Common Radiological l lesions of brain mri
Reading File
Finding Sources
Finding Sources
Searching the Web
common radiological lesions brain MRI radiology 2024
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive textbook content and images. Let me compile the complete structured answer.
Common Radiological Lesions of the Brain on MRI
Based on Grainger & Allison's Diagnostic Radiology, 7th ed. and supporting neurology textbooks
Understanding MRI Signal Characteristics (Quick Reference)
Before categorising lesions, understanding basic MRI signal behaviour is essential:
| Tissue/State | T1 Signal | T2/FLAIR Signal | DWI |
|---|---|---|---|
| CSF | Dark (hypointense) | Bright; suppressed on FLAIR | Dark (free diffusion) |
| Normal white matter | Intermediate | Dark relative to grey matter | - |
| Oedema / gliosis | Dark | Bright | Variable |
| Acute infarction | Dark | Bright | Bright (restricted) |
| Subacute haemorrhage | Bright (metHb) | Bright | - |
| Chronic haemorrhage | Dark rim (haemosiderin) | Dark rim | - |
| Pus/viscous fluid | Intermediate | Intermediate-bright | Bright (restricted) |
| Fat | Bright | Bright | - |
| Calcification | Dark | Dark | - |
1. Vascular Lesions
1a. Acute Ischaemic Stroke / Infarction
- DWI is the key sequence: shows bright signal within minutes of onset (restricted diffusion)
- Corresponding ADC map shows dark (low) signal - confirming true restriction, not T2 shine-through
- T2/FLAIR: hyperintense, but may lag DWI by 6-12 hours
- T1: hypointense territory
- Cortical gyral enhancement may appear after 1-2 weeks
- Distribution follows a vascular territory (e.g., MCA, ACA)
- Cytotoxic oedema: no ADC elevation on DWI = distinguishes from vasogenic oedema
1b. Intracranial Haemorrhage
MRI signal evolves predictably with time:
| Stage | Timing | T1 | T2 |
|---|---|---|---|
| Hyperacute | <24 h | Iso/hypointense | Hyperintense |
| Acute | 1-3 days | Iso/hypointense | Hypointense (deoxy-Hb) |
| Early subacute | 3-7 days | Hyperintense (met-Hb, intracellular) | Hypointense |
| Late subacute | 1-2 wk | Hyperintense | Hyperintense |
| Chronic | Months | Hypointense rim | Dark rim (haemosiderin) |
- Susceptibility-Weighted Imaging (SWI) is most sensitive for microbleeds, cavernomas and haemorrhagic transformation
- Germinal matrix haemorrhage (neonates): begins under frontal horn ependyma; progresses to intraventricular haemorrhage (IVH) and porencephalic cyst
1c. Subdural Haematoma
- Crescentic collection over the brain surface
- Acute: hyperdense on CT; T1 iso-/hypointense, T2 hypointense
- Subacute: bright on T1 (methaemoglobin)
- Chronic: T1/T2 hyperintense (lysed blood products)
1d. Cerebral Venous Sinus Thrombosis
- Non-arterial territory infarction, often with haemorrhage
- MRV (MR venography) shows filling defect in the affected sinus
- T1 shows hyperintense thrombus in the sinus
2. Infective / Inflammatory Lesions
2a. Brain Abscess
This is one of the most important lesions to recognise on MRI:
- Central cavity: T1 intermediate (between CSF and white matter); T2 iso- to mildly hyperintense
- Abscess rim: T2 hypointense (relatively - caused by free radicals from phagocytosis)
- SWI: rim appears markedly hypointense; a "dual rim" sign (outer hypointense + inner hyperintense) is characteristic
- DWI: central cavity is bright (restricted diffusion) with low ADC - this is the key distinguishing feature from necrotic tumour
- Post-contrast: smooth, thin ring enhancement; the inner margin is smooth; medial wall is thinner than the lateral wall
- Surrounding vasogenic oedema: T1 low, T2/FLAIR high
- Satellite microabscesses are common (10-50% are multiple)
Key distinction: Tumour (GBM, metastasis) tends to have thick, irregular enhancement and does NOT show central restricted diffusion reliably. Dynamic perfusion MRI shows lower rCBV in abscess rim vs. glioma rim.
2b. Meningitis
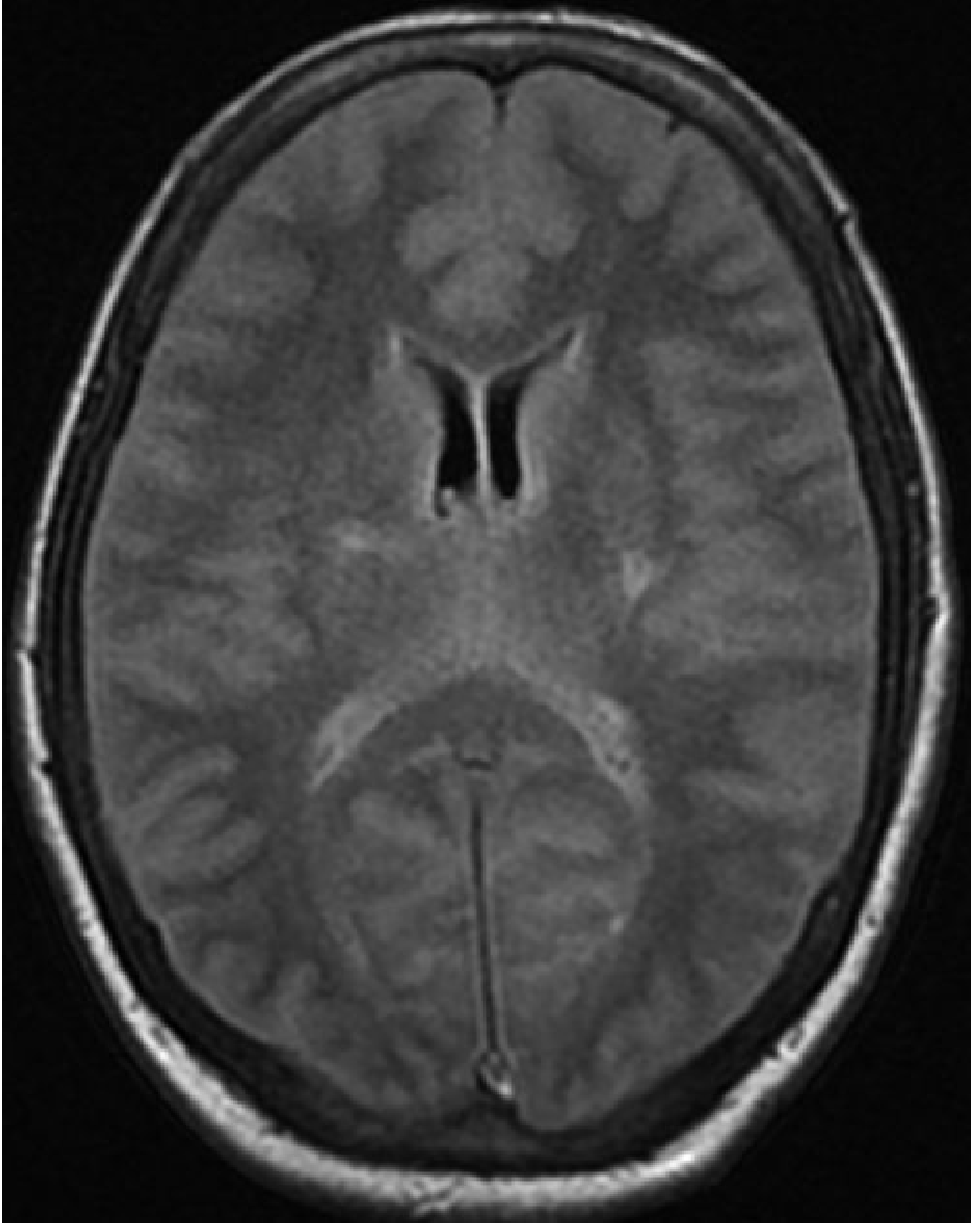
- FLAIR may show failure of CSF suppression (pus in sulci appears hyperintense, as in image above)
- Post-contrast T1: leptomeningeal enhancement (following sulci and gyri)
- May cause complications: cerebral oedema, ventriculitis, empyema, venous thrombosis
2c. Subdural Empyema
- Crescentic collection identical in location to subdural haematoma
- T2/FLAIR: hyperintense; DWI restricted (pus)
- Post-contrast: thick dural enhancement at the deep margin
- Does NOT cross midline (unlike epidural abscess, which can cross)
2d. Epidural Abscess
- Lentiform (biconvex) extradural collection between dura and inner skull table
- T2/FLAIR: hyperintense; DWI: restricted
- Thick, slightly irregular dural enhancement at deep margin
- CAN cross midline (dura not attached at midline anteriorly)
- Common cause: frontal sinusitis, otomastoiditis
2e. Ventriculitis
- Ependymal enhancement around ventricles on post-contrast T1
- T2/FLAIR: periventricular hyperintensity
- DWI: may show restricted diffusion within ventricles (intraventricular pus)
3. Neoplastic Lesions
3a. Classification Framework
Brain tumours are first classified as:
- Intra-axial (within brain parenchyma): gliomas, metastases, lymphoma
- Extra-axial (outside parenchyma, from meninges/nerves/skull): meningioma, schwannoma, epidermoid
Clue: The "claw sign" - cerebral parenchyma surrounding an intra-axial tumour like a claw confirms its parenchymal origin.
3b. Glioblastoma Multiforme (GBM) - WHO Grade IV
- Most common malignant primary brain tumour in adults (mean age 59 years)
- MRI hallmarks:
- Heterogeneous intra-axial mass
- Central necrosis: T1 dark, T2 bright
- Thick, irregular ring enhancement post-gadolinium
- Surrounding T2/FLAIR hyperintensity (vasogenic oedema + infiltrative tumour)
- "Butterfly" appearance when crossing the corpus callosum
- Perfusion MRI: elevated rCBV (hyperperfused)
- MR spectroscopy: elevated choline, reduced NAA, elevated lipids/lactate
3c. Low-Grade Glioma (Astrocytoma/Oligodendroglioma - WHO Grade II)
- Diffuse infiltrating, non-enhancing (typically)
- T2/FLAIR hyperintense white matter expansion with preserved architecture
- Low-grade fibrillary astrocytomas: no enhancement (key feature)
- Pilocytic astrocytoma (WHO Grade I, paediatric): cyst with an enhancing mural nodule, especially in cerebellum
3d. Metastases
- Multiple ring-enhancing lesions at grey-white junction (most common location)
- Often disproportionately large surrounding oedema relative to tumour size
- Central necrosis common in large lesions
- May show restricted diffusion (overlap with abscess)
- Perfusion: elevated rCBV (but lower than GBM)
- Common primaries: lung, breast, melanoma, renal cell, colorectal
3e. Meningioma (Extra-axial)
- Arises from dura; extra-axial location
- T1: isointense to grey matter; T2: variable (may be hypointense)
- Post-contrast: intense, homogeneous enhancement
- Dural tail sign: linear enhancement extending from tumour along dura
- May show calcification (hypointense on all sequences)
- Buckling and displacement of adjacent cortex (not invasion of parenchyma)
3f. Lymphoma (Primary CNS)
- Typically periventricular, corpus callosum, basal ganglia
- T1: isointense; T2: isointense to mildly hyperintense (relatively hypercellular)
- Homogeneous enhancement in immunocompetent patients
- DWI: restricted (highly cellular)
- Perfusion: low rCBV despite enhancement (unlike GBM)
- Dramatically sensitive to corticosteroids ("ghost tumour" - may vanish on MRI after steroids)
3g. Posterior Fossa Tumours (Paediatric)
The most common in children, in order of frequency:
- Medulloblastoma - midline, arises from 4th ventricle roof; DWI restricted; homogeneous enhancement; leptomeningeal spread common
- Pilocytic astrocytoma - cystic with mural nodule; intense enhancement of nodule; favourable prognosis
- Ependymoma - arises from floor of 4th ventricle; "plastic" extension through foramina (Luschka/Magendie); calcification common
- Atypical Teratoid Rhabdoid Tumour (ATRT) - very young children; heterogeneous, aggressive
4. Demyelinating / White Matter Lesions
4a. Multiple Sclerosis (MS)
- Ovoid periventricular lesions oriented perpendicular to ventricles ("Dawson's fingers" on sagittal FLAIR)
- Lesion locations required for diagnosis (2024 McDonald criteria): periventricular, cortical/juxtacortical, infratentorial, spinal cord
- T2/FLAIR: hyperintense
- Active lesions: ring or nodular enhancement on post-gadolinium T1
- Central vein sign: a thin central vein within a lesion (SWI/T2*) - supports MS diagnosis
- Paramagnetic rim lesions (PRL): persistently hypointense rim on SWI/T2* - chronic active inflammation
- Black holes: T1-hypointense lesions = irreversible axonal loss
4b. Posterior Reversible Encephalopathy Syndrome (PRES)
- T2/FLAIR hyperintensity predominantly in parieto-occipital regions
- Vasogenic oedema (ADC elevated - distinguishes from infarction)
- Associated with hypertensive emergency, eclampsia, immunosuppressants
5. Traumatic Lesions
5a. Diffuse Axonal Injury (DAI)
- T2/FLAIR hyperintensities at grey-white junctions, corpus callosum, dorsolateral brainstem
- SWI most sensitive: multiple punctate microhaemorrhages (haemorrhagic DAI)
- May appear normal on CT
5b. Contusional Brain Injury
- Cortical haemorrhagic contusions: SWI/GRE hypointense foci at sites of impact and contrecoup
- Overlying subdural/extradural collections may be present
5c. Intraventricular Haemorrhage (IVH) in Premature Neonates
- Germinal matrix: hyperechogenic on US; MRI signal varies with haemorrhage age
- Late: porencephalic cyst (T2 bright communicating with lateral ventricle)
6. Epilepsy-Associated Structural Lesions
Common structural causes of epilepsy seen on MRI:
- Hippocampal sclerosis: T2 hyperintensity + volume loss in hippocampus; best on coronal FLAIR
- Focal cortical dysplasia (FCD): cortical thickening, blurring of grey-white junction on FLAIR; "transmantle" sign (linear FLAIR hyperintensity from cortex to ventricle)
- DNET (Dysembryoplastic Neuroepithelial Tumour): cortical/subcortical; T2 hyperintense; "bubbly" multilocular; no mass effect; no oedema; characteristic of temporal lobe epilepsy
- Ganglioglioma: T2 hyperintense cortical/subcortical mass; often cystic; may calcify; typically temporal; enhances variably
- Cavernous malformation: "popcorn" appearance on MRI (mixed signal core); dark hemosiderin rim on T2*/SWI; no enhancement; no surrounding oedema
7. Infective Lesions - Special Types
Neurocysticercosis
- Multiple cystic lesions; live cyst = T2 bright with scolex (white dot); dying cyst = ring enhancement + oedema; calcified = T2/SWI dark dot
- Most common cause of seizures due to parasitic CNS infection worldwide
Tuberculoma
- Solid or ring-enhancing nodule(s) with surrounding oedema
- Central T2 signal varies: T2 dark in solid caseating centre (TB-characteristic, unlike pyogenic abscess)
- Preferred locations: cerebral convexities, basal cisterns (basilar meningitis)
Toxoplasma (immunocompromised)
- Multiple ring-enhancing lesions; basal ganglia predilection
- Eccentric target sign on MRI (enhancing nodule within ring) helps distinguish from CNS lymphoma
8. Summary Table - Common MRI Lesion Patterns
| Lesion | T1 | T2/FLAIR | DWI | Enhancement |
|---|---|---|---|---|
| Acute infarction | Dark | Bright | Bright | Absent early |
| Brain abscess | Intermediate | Intermediate | Bright | Ring (thin, smooth) |
| GBM | Mixed | Bright (oedema) | Variable | Thick, irregular ring |
| Metastasis | Variable | Bright halo | Variable | Ring/nodular |
| Meningioma | Iso | Iso-bright | Variable | Intense, homogeneous + dural tail |
| MS plaque (active) | Dark | Bright | Variable | Ring/nodular |
| PRES | Iso | Bright (parieto-occipital) | Normal/high ADC | Usually absent |
| Lymphoma | Iso | Iso-bright | Bright | Homogeneous |
| Neurocysticercosis (live) | Dark | Bright (with scolex dot) | Variable | None (live) / ring (dying) |
Key MRI Sequences and Their Roles
| Sequence | Primary Use |
|---|---|
| T1 | Anatomy, haemorrhage stages, contrast enhancement |
| T2 | Oedema, demyelination, white matter disease, tumour extent |
| FLAIR | White matter lesions (suppresses CSF), meningeal disease |
| DWI/ADC | Acute stroke, abscess, lymphoma, prion disease |
| SWI/GRE T2* | Microbleeds, cavernomas, haemorrhage, DAI |
| Post-Gd T1 | Blood-brain barrier breakdown, tumour, infection |
| MR Perfusion | Tumour grading, abscess vs tumour differentiation |
| MR Spectroscopy | Metabolite ratios (Cho/NAA), tumour, demyelination |
| DTI | White matter tract integrity, pre-surgical planning |
Sources: Grainger & Allison's Diagnostic Radiology, 7th ed. | Bradley and Daroff's Neurology in Clinical Practice | Adams and Victor's Principles of Neurology, 12th ed.
Common named signs , like bathing appearance
Finding Sources
Searching the Web
named radiological signs brain MRI "bathing sign" "butterfly sign" "Dawson fingers" neuroradiology mnemonics
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC2765171
Searching the Web
neuroradiology MRI named signs "eye of tiger" "hot cross bun" "bat wing" "lollipop sign" "salt pepper" brain
Finding Sources
Reading File
Reading File
Reading Web Page
https://radiologyreviewarticles.com/neuro/neuroimaging-signs
Loading Image
Loading Image
Finding Sources
I now have rich content and beautiful textbook images. Let me compile the comprehensive answer.
Named Radiological Signs on Brain MRI
Sources: Grainger & Allison's Diagnostic Radiology | Bradley & Daroff's Neurology | PMC "Twenty Classic Signs in Neuroradiology" (IJRI 2009)
DEMYELINATING / NEURODEGENERATIVE SIGNS
1. Dawson's Fingers
- Modality: Sagittal FLAIR / T2
- Appearance: Periventricular white matter lesions oriented perpendicular to the long axis of the lateral ventricles, radiating outward like outstretched fingers
- Key anatomy: These extend along medullary veins, which run perpendicular to the ventricle walls
- Diagnosis: Multiple Sclerosis (MS) - present in ~78-93% of MS patients
- Best sequence: Sagittal FLAIR (the classic teaching image)
- Note: Can also be seen in cerebral small vessel disease; absent in NMO/NMOSD (0-5%)
2. Central Vein Sign (CVS)
- Modality: SWI or T2* (susceptibility)
- Appearance: A thin, central vein running through the middle of an MS white matter plaque
- Diagnosis: Supports MS diagnosis over other causes of white matter lesions (e.g., migraine, CSVD, vasculitis)
- Part of the 2024 McDonald MS diagnostic criteria when lesions in fewer than 4 locations are present
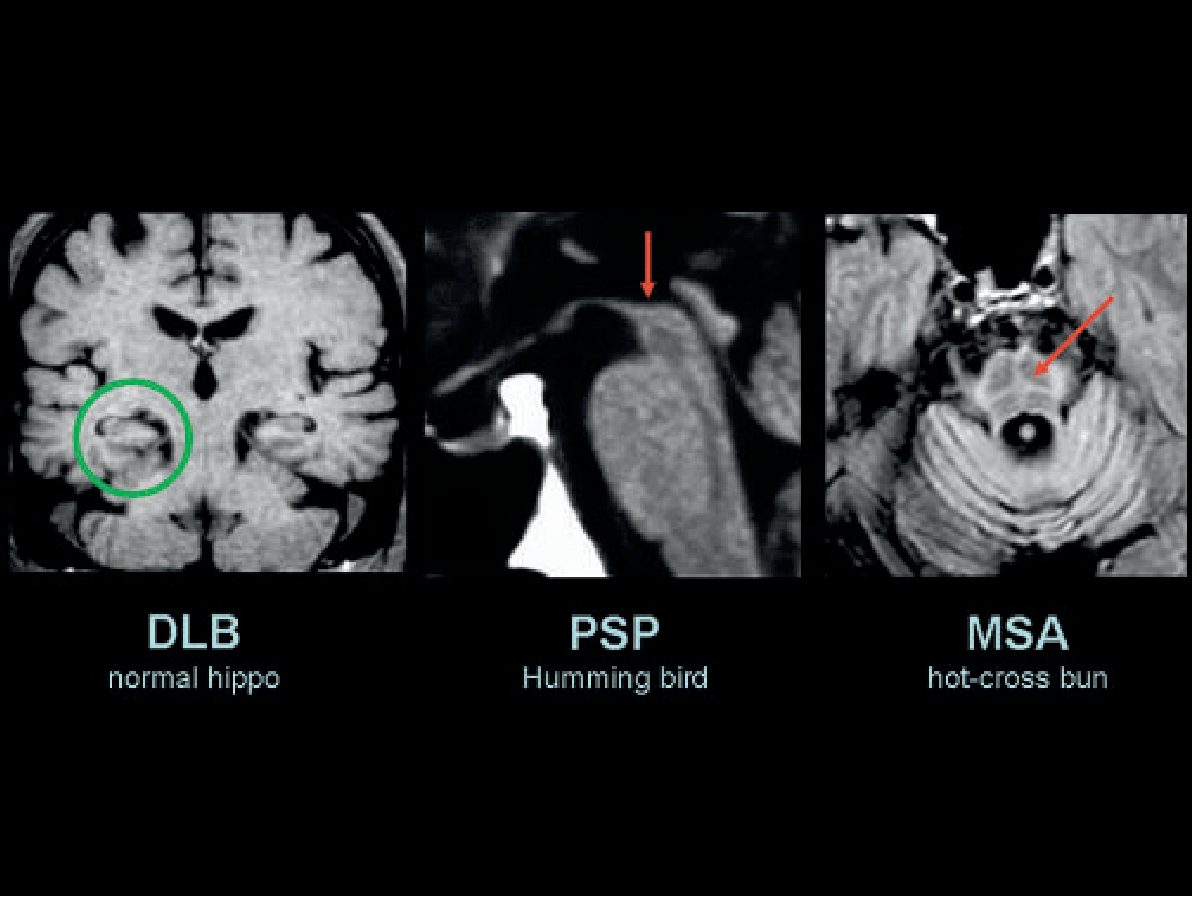
3. Hot Cross Bun Sign
- Modality: T2 / FLAIR axial through the pons
- Appearance: T2 hyperintensity forming a cross shape (horizontal + vertical lines) within the pons
- Mechanism: Selective degeneration of transverse pontocerebellar tracts (horizontal) and median pontine raphe nuclei (vertical)
- Diagnosis: Multiple System Atrophy - Cerebellar type (MSA-C); also seen in spinocerebellar ataxias
- Precursor: Vertical line alone = "vertical line sign" (earlier stage)
4. Hummingbird Sign (Penguin Sign)
- Modality: T1 mid-sagittal
- Appearance: Severe atrophy of the midbrain tegmentum with relative preservation of the pons, giving the midbrain the profile of a hummingbird's head and the pons its beak/body
- Diagnosis: Progressive Supranuclear Palsy (PSP)
- Also called the "Penguin sign" due to similar sagittal profile
5. Mickey Mouse Sign
- Modality: T2 axial through midbrain
- Appearance: The midbrain and superior cerebellar peduncles resemble the silhouette of Mickey Mouse ears
- Diagnosis: PSP (same disease as hummingbird sign, different orientation)
6. Eye of the Tiger Sign
- Modality: T2 axial through basal ganglia
- Appearance: Bilateral globus pallidus shows a central zone of T2 hyperintensity (gliosis/spongiosis) surrounded by a hypointense ring (iron accumulation) - resembling a tiger's eye
- Diagnosis: Pantothenate Kinase-Associated Neurodegeneration (PKAN), formerly Hallervorden-Spatz disease
- Also reported (non-pathognomonic) in: corticobasal degeneration, early-onset parkinsonism
7. Panda Sign (Face of the Panda)
- Modality: T2 axial through midbrain
- Appearance: T2 hyperintensity in the mesencephalon gives the appearance of a panda's face - red nuclei appear as the eyes, tegmentum as the face, and superior colliculi as ears
- Diagnosis: Wilson's disease (hepatolenticular degeneration)
- Seen in only ~12% but is the only MRI feature that distinguishes Wilson's from other early-onset extrapyramidal disorders
- Note: A "giant panda cub" sign also described in the pons in Wilson's disease
TUMOUR-RELATED SIGNS
8. Dural Tail Sign
- Modality: Post-gadolinium T1
- Appearance: Linear enhancement of the dura extending away from a dural-based mass, tapering like a tail
- Diagnosis: Meningioma (classic); also seen in schwannoma, dural metastases, pituitary macroadenoma
- NOT pathognomonic - occurs in ~60-72% of meningiomas
- Broad dural base + dural tail = hallmark of extra-axial lesion

9. Butterfly Sign (Butterfly Glioma)
- Modality: T2/FLAIR axial
- Appearance: A glioma (typically GBM) that crosses the corpus callosum bilaterally, producing a butterfly-shaped T2 hyperintense mass spanning both hemispheres
- Diagnosis: Glioblastoma multiforme (GBM) - WHO Grade IV; also lymphoma
- Indicates direct spread via white matter commissures - poor prognosis
10. Figure-of-8 Sign (Snowman Sign)
- Modality: T1 sagittal / coronal
- Appearance: A pituitary macroadenoma expands the sella and then grows superiorly; as it squeezes through the diaphragma sellae, an indentation (waist) develops giving it a figure-of-8 or snowman appearance
- Diagnosis: Pituitary macroadenoma (>1 cm)
11. Horseshoe Sign (Open Ring Sign)
- Modality: Post-gadolinium T1
- Appearance: Incomplete ring of enhancement where the open (non-enhancing) side faces the cortex/grey matter
- Diagnosis: Tumefactive MS plaques - helps distinguish from abscess or tumour (which tend to have closed, complete rings)
12. Claw Sign
- Modality: T1/T2
- Appearance: Cerebral parenchyma surrounding the tumour like a claw, confirming the lesion is intra-axial (within the brain)
- Diagnosis: Differentiates intra-axial from extra-axial tumours
13. Salt and Pepper Sign
- Modality: T1/T2 axial at jugular foramen level
- Appearance: Heterogeneous mass with dark and bright areas intermixed (flow voids = dark "pepper"; haemorrhage/slow flow = bright "salt")
- Diagnosis: Glomus jugulare (paraganglioma) - highly vascular tumour at the jugular foramen
14. Medusa Head Sign (Caput Medusae)
- Modality: Post-gadolinium T1
- Appearance: Multiple small draining veins radiating outward from a central collecting vein, resembling the hair of Medusa
- Diagnosis: Developmental Venous Anomaly (DVA / cerebral venous angioma) - most common vascular malformation of the brain; usually benign
VASCULAR / HAEMORRHAGIC SIGNS
15. Empty Delta Sign (Delta Sign)
- Modality: Post-contrast CT / MRI
- Appearance: Triangular (delta-shaped) superior sagittal sinus with peripheral dural enhancement and a non-enhancing central filling defect (the clot)
- Diagnosis: Superior Sagittal Sinus Thrombosis (SSST) / Cerebral Venous Thrombosis
- On non-contrast CT: the thrombosed sinus appears hyperdense = "Dense triangle sign" or "Triangle sign"
16. Cord Sign
- Modality: CT / MRI
- Appearance: Hyperdense cortical vein on CT or T1 hyperintense vein on MRI, shaped like a cord
- Diagnosis: Cortical venous thrombosis
17. Hyperdense MCA Sign
- Modality: Non-contrast CT (not MRI but commonly tested)
- Appearance: Spontaneous hyperdensity of the middle cerebral artery on CT = fresh thrombus
- Diagnosis: Acute MCA occlusion / ischaemic stroke
18. MCA Dot Sign
- Modality: CT
- Appearance: Focal hyperdensity within the Sylvian fissure (M2 MCA branch level)
- Diagnosis: M2 MCA thrombus
19. Bathing Appearance (Subarachnoid / Meningeal Enhancement)
- Modality: Post-gadolinium FLAIR or T1
- Appearance: CSF spaces and sulci appear to "bathe" in enhancement / high signal - the brain is surrounded by abnormal signal like it is bathing in fluid
- Diagnosis: Leptomeningeal disease - meningitis, leptomeningeal carcinomatosis, subarachnoid haemorrhage (blood in sulci on FLAIR), or meningeal metastases
20. Ivy Sign
- Modality: Post-gadolinium T1 FLAIR
- Appearance: Leptomeningeal enhancement forming a "creeping ivy" pattern over the brain surface - fine, linear enhancement along sulci
- Diagnosis: Moyamoya disease - represents extensive leptomeningeal collateral vessels
21. Brush Sign
- Modality: SWI / T2*
- Appearance: Brush-like striation pattern along cortical veins (engorged medullary veins), seen in Moyamoya disease
- Diagnosis: Severity indicator in Moyamoya
DEVELOPMENTAL / CONGENITAL SIGNS
22. Molar Tooth Sign
- Modality: T2 axial at the level of the pons/cerebellum
- Appearance: Elongated, thick superior cerebellar peduncles combined with a deep interpeduncular fossa give the brainstem the appearance of a molar tooth on axial view
- Diagnosis: Joubert syndrome (a ciliopathy) - pathognomonic
- Associated with the "bat wing" appearance of the 4th ventricle on axial view
23. Bat Wing Appearance
- Modality: T2 axial
- Appearance: The 4th ventricle appears enlarged and shaped like bat wings, with vermian aplasia/hypoplasia
- Diagnosis: Joubert syndrome (same lesion as molar tooth, different slice level)
24. Radial Band Sign
- Modality: Proton density / FLAIR
- Appearance: Hyperintense bands radiating from the ventricular margin to the subcortical region, like spokes of a wheel
- Diagnosis: Tuberous sclerosis - represents transmantle migration lines between cortical tubers and subependymal nodules
METABOLIC / TOXIC SIGNS
25. Lentiform Fork Sign
- Modality: T2 / DWI
- Appearance: Hyperintensity outlining the lentiform nucleus in a fork shape - outer capsule + medial capsule enhancement surrounding the putamen/globus pallidus
- Diagnosis: Acute metabolic acidosis (uremic encephalopathy, methanol toxicity)
26. Mexican Hat Sign
- Modality: T2 axial
- Appearance: Central T2 hyperintensity in the pons with hypointense rim
- Diagnosis: Osmotic demyelination syndrome (Central Pontine Myelinolysis - CPM), caused by rapid correction of hyponatraemia
27. Boomerang Sign
- Modality: DWI / FLAIR
- Appearance: Transient T2/DWI hyperintensity in the splenium of the corpus callosum, shaped like a boomerang
- Diagnosis: Transient splenial lesion syndrome - causes include antiepileptic drug withdrawal, hypoglycaemia, Marchiafava-Bignami, rotavirus encephalitis, altitude illness
- Characteristically reversible
VASCULAR MALFORMATION SIGNS
28. Popcorn Sign (Cavernoma)
- Modality: T2* / SWI
- Appearance: Mixed signal mass with a dark (haemosiderin) peripheral rim and "popcorn-ball" internal signal - lobulated mixed T1/T2 signal from repeated haemorrhages at different stages
- Diagnosis: Cavernous malformation (cavernoma)
- No surrounding oedema, no enhancement = distinguishes from tumour
OPTIC / SKULL BASE SIGNS
29. Tram-Track Sign
- Modality: Post-gadolinium T1 / CT
- Appearance: Parallel lines of enhancement (or calcification) along the optic nerve sheath, like tram tracks, with a dark centre
- Diagnosis: Optic nerve sheath meningioma
- Also seen as cortical "tram-track" calcification in Sturge-Weber syndrome (brain CT)
QUICK REFERENCE SUMMARY TABLE
| Sign | Shape/Appearance | Sequence | Diagnosis |
|---|---|---|---|
| Dawson's Fingers | Fingers perpendicular to ventricles | Sagittal FLAIR | MS |
| Central Vein Sign | Vein within plaque | SWI | MS |
| Hot Cross Bun | Cross in pons | T2 axial | MSA-C |
| Hummingbird/Penguin | Midbrain beak profile | T1 sagittal | PSP |
| Mickey Mouse | Midbrain silhouette | T2 axial | PSP |
| Eye of the Tiger | Tiger eye in globus pallidus | T2 axial | PKAN (Hallervorden-Spatz) |
| Panda Sign | Panda face in midbrain | T2 axial | Wilson's disease |
| Dural Tail | Tapering dural enhancement | Post-Gd T1 | Meningioma |
| Butterfly | Bilateral corpus callosum mass | T2 axial | GBM / Lymphoma |
| Snowman/Figure-of-8 | Waist in pituitary mass | T1 sagittal | Pituitary macroadenoma |
| Horseshoe/Open Ring | Incomplete ring open toward cortex | Post-Gd T1 | Tumefactive MS |
| Bathing Appearance | Sulci filled with abnormal signal | Post-Gd FLAIR | Leptomeningeal disease |
| Empty Delta | Non-enhancing sinus in triangle | Post-Gd CT/MRI | SSST (venous thrombosis) |
| Medusa Head | Radiating draining veins | Post-Gd T1 | Developmental Venous Anomaly |
| Salt & Pepper | Mixed signal at jugular foramen | T1/T2 | Glomus jugulare |
| Ivy Sign | Leptomeningeal ivy-like enhancement | Post-Gd FLAIR | Moyamoya disease |
| Molar Tooth | Molar shape at pons level | T2 axial | Joubert syndrome |
| Bat Wing | Wide 4th ventricle | T2 axial | Joubert syndrome |
| Radial Band | Spokes from ventricle | PD / FLAIR | Tuberous sclerosis |
| Popcorn | Mixed signal + dark rim | T2* / SWI | Cavernoma |
| Lentiform Fork | Fork around lentiform nucleus | T2 / DWI | Metabolic acidosis |
| Boomerang | Reversible splenial lesion | DWI / FLAIR | Transient splenial syndrome |
| Tram Track | Parallel lines optic nerve | Post-Gd T1 | Optic nerve sheath meningioma |
| Cord Sign | Hyperdense/bright vein | CT / MRI | Cortical venous thrombosis |
| Claw Sign | Parenchyma grips tumour | T1/T2 | Intra-axial tumour confirmation |
Sources: Grainger & Allison's Diagnostic Radiology, 7th ed. | Bradley and Daroff's Neurology in Clinical Practice, 8th ed. | PMC - Twenty Classic Signs in Neuroradiology (IJRI 2009) | Radiopaedia Hot Cross Bun Sign
This is a shared conversation. Sign in to Orris to start your own chat.