speculum exam, nitrazine, and ferning before digital exam
"Initiation of tocolytic therapy for potential but unconfirmed preterm labor is discouraged." - Mulholland & Greenfield's Surgery 7e
Principle 2: Identify and Treat Reversible Causes
Uterine, cervical, and urinary tract infections account for 20-40% of preterm labour cases. Before reaching for tocolytics, basic corrective steps must be taken:
- Supplemental oxygen - uterine hypoxia can itself drive contractions
- IV crystalloid hydration (500 mL) - dehydration is a common precipitant; can reduce contraction frequency
- Left lateral decubitus position - improves uterine and placental perfusion
- Urinalysis + culture - treat UTI/pyelonephritis promptly
- Rule out chorioamnionitis: fever, uterine tenderness, maternal/fetal tachycardia, leukocytosis, purulent discharge
- Screen for GBS, Chlamydia, GC, bacterial vaginosis
- If contractions persist after these measures and cervical change is confirmed, proceed to pharmacologic therapy
"Because uterine, cervical, or urinary tract infections account for 20% to 40% of cases of preterm labor, search for a specific cause and treat infections appropriately." - Roberts & Hedges' Clinical Procedures in Emergency Medicine
Principle 3: Assess Contraindications to Labour Arrest
Stopping preterm labour is NOT always appropriate. Before any tocolysis, confirm there is no indication for prompt delivery.
Absolute contraindications to tocolysis:
| Maternal | Fetal |
|---|---|
| Chorioamnionitis | Gestational age >37 weeks |
| Severe preeclampsia / eclampsia | Fetal compromise requiring delivery |
| Abruptio placentae / significant haemorrhage | Lethal fetal anomaly |
| Placenta praevia with haemorrhage | Fetal demise |
| Maternal haemodynamic instability | Chorioamnionitis |
| Significant maternal cardiac disease |
Relative contraindications: vaginal bleeding, poorly controlled hypertension, maternal diabetes with complications.
- Vaginal spotting from cervical effacement is acceptable, but anything beyond light spotting must prompt exclusion of abruption and praevia
- In extreme prematurity with borderline haemorrhage, short-term tocolysis to gain corticosteroid benefit may occasionally be considered with caution
Principle 4: Delay Delivery by 48-72 Hours (the actual goal of tocolysis)
Tocolytics do NOT prevent preterm birth. Their only proven, clinically meaningful goal is to buy 48-72 hours to:
- Administer antenatal corticosteroids (which need ~24 hours to work)
- Transfer the mother to a tertiary facility with neonatal ICU capability
- Administer MgSO4 for neuroprotection
"Although tocolytic agents delay delivery in approximately 80% of women, they neither prevent premature births nor improve adverse fetal outcomes such as respiratory distress syndrome." - Goodman & Gilman's Pharmacological Basis of Therapeutics
"The goal of delaying delivery is to enable administration of antenatal corticosteroids for lung maturation and magnesium sulfate for neuroprotection, as well as to permit maternal transport to a tertiary facility." - Roberts & Hedges' Clinical Procedures in Emergency Medicine
Principle 5: Administer Antenatal Corticosteroids (the single most important intervention)
Corticosteroids accelerate fetal organ maturation and are the cornerstone of preterm labour management. Maximum benefit appears within 24 hours and effects last approximately 7 days.
Regimen:
- Betamethasone 12 mg IM every 24 hours x 2 doses, OR
- Dexamethasone 6 mg IM every 12 hours x 4 doses
Indications: 24-34 weeks with risk of preterm delivery within 7 days
- Consider also at 34-36+6 weeks (late preterm) if not previously given
- A single rescue course may be given if >2 weeks have passed since original course and gestation is still <34 weeks
Benefits established by evidence:
- Reduced RDS (hyaline membrane disease)
- Reduced intraventricular haemorrhage (IVH)
- Reduced necrotising enterocolitis (NEC)
- Reduced periventricular leukomalacia
- Reduced neonatal death
- Maximum benefit seen for births between 22-25 weeks
"Corticosteroids not only increase surfactant secretion in the fetal lung but also induce morphologic development of pulmonary epithelial cells and increase lung compliance... decreasing the incidence of NEC, IVH, periventricular leukomalacia, and death." - Mulholland & Greenfield's Surgery 7e
Principle 6: Choose Tocolytic Agent Thoughtfully
No single tocolytic is FDA-approved for this indication. Selection should be guided by gestational age, clinical circumstances, and maternal comorbidities.
First-line: Nifedipine (Calcium Channel Blocker) - WHO preferred
- Mechanism: blocks calcium entry into myometrial smooth muscle cells, reducing actin-myosin interaction
- Dosing: 10-20 mg oral loading dose, repeated every 3-6 hours until contractions settle, then 30-60 mg long-acting every 12-24 hours for 48 hours
- Advantages: oral, convenient, fewer maternal side effects than β-mimetics
- Cochrane evidence: effective in delaying delivery >48 hours; better neonatal outcomes and fewer maternal side effects vs β-mimetics
- Caution: avoid in hypotension, cardiac disease; do NOT combine with MgSO4 (risk of skeletal muscle blockade) or β-mimetics (cardiovascular interaction)
- Avoid doses >60 mg total in acute phase; do not chew short-acting tablets
Second-line options:
| Agent | Mechanism | Key Use / Notes |
|---|---|---|
| Indomethacin (COX inhibitor) | Reduces prostaglandin synthesis → decreases intracellular Ca²+ and myosin kinase activation | Use <32 weeks only. Loading 50-100 mg PO/PR, then 25-50 mg q6h x max 48 hours. Risk: ductal constriction (usually reversible), oligohydramnios |
| Magnesium sulphate | Ca²+ antagonism at myometrial level | IV: 4-6 g bolus over 20 min, then 1-3 g/h. Cochrane evidence shows it is ineffective as tocolytic; given in PTL mainly for neuroprotection <32 weeks |
| Terbutaline (β2-agonist) | Stimulates β2-adrenergic receptors → increases cAMP → reduces myosin kinase activity | 0.25 mg SC q20-60 min. High side-effect burden (tachycardia, arrhythmias, pulmonary oedema, hyperglycaemia, hypokalaemia). FDA warned against oral/SQ maintenance use. |
| Atosiban (oxytocin receptor antagonist) | Competitive inhibitor of oxytocin/vasopressin receptors | IV bolus + infusion. Minimal maternal side effects; widely used in Europe, not FDA-approved in USA |
Key prescribing rules:
- Do NOT combine nifedipine + MgSO4 (neuromuscular blockade)
- Do NOT combine nifedipine + IV β-mimetics (cardiovascular)
- Do not initiate tocolysis for unconfirmed labour
- Cochrane evidence favours nifedipine > β-mimetics > MgSO4 for tocolytic efficacy
Principle 7: Magnesium Sulphate for Fetal Neuroprotection (<32 weeks)
Separate from its role as a tocolytic (where evidence is weak), MgSO4 significantly reduces the risk of cerebral palsy in surviving preterm infants when given before delivery <32 weeks.
- Typical regimen: 4-6 g IV bolus + 1-2 g/h infusion until delivery
- Monitor for toxicity: respiratory depression (patellar reflexes lost at ~7-10 mEq/L, respiratory arrest at >12 mEq/L)
- Antidote: calcium gluconate 1 g IV
Principle 8: GBS Prophylaxis
Administer intrapartum antibiotic prophylaxis for Group B Streptococcus (GBS) if preterm delivery appears likely and GBS status is unknown or positive.
- First-line: Penicillin G 5 million units IV, then 2.5-3 million units q4h until delivery
- Penicillin allergy (low risk): Ampicillin 2 g IV, then 1 g q4h
- Penicillin allergy (high risk / anaphylaxis): Clindamycin or vancomycin (based on sensitivities)
Principle 9: Do NOT Use Maintenance Tocolysis
Once the initial 48-hour window has passed (corticosteroids given, transfer complete), maintenance tocolysis does not work and is not recommended.
- Cochrane reviews of oral β-mimetics, terbutaline pump, oxytocin antagonists, and calcium channel blockers all found no evidence of reduced preterm birth rate with maintenance therapy
- One study found infants exposed to maintenance calcium channel blockers had significantly longer NICU stays (mean 14 extra days)
- Outpatient uterine contraction monitoring and associated care did not improve delivery rates or birth weight
"Continued suppression of contractions after acute tocolysis (maintenance tocolysis) does not reduce the rate of preterm birth." - Creasy & Resnik's Maternal-Fetal Medicine
Principle 10: Plan for Delivery and Neonatal Care
If tocolysis fails or is not indicated, prepare for preterm delivery:
- Mode of delivery: Aim for slow, controlled vaginal delivery with minimal maternal expulsive effort; episiotomy and low forceps may be used for head protection
- Breech at <34 weeks: Caesarean section is generally preferred - soft cranium and cord prolapse risk
- Fetal indications for CS: Fetal distress, IUGR, failure to progress, malpresentation
- Analgesia: Epidural/spinal preferred - promotes pelvic relaxation and allows slow delivery
- Neonatal team: Alert NICU/paediatrics team for resuscitation; very preterm infants (<30 weeks) need immediate respiratory support
- Avoid: Prolonged cord compression; manage PROM with vigilance for ascending infection
Summary Framework
Suspected preterm labour
↓
Confirm diagnosis (cervical change + contractions)
↓
Exclude PROM, infection, contraindications to tocolysis
↓
Basic measures: O₂, hydration, left lateral position, treat UTI
↓
Give CORTICOSTEROIDS (betamethasone 12 mg IM x 2 doses over 24h)
↓
Give GBS prophylaxis if delivery likely
↓
Tocolysis (48-hour window only):
First-line → Nifedipine
<32 weeks → Add MgSO₄ for neuroprotection
<32 weeks → Consider indomethacin
↓
Arrange maternal transfer to tertiary centre if <34 weeks
↓
No maintenance tocolysis after 48 hours
↓
Plan delivery: mode, analgesia, NICU team
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Goodman & Gilman's Pharmacological Basis of Therapeutics; Morgan & Mikhail's Clinical Anesthesiology 7e; Textbook of Family Medicine 9e; Mulholland & Greenfield's Surgery 7e

photo-1783936885729.jpg
Write a complete case sheet and discusssion on this
analyse_media
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
CASE SHEET
PATIENT IDENTIFICATION
| Name | Mrs. R |
| Age | 32 years |
| Gravida / Para | Primigravida (G1 P0 L0 A0) |
| Residence | Bheemili |
| Education | 10th Standard |
| Occupation | Homemaker |
| Socioeconomic Status | Middle class |
| Religion | Not mentioned |
| Date of Admission | (Date of presentation) |
| IP Number | |
| Ward | Obstetrics |
OBSTETRIC DETAILS
| Last Menstrual Period (LMP) | 22 July 2024 |
| Expected Date of Delivery (EDD) | 29 April 2025 |
| Period of Gestation at Presentation | ~32 weeks (8 months) |
| Period of Amenorrhoea | ~8 months |
Gestational age calculation:
LMP 22 July 2024 → by Naegele's rule (add 9 months + 7 days) → EDD 29 April 2025.
At presentation (~early March 2025) = approximately 32 weeks 0 days of gestation.
This places the pregnancy firmly in the preterm period (20-36+6 weeks).
CHIEF COMPLAINT
- Lower abdominal pain since 6 hours (on the day of admission)
HISTORY OF PRESENTING ILLNESS
Mrs. R, a 32-year-old primigravida at approximately 32 weeks of gestation, presented to the Obstetrics OPD/Emergency with complaints of lower abdominal pain since 6 hours. The pain was:
- Onset: Sudden / gradual (to be elicited)
- Character: Intermittent, cramping in nature (suggestive of uterine contractions)
- Duration of each episode: Approximately 20-45 seconds per contraction (to be confirmed by CTG)
- Frequency: To be assessed on CTG monitoring
- Radiation: To the back (to be elicited)
- Associated symptoms:
- Watery vaginal discharge / leaking per vaginum - to be asked (to rule out PROM)
- Bleeding per vaginum - to be asked (to rule out placenta praevia / abruption)
- Decreased fetal movements - to be asked
- Fever / chills - to be asked (to rule out chorioamnionitis / UTI)
- Dysuria / frequency - to be asked (to rule out UTI as a precipitant)
- Vomiting / nausea - to be asked
- Relieving / aggravating factors: To be elicited
MENSTRUAL HISTORY
| Age of menarche | To be elicited |
| Cycle | Regular / Irregular |
| Duration | To be elicited |
| Flow | Normal |
| Dysmenorrhoea | To be elicited |
| LMP | 22 July 2024 (certain / uncertain) |
PAST OBSTETRIC HISTORY
- Primigravida - no previous pregnancies, no history of prior preterm birth, miscarriage, or cervical procedure
ANTENATAL HISTORY (Current Pregnancy)
| Antenatal registration | Yes / No |
| Number of ANC visits | To be elicited |
| Place of ANC | To be elicited |
| Iron / folic acid supplementation | Yes / No |
| Calcium supplementation | Yes / No |
| Immunisation (TT/Td) | Given / Not given |
| Ultrasonography done | Yes / No (dating scan, anomaly scan) |
| Gestational diabetes screening | Done / Not done |
| Anomaly scan findings | Normal / Abnormal |
| History of UTI / treated infection | To be elicited |
| History of trauma / heavy lifting | To be elicited |
| History of intercourse prior to pain | To be elicited |
| Cervical cerclage | None |
PAST MEDICAL HISTORY
- Hypertension: No (to be confirmed)
- Diabetes mellitus: No (to be confirmed)
- Cardiac disease: No
- Thyroid disorder: No
- Asthma: No
- Tuberculosis: No
- Surgeries: None
- Blood transfusions: None
- Allergies: None known
FAMILY HISTORY
- No known history of multiple gestations, inherited disorders, or preterm births in family
PERSONAL HISTORY
- Diet: Mixed / Vegetarian
- Sleep: Adequate
- Bowel/Bladder: Regular
- Tobacco / Alcohol / Substance use: Nil (to be confirmed)
- Stress / Physical exertion: To be elicited
GENERAL PHYSICAL EXAMINATION
| Parameter | Finding |
|---|---|
| General appearance | Conscious, oriented, cooperative, in mild distress |
| Built and nourishment | Moderately built and nourished |
| Height | |
| Weight | |
| BMI | |
| Pallor | Present / Absent |
| Icterus | Absent |
| Cyanosis | Absent |
| Clubbing | Absent |
| Oedema | Present / Absent (pedal) |
| Lymphadenopathy | Absent |
| Pulse rate | bpm |
| Blood pressure | mmHg |
| Respiratory rate | /min |
| Temperature | °F |
| SpO2 | % on room air |
SYSTEMIC EXAMINATION
Cardiovascular System
- S1 S2 heard, no murmurs
Respiratory System
- Bilateral air entry equal, no added sounds
Central Nervous System
- Conscious, oriented, no focal deficits
OBSTETRIC EXAMINATION
Abdominal Examination
Inspection:
- Abdomen distended corresponding to approximately 32 weeks of gestation
- Linea nigra present
- Striae gravidarum present
- Umbilicus - everted / flat
- Fetal movements visible / not visible
Palpation:
| Fundal height | 32 weeks / cm from pubic symphysis |
| Uterine contractions | Present - frequency, duration, intensity to be documented |
| Uterine tenderness | Absent (if present - suspect chorioamnionitis / abruption) |
| Lie | Longitudinal |
| Presentation | Cephalic / Breech |
| Engagement | Not engaged (expected at 32 weeks) |
| Liquor | Adequate (to be assessed) |
Auscultation:
- Fetal Heart Rate (FHR): bpm (normal 110-160 bpm)
Sterile Speculum Examination
(Done first if leaking suspected, before digital examination)
- Liquor pooling: Present / Absent
- Nitrazine test: Positive (turns blue) / Negative
- Ferning: Positive / Negative
- Cervical os: Open / Closed
- Bleeding: Present / Absent
- Discharge: Character, colour, odour
Digital Vaginal Examination
(Done only after excluding PROM and after fFN swab collection)
| Cervical position | Posterior / Mid / Anterior |
| Cervical consistency | Soft / Firm |
| Cervical effacement | % |
| Cervical dilatation | cm |
| Membranes | Intact / Bulging / Absent |
| Station of presenting part | |
| Bishop Score | /13 |
INVESTIGATIONS
Mandatory
| Investigation | Value | Normal |
|---|---|---|
| Haemoglobin | g/dL | >11 g/dL |
| Total leucocyte count (TLC) | cells/mm³ | 4000-11000 (elevated in infection) |
| Differential count | Neutrophilia in infection | |
| Platelets | >1.5 lakh | |
| Blood group and Rh type | ||
| Blood glucose (random/fasting) | mg/dL | |
| Urine routine and microscopy | No pus cells | |
| Urine culture and sensitivity | Sterile | |
| CRP | mg/L | Elevated in chorioamnionitis |
Obstetric Investigations
| Investigation | Purpose |
|---|---|
| Cardiotocography (CTG) | Confirm contractions, assess FHR pattern |
| Fetal fibronectin (fFN) swab | Negative = PTB unlikely in 7-10 days; positive = at risk |
| Transvaginal ultrasound (TVU) - cervical length | <25 mm = high risk for PTB |
| Obstetric ultrasound | Fetal biometry, presentation, AFI, placental site, Doppler |
| High vaginal swab (HVS) | Culture for GBS, Chlamydia, GC |
If Chorioamnionitis Suspected
- Blood culture
- Amniocentesis (in selected cases) - WBC, glucose, culture
DIAGNOSIS
Working Diagnosis:
G1P0L0A0 with preterm labour at 32 weeks of gestation
Supporting evidence:
- Primigravida with 32 weeks of gestation (LMP 22 July 2024, EDD 29 April 2025)
- Lower abdominal pain since 6 hours - suggestive of uterine contractions
- Gestational age <37 weeks = preterm
Diagnosis confirmed by:
- Uterine contractions on CTG (≥4/hour)
- Cervical change: ≥2 cm dilatation OR ≥80% effacement OR documented progression
MANAGEMENT
Immediate (Emergency measures)
- Admit to labour ward / antenatal ward
- IV access - 18G cannula
- Continuous CTG monitoring - confirm contractions and FHR
- Left lateral position - improves uteroplacental perfusion
- IV crystalloid - Ringer's lactate 500 mL over 30 minutes (treat dehydration)
- Supplemental oxygen - if SpO2 <95%
- NPO in case delivery is imminent
Step 1 - Rule out contraindications to tocolysis
Check for:
- Chorioamnionitis (fever + uterine tenderness + leukocytosis)
- PROM (sterile speculum exam)
- Abruption (bleeding + uterine rigidity)
- Fetal compromise (CTG - non-reassuring pattern)
- Placenta praevia
Step 2 - Antenatal Corticosteroids (most important)
Betamethasone 12 mg IM - first dose immediately; second dose after 24 hours
- Indication: 32 weeks gestation, risk of preterm delivery
- Accelerates fetal lung maturity - reduces RDS, IVH, NEC, death
- Maximum benefit after 24 hours - tocolysis aims to buy this window
Step 3 - GBS Prophylaxis
Injection Penicillin G 5 million units IV stat, then 2.5 million units IV every 4 hours until delivery
- If penicillin allergy: Ampicillin IV
- Reduces neonatal early-onset GBS sepsis
Step 4 - Tocolysis (to allow 48 hours for corticosteroids)
First-line: Nifedipine (Calcium Channel Blocker) - WHO preferred
- Tab. Nifedipine 10-20 mg oral loading dose
- Repeat 10-20 mg every 3-6 hours until contractions settle
- Then Tab. Nifedipine SR 30-60 mg every 12-24 hours for 48 hours
- Monitor: BP (hypotension), FHR
If nifedipine contraindicated (hypotension, cardiac disease):
Alternative: Indomethacin (at 32 weeks - still within safe window)
- 50-100 mg loading dose oral/rectal
- 25-50 mg every 6 hours for maximum 48 hours
- Monitor: liquor volume (oligohydramnios), ductus arteriosus (fetal echo after 48 hours)
- Do not use beyond 32 weeks due to ductal constriction risk
Step 5 - Magnesium Sulphate for Neuroprotection
Inj. MgSO4 4-6 g IV bolus over 20-30 min, then 1-2 g/hour IV infusion until delivery or 24 hours
- Indication: <34 weeks - reduces risk of cerebral palsy in surviving preterm infant
- Monitor: respiratory rate, patellar reflexes (absent = toxicity), urine output
- Antidote: Calcium gluconate 1 g IV
Step 6 - Monitoring
| Parameter | Frequency |
|---|---|
| CTG | Continuous |
| BP | Every 30 minutes |
| Urine output | Hourly |
| Temperature | Every 4 hours |
| FHR | Continuous |
| TLC / CRP | Repeat at 24 hours |
| Patellar reflex (if on MgSO4) | Every hour |
| Cervical examination | Every 4-6 hours |
Step 7 - Supportive
- Bed rest (left lateral)
- Hydration
- Treat UTI if present (empirical: oral nitrofurantoin / cephalexin - pending culture)
- Anaemia correction if Hb <10 g/dL: oral/IV iron
- Psychological support and counselling to patient and family
Step 8 - If Tocolysis Fails / Delivery Proceeds
- Alert Neonatology / NICU team for preterm baby of ~32 weeks
- Mode of delivery: Vaginal if vertex presentation; CS if breech, fetal distress, failure to progress
- Slow, controlled delivery with epidural analgesia
- Episiotomy and low forceps may be used to protect soft preterm head
- Do not give maternal maintenance tocolysis after 48 hours
PROGNOSIS
- Fetal prognosis at 32 weeks with timely corticosteroids and NICU support: generally good; survival rate >95%
- Neonatal risks: RDS, IVH, NEC, hypothermia, hypoglycaemia, feeding difficulties
- Maternal prognosis: Good if no sepsis or underlying disease
DISCUSSION
Overview
This case involves a 32-year-old primigravida presenting at approximately 32 weeks of gestation (preterm period) with lower abdominal pain for 6 hours - the classic presentation of preterm labour. Several features make this case clinically instructive.
Why 32 Weeks is a Critical Gestational Age
At 32 weeks, the fetus has passed the threshold of viability (24 weeks) but is not yet mature. Specific concerns at this gestation:
- Pulmonary: Surfactant production begins around 20 weeks but is inadequate before 34-35 weeks; RDS is a major cause of neonatal death
- Neurological: High risk of IVH and periventricular leukomalacia leading to cerebral palsy
- Gastrointestinal: NEC risk is significant
- Thermoregulation: Poor subcutaneous fat → hypothermia
This makes every hour of additional intrauterine time valuable - and explains why the focus of management is NOT to prevent delivery indefinitely, but to gain 48 hours for corticosteroids to work.
Significance of Primigravida Status
- Primigravidae have no prior obstetric history to suggest risk; this makes it critical to identify precipitating causes
- A prior preterm birth is the strongest single risk factor for recurrence (RR 2-5x); here it is absent, so other causes must be sought: UTI, BV, physical exertion, dehydration
- Cervical incompetence is less common in primigravidae but cannot be entirely excluded
- Advanced maternal age (32 years) combined with primigravida status is itself a mild risk factor
Calculating Gestational Age - Clinical Importance
- LMP: 22 July 2024
- EDD (Naegele's rule): Add 1 year, subtract 3 months, add 7 days → 29 April 2025 (confirmed by the slide)
- At presentation with "8 months pregnancy": ~32 weeks
- This lies in the period where all four major interventions (tocolysis, betamethasone, GBS prophylaxis, MgSO4 neuroprotection) are indicated
Accurate gestational age is critical: corticosteroids are indicated at 24-34 weeks; indomethacin is safe only <32 weeks; MgSO4 neuroprotection is given <34 weeks.
Pathophysiology of Preterm Labour
Normal labour results from a shift from uterine quiescence to active contractions, mediated by:
- Rise in prostaglandins (PGE2, PGF2α) - stimulate myometrial contractions
- Oxytocin receptor upregulation
- Cervical ripening (collagen breakdown, prostaglandin-mediated)
- Gap junction formation between myometrial cells (electrical coupling)
In preterm labour, this process is triggered prematurely by:
| Pathway | Example triggers |
|---|---|
| Infection / inflammation | Chorioamnionitis, UTI, BV → cytokines → prostaglandin release |
| Uterine overdistension | Multiple gestation, polyhydramnios |
| Decidual haemorrhage | Abruption, placenta praevia |
| Cervical insufficiency | Prior trauma, congenital |
| Stress / hypothalamic-adrenal axis activation | Psychosocial stress, physical labour |
| Idiopathic | ~50% of cases |
The final common pathway is myosin light-chain kinase (MLCK) activation through rising intracellular calcium - the target of tocolytic agents.
Why Each Management Step is Justified in This Case
1. Confirm the diagnosis
At 32 weeks with 6 hours of pain, true preterm labour must be distinguished from Braxton-Hicks contractions. Digital examination after collecting fFN is the cornerstone. A negative fFN has 99% NPV for delivery in 7-10 days and can avoid unnecessary intervention. TVU cervical length <25 mm strongly supports preterm labour.
2. Antenatal corticosteroids
This is the single most important intervention in preterm labour management. Betamethasone at 32 weeks:
- Stimulates surfactant production by type II pneumocytes
- Induces morphological maturation of pulmonary epithelial cells
- Reduces RDS by 50%, IVH by 40%, NEC by 50%
- Maximum effect appears within 24 hours and lasts 7 days
- Both doses should be completed before delivery if at all possible - hence tocolysis is used to buy this window
3. Tocolysis with nifedipine
Nifedipine (calcium channel blocker) is the WHO-preferred first-line tocolytic:
- Oral route - convenient and safe
- Cochrane reviews confirm it delays delivery >48 hours and improves neonatal outcomes compared to β-mimetics
- At 32 weeks, indomethacin could also be considered (within the <32-week cut-off), but nifedipine is safer beyond 30 weeks
- Tocolysis does NOT prevent preterm birth - it only buys time (48-72 hours in ~75-80% of patients)
- Maintenance tocolysis after 48 hours provides NO benefit and may increase NICU stay - it should not be continued
4. GBS prophylaxis
Group B Streptococcus is the leading cause of early-onset neonatal sepsis. If GBS status is unknown and preterm delivery is anticipated, empirical prophylaxis is given. At 32 weeks, even a brief neonatal bacteraemia carries significantly higher morbidity than at term.
5. Magnesium sulphate for neuroprotection
At 32 weeks, the fetal brain is highly vulnerable to white matter injury (periventricular leukomalacia). MgSO4:
- Stabilises neuronal membranes
- Reduces glutamate excitotoxicity
- Multiple RCTs confirm reduced risk of cerebral palsy when given <34 weeks before preterm delivery
- This is given in addition to (not instead of) tocolysis, and is a separate indication
Special Considerations for This Patient
Primigravida + Advanced age (32 years)
- No prior obstetric history to guide risk stratification
- Baseline pre-delivery workup especially important: USS biometry, Doppler, AFI
- Psychological impact of a preterm birth in a primigravida - may be profound; counselling needed
Residing in Bheemili (semi-rural area)
- Access to tertiary NICU care may be limited locally
- Maternal transport to a tertiary facility with NICU should be arranged if tocolysis is successful and delivery is not imminent
- A 32-weeker requires Level III NICU support (ventilation, TPN, monitoring)
Middle socioeconomic class
- Compliance with follow-up and medications is likely reasonable
- Financial counselling regarding NICU costs should be initiated early
No known risk factors
- In the absence of infection, abruption, or PROM: this may represent idiopathic preterm labour, which comprises ~50% of cases
- Investigate for occult UTI, BV, or subclinical chorioamnionitis
Differential Diagnoses
| Condition | Differentiating Features |
|---|---|
| True preterm labour | Regular contractions + cervical change; CTG confirms contractions |
| Braxton-Hicks contractions | Irregular, no cervical change; negative fFN |
| Preterm PROM | Leaking per vaginum, positive nitrazine/ferning; no prolonged contractions initially |
| Abruptio placentae | Painful bleeding, rigid uterus, non-reassuring FHR |
| Placenta praevia | Painless fresh PV bleeding (but can coexist with contractions) |
| UTI / pyelonephritis | Dysuria, fever, CVA tenderness; uterine contractions as secondary finding |
| Chorioamnionitis | Fever + uterine tenderness + leukocytosis + maternal/fetal tachycardia |
| Round ligament pain | Sharp, non-cramping, no contractions, no cervical change |
| Appendicitis | Right-sided, maximal at McBurney's point, associated with nausea/vomiting |
Complications if Untreated / If Delivery Occurs at 32 Weeks
Neonatal
- Respiratory Distress Syndrome (RDS) - surfactant deficiency; requires CPAP/ventilation
- Intraventricular Haemorrhage (IVH) - immature germinal matrix; risk of hydrocephalus, cerebral palsy
- Necrotising Enterocolitis (NEC) - immature gut; surgical emergency
- Hypothermia - poor thermoregulation
- Hypoglycaemia - limited glycogen stores
- Retinopathy of Prematurity (ROP) - especially if oxygen therapy needed
- Neonatal sepsis - immature immune system
- Prolonged NICU stay - feeding difficulties, apnoeas
Maternal
- Chorioamnionitis if labour prolonged
- PPH (particularly if prolonged tocolytic use)
- Psychological trauma / postnatal depression in a primigravida experiencing preterm birth
Outcome and Follow-up
If successfully arrested:
- Discharge after 48-72 hours if contractions settled and cervix stable
- Outpatient follow-up at 1 week
- Serial TVU cervical length monitoring
- Avoid strenuous activity, coitus (debated)
- Oral tocolytics: NOT recommended as maintenance
- Repeat corticosteroids: single rescue course if >2 weeks from first course and <34 weeks
- Plan delivery at a tertiary centre
If delivery proceeds at 32 weeks:
- NICU team to be present at delivery
- Neonatal resuscitation readiness
- Delayed cord clamping (60 seconds) - improves neonatal Hb and reduces IVH
- Kangaroo mother care and breastfeeding support
Key Takeaways from This Case
- Gestational age at 32 weeks means all four major interventions apply: corticosteroids, tocolysis (48h only), GBS prophylaxis, and MgSO4 neuroprotection
- Tocolysis is a bridge - its only goal is 48 hours for steroids and/or maternal transfer; it does not prevent preterm birth
- Corticosteroids are the single most important intervention - they should never be omitted
- Confirm the diagnosis first - overtreatment of Braxton-Hicks contractions is common; fFN and TVU cervical length are the most useful diagnostic tools
- Primigravida at 32 weeks with no identifiable risk factor = likely idiopathic; investigate thoroughly for treatable causes (UTI, BV, dehydration)
- Arrange NICU transport early if tertiary facilities are not locally available
Sources: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice; Textbook of Family Medicine 9e; Goodman & Gilman's Pharmacological Basis of Therapeutics; Morgan & Mikhail's Clinical Anesthesiology 7e; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Mulholland & Greenfield's Surgery 7e
This is a shared conversation. Sign in to Orris to start your own chat.