Explain body fluid compartments with their regulation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed to produce a comprehensive, well-illustrated answer. Let me compile it.
Body Fluid Compartments and Their Regulation
1. Overview and Total Body Water
Total body water (TBW) makes up 60% of body weight in an average adult male (~42 L in a 70-kg man) and ~50% in females (who carry more adipose tissue). In premature neonates and newborns it reaches 70–75%. TBW is inversely correlated with body fat — muscle is ~75% water, fat is only ~10% water.
2. The Two Primary Compartments
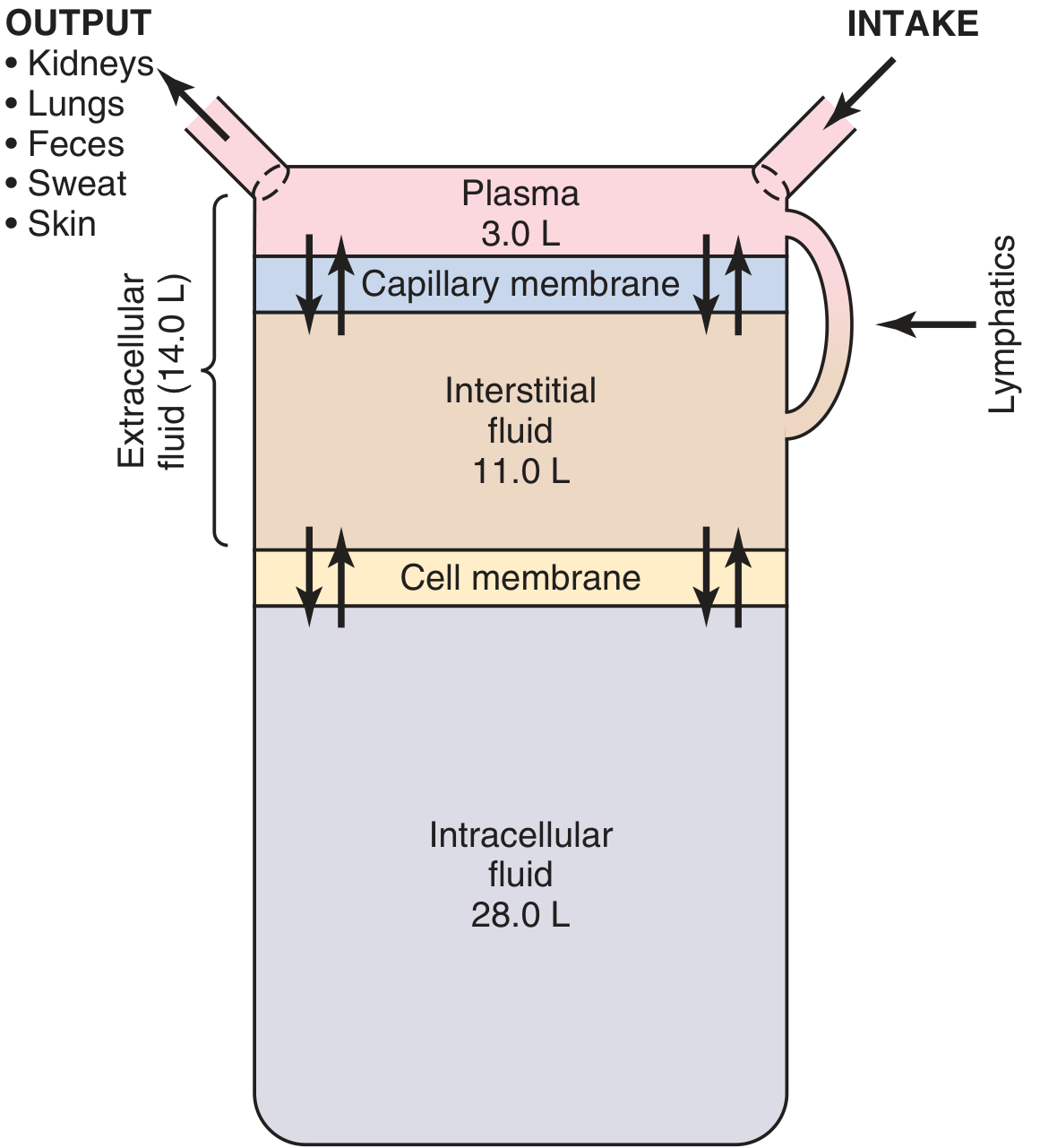
TBW is divided into two major compartments:
| Compartment | % Body Weight | % of TBW | Volume (70-kg man) |
|---|---|---|---|
| Total Body Water | 60% | 100% | 42 L |
| Intracellular Fluid (ICF) | 40% | 67% | 28 L |
| Extracellular Fluid (ECF) | 20% | 33% | 14 L |
| — Interstitial fluid | 15% | 25% | 11 L |
| — Plasma | 5% | 8% | 3 L |
| — Transcellular | ~2% | ~4% | 1–2 L |
3. Compartments in Detail
A. Intracellular Fluid (ICF)
- Constitutes 2/3 of TBW (~28 L in 70 kg man)
- Composed of trillions of individual cells, but treated collectively as one compartment because its ionic composition is remarkably similar across cell types
- Dominant cation: K⁺ (~42 mEq/kg body weight, mostly freely exchangeable)
- Also rich in Mg²⁺, phosphate, and organic anions (proteins, nucleotides)
- ICF volume is determined indirectly: TBW − ECF volume (no unique marker exists for direct measurement)
B. Extracellular Fluid (ECF)
ECF (~14 L) is divided into two main sub-compartments by the capillary wall:
Interstitial Fluid (~11 L, ~75% of ECF)
- Fluid bathing cells; essentially an ultrafiltrate of plasma
- The capillary wall is virtually impermeable to large proteins → interstitial fluid has very low protein content
- Gibbs-Donnan equilibrium slightly elevates diffusible cation and anion concentrations in interstitial fluid compared to plasma
Plasma (~3 L, ~25% of ECF)
- The non-cellular component of blood; continuously exchanges with interstitial fluid via capillary pores
- Key difference from interstitial fluid: high protein concentration (~7 g/dL, contributing ~0.8 mOsm/L oncotic pressure)
- Plasma + red blood cells = blood (~5 L, ~7% of body weight); hematocrit ~0.42 (men), ~0.38 (women)
Transcellular Fluid (~1–2 L)
- Specialized ECF in synovial, peritoneal, pericardial, intraocular spaces, and cerebrospinal fluid
- Composition may differ markedly from plasma
Dominant ECF cation: Na⁺ — sodium and its accompanying anions (Cl⁻, HCO₃⁻) are the major determinants of ECF volume.
4. Ionic Composition
| Ion | ECF (plasma) | ICF |
|---|---|---|
| Na⁺ | 142 mEq/L | 10 mEq/L |
| K⁺ | 4 mEq/L | 140 mEq/L |
| Ca²⁺ (free) | 2.4 mEq/L | ~0.0001 mEq/L |
| Mg²⁺ | 1.2 mEq/L | 58 mEq/L |
| Cl⁻ | 103 mEq/L | 4 mEq/L |
| HCO₃⁻ | 24 mEq/L | 10 mEq/L |
| Phosphate | 4 mEq/L | 75 mEq/L |
| Protein | 16 mEq/L | 74 mEq/L |
| Osmolarity | ~300 mOsm/L | ~300 mOsm/L |
Key rule: intracellular osmolarity always equals extracellular osmolarity at steady state. Water shifts freely across cell membranes to maintain this equilibrium.
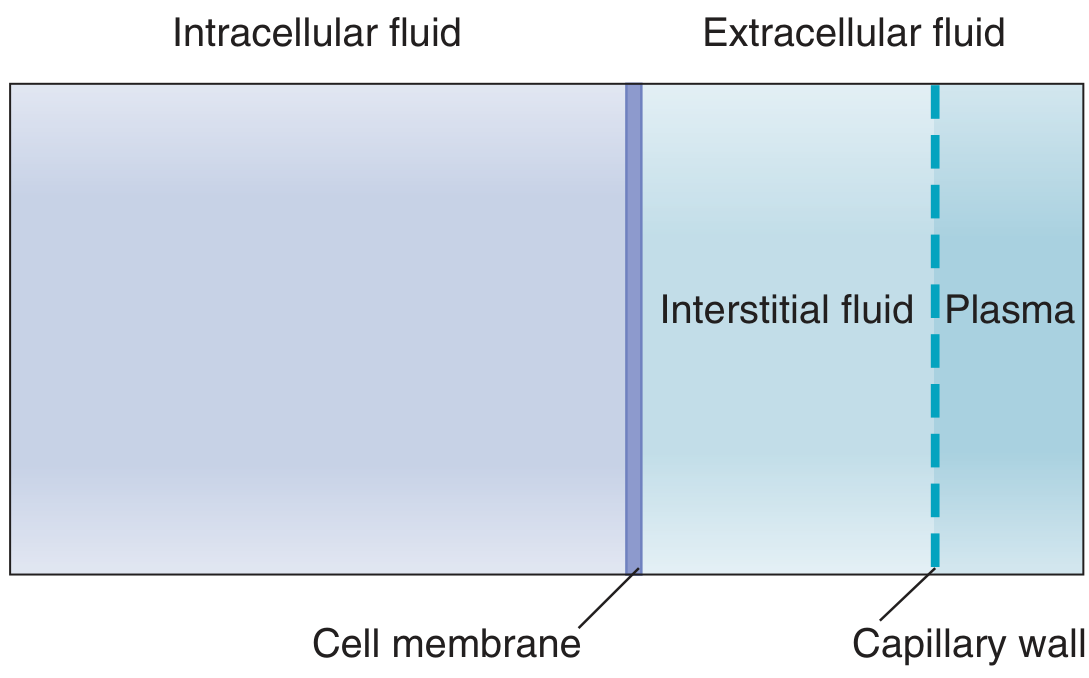
5. Barriers Separating Compartments
Cell Membrane (ICF ↔ ECF)
- Highly selective; maintains the Na⁺/K⁺ gradient via Na⁺/K⁺-ATPase
- Water crosses freely via aquaporins in response to osmotic gradients
- Large molecules, charged ions cross only via specific transporters or channels
Capillary Wall (Plasma ↔ Interstitial Fluid)
- Highly permeable to small solutes and water, but impermeable to proteins
- Fluid movement governed by Starling forces:
- Capillary hydrostatic pressure → drives fluid out
- Plasma oncotic pressure (colloid osmotic pressure, ~28 mmHg) → draws fluid in
- Interstitial hydrostatic pressure and oncotic pressure oppose or assist respectively
- Net filtration at arteriolar end → reabsorption at venous end
- Residual filtered fluid is returned via lymphatics
6. Osmolarity and Tonicity
Plasma osmolarity (normally ~290–300 mOsm/L) is estimated by:
Plasma Osm = 2 × [Na⁺] + Glucose/18 + BUN/2.8
- Multiplying Na⁺ × 2 accounts for its balancing anions (Cl⁻, HCO₃⁻)
- Na⁺ is the dominant determinant; glucose and urea contribute smaller amounts
Tonicity (effective osmolality) refers to solutes that cannot cross cell membranes freely:
- Isotonic (~282 mOsm/L): no cell volume change (e.g., 0.9% NaCl, D5W initially)
- Hypotonic (<282 mOsm/L): water enters cells → cell swelling
- Hypertonic (>282 mOsm/L): water exits cells → cell shrinkage
Urea freely crosses cell membranes → it is an ineffective osmole (contributes to osmolarity but not tonicity).
7. Regulation of Body Fluid Compartments
A. Osmoregulation (Water Balance)
Plasma osmolality is maintained within a remarkably narrow window (~285–295 mOsm/kg) by a high-sensitivity feedback loop:
Osmoreceptors in the paraventricular and supraoptic nuclei of the hypothalamus are equipped with mechanical stretch receptors that depolarize when cells shrink (hyperosmolality).
↑ Osmolality triggers:
- Thirst → increased water intake
- ADH (Vasopressin) release from posterior pituitary → binds V2 receptors on principal cells of collecting ducts → cyclic AMP cascade → translocation of aquaporin-2 (AQP2) to luminal membrane → increased water reabsorption → concentrated urine (up to 1,200 mOsm/kg)
↓ Osmolality triggers:
- Thirst suppression
- ADH suppression → collecting ducts become impermeable to water → dilute urine (as low as 50 mOsm/kg)
Non-osmotic stimuli for ADH release include: volume depletion, hypotension, sympathetic activation, pain, nausea, and hypoxia. Large decreases in blood pressure override the osmotic set point, causing massive ADH release regardless of osmolality to preserve volume.
"A 1-mOsm change in plasma osmolality results in a 95-fold change in urine osmolality" — Mulholland & Greenfield's Surgery
The countercurrent mechanism (loop of Henle + vasa recta) creates the hypertonic medullary interstitium necessary for ADH to concentrate urine:
- TAL actively pumps NaCl (without water) into interstitium
- Descending limb is water-permeable → fluid concentrates
- Urea recycling in medulla further enhances hypertonicity
B. Volume Regulation (ECF/Sodium Balance)
ECF volume is primarily determined by total body sodium content (Na⁺ + accompanying anions). Volume regulation is achieved through the kidney via several hormonal systems:
Renin-Angiotensin-Aldosterone System (RAAS)
Renin is released by juxtaglomerular cells of the afferent arteriole in response to:
- Decreased afferent arteriolar pressure (baroreceptor)
- Decreased NaCl delivery to macula densa (via NKCC2)
- Increased sympathetic outflow
Renin cleaves angiotensinogen → Angiotensin I → (ACE, in lungs/kidneys) → Angiotensin II, which:
- Directly increases Na⁺ reabsorption in the proximal tubule
- Stimulates aldosterone release from adrenal cortex
- Causes systemic vasoconstriction (V1 receptor)
Aldosterone → increases ENaC activity on luminal membrane of cortical collecting duct → Na⁺ reabsorption, K⁺ excretion. WNK kinases modulate aldosterone's differential effects during hypovolemia (conserve both Na⁺ and K⁺) vs. hyperkalemia (excrete K⁺ while reabsorbing Na⁺).
Atrial Natriuretic Peptide (ANP)
Released from atria when stretched by increased ECF volume:
- Dilates afferent arteriole, constricts efferent arteriole → ↑ GFR
- Inhibits ENaC in collecting ducts → natriuresis
- Net effect: ECF volume reduction back toward normal
Vasopressin (V1 Receptor) and Sympathetic System
- Vasopressin also enhances Na⁺ reabsorption in TAL and collecting duct
- Sympathetic activation → renal vasoconstriction → ↓ GFR → ↑ renin → volume retention
8. Fluid Shifts Between Compartments
Key principles governing fluid shifts (Costanzo):
- ECF volume is determined by its total solute content — primarily Na⁺ salts
- ICF osmolarity = ECF osmolarity at steady state (maintained by free water movement)
- Effective osmoles (NaCl, mannitol) stay confined to ECF and drive water movement
- Ineffective osmoles (urea) distribute throughout TBW without osmotic shift
| Disturbance | ECF Volume | Osmolarity | ICF Volume |
|---|---|---|---|
| Isotonic volume loss (diarrhea) | ↓ | Normal | Normal |
| Pure water loss (diabetes insipidus) | ↓ (slight) | ↑ | ↓ |
| Hypertonic NaCl gain | ↑ | ↑ | ↓ |
| Isotonic NaCl gain (IV saline) | ↑ | Normal | Normal |
| SIADH (water retention) | ↑ (slight) | ↓ | ↑ |
| Adrenal insufficiency (Na⁺ loss) | ↓ | ↓ | ↑ |
9. Measuring Compartment Volumes
The dilution principle (indicator dilution method) is used:
| Compartment | Markers |
|---|---|
| TBW | ³H₂O, ²H₂O (deuterium), antipyrine |
| ECF | ²²Na, sulfate, mannitol, inulin |
| Plasma | Radioiodinated albumin (RISA), Evans blue dye |
| ICF | Calculated: TBW − ECF |
| Interstitial fluid | Calculated: ECF − Plasma volume |
Summary
The body's ~42 L of water is partitioned into ICF (28 L, K⁺-rich) and ECF (14 L, Na⁺-rich), separated by the cell membrane (osmotically driven) and capillary wall (Starling forces). Regulation operates through two parallel systems: osmoregulation (hypothalamic osmoreceptors → ADH → aquaporin-2 insertion → urine concentration) maintains constant osmolality, while volume regulation (RAAS → aldosterone + ANP + sympathetics) controls total body Na⁺ and thus ECF volume. These two systems interact — notably, severe hypovolemia overrides osmolality setpoints, causing ADH release even in hypotonic states, prioritizing volume preservation over tonicity.
Sources: Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology 7e; Mulholland & Greenfield's Surgery 7e; National Kidney Foundation Primer on Kidney Diseases 8e
Short and long term regulation of body fluid balance
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Can I have a answer of my question?
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.