Tuberculosis bhms 3rd year
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive content from all major sources. Here is the complete BHMS 3rd year-level note on Tuberculosis:
Tuberculosis - BHMS 3rd Year
1. Definition
Tuberculosis (TB) is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the body.
- Robbins & Kumar Basic Pathology
2. Causative Organism
| Property | Detail |
|---|---|
| Organism | Mycobacterium tuberculosis hominis (most common) |
| Type | Weakly gram-positive, strongly acid-fast, aerobic rods |
| Cell wall | Lipid-rich (mycolic acids) - resists disinfectants, detergents, and common antibiotics |
| Key property | Capable of intracellular growth in alveolar macrophages |
| Stain | Ziehl-Neelsen (carbol fuchsin) - appears red on blue background |
| Other species | M. bovis (bovine TB, from unpasteurized milk); M. avium complex (in AIDS patients) |
Humans are the only natural reservoir. Spread is by person-to-person aerosol inhalation.
- Medical Microbiology 9e
3. Epidemiology
-
One of the leading infectious causes of death globally; WHO estimated 10 million new cases and 1.3 million deaths in 2021
-
One-third of the global population is asymptomatically infected; only 5-10% develop clinical disease during their lifetime
-
An infectious TB patient can infect 10-15 persons per year
-
High burden countries: India, Pakistan, sub-Saharan Africa, South Africa, China, Eastern Europe
-
MDR-TB: 3.3% of new cases; 18% of previously treated cases had MDR/RR-TB
-
Risk factors: poverty, overcrowding, malnutrition, HIV/AIDS, diabetes, silicosis, chronic renal failure, Hodgkin lymphoma, alcohol use disorder, immunosuppression
-
Park's Textbook of Preventive and Social Medicine; Robbins & Kumar Basic Pathology
4. Pathogenesis
Key Concept: Infection vs. Disease
- Infection = seeding of a focus with organisms (may not cause disease)
- Disease = clinically significant tissue damage
Sequence of Events (see diagram below):
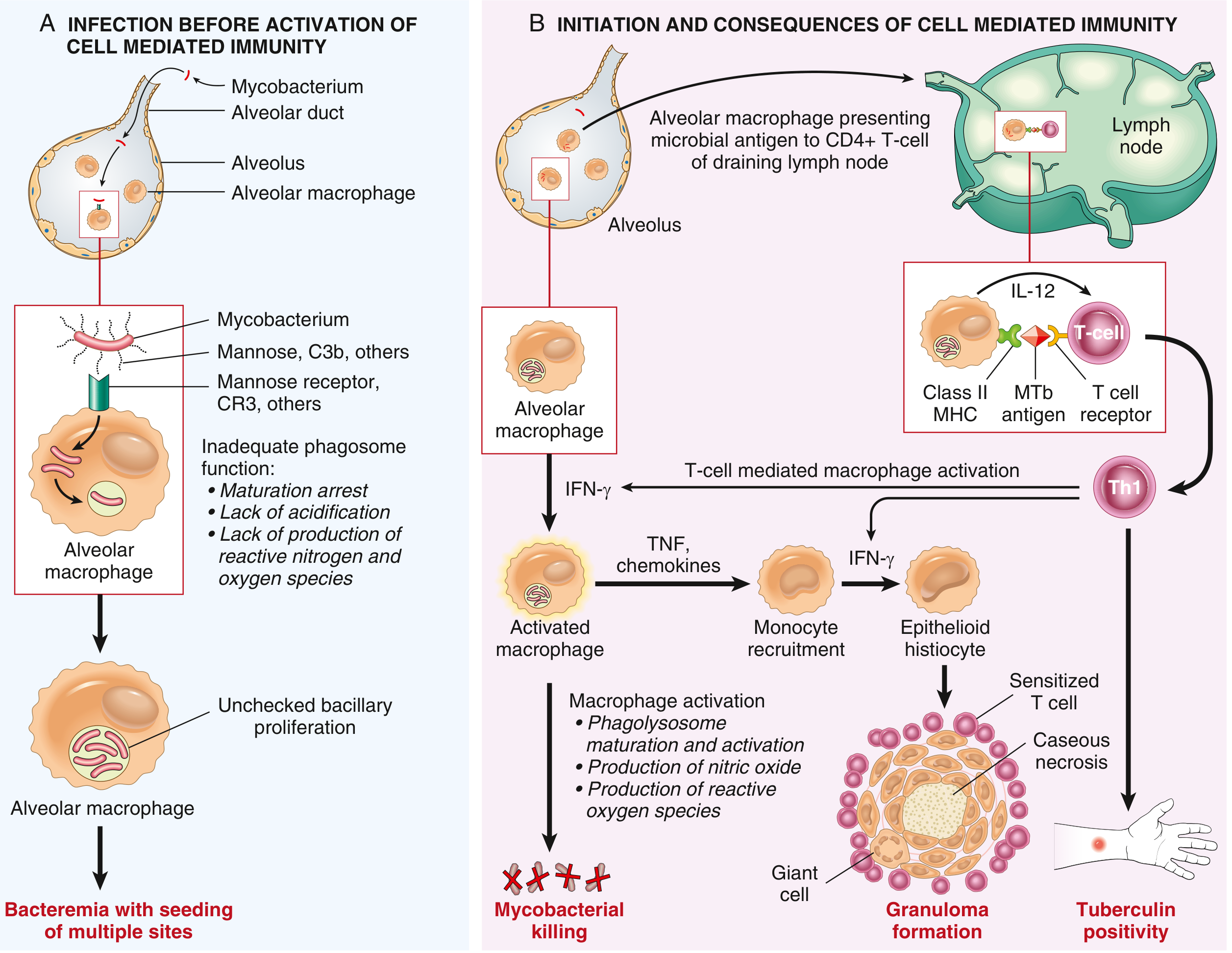
Phase A - First 3 weeks (Before cell-mediated immunity):
- Mycobacteria inhaled → enter alveolar macrophages via mannose receptors and complement receptors (CR3)
- Organisms inhibit phagolysosome fusion → prevent acidification and killing → proliferate unchecked in macrophages
- Bacteremia occurs → organisms seed multiple body sites
- Patient is usually asymptomatic or has mild flu-like illness
Phase B - After 3 weeks (Cell-mediated immunity develops):
- Macrophages present mycobacterial antigens to CD4+ T cells via MHC Class II
- Under macrophage-secreted IL-12, CD4+ T cells differentiate into Th1 cells
- Th1 cells secrete IFN-γ → activates macrophages
- Activated macrophages produce: nitric oxide, reactive oxygen species → kill mycobacteria
- TNF secreted → recruits more monocytes
- Macrophages differentiate into epithelioid histiocytes → form granulomas
- Some epithelioid cells fuse → Langhans giant cells
- Outcome: granuloma formation + caseous necrosis + tuberculin skin test positivity
Important: Immunity and hypersensitivity are two sides of the same coin - the same Th1 cells that mediate protection also cause tissue destruction (caseation).
- Robbins & Kumar Basic Pathology, p. 475-476
5. Primary Tuberculosis
- Occurs in a previously unexposed, unsensitized host
- ~5% of newly infected individuals develop significant disease
Ghon Complex (Morphology):
- Bacilli implant in distal air spaces of lower upper lobe or upper lower lobe, close to pleura
- A 1-1.5 cm gray-white area of consolidation forms = Ghon focus (often with central caseous necrosis)
- Bacilli travel via lymphatics to regional hilar lymph nodes (also caseate)
- Ghon complex = Ghon focus + affected regional lymph nodes (parenchymal + nodal lesion)
- Hematogenous dissemination occurs in first few weeks
- In ~95% of cases, cell-mediated immunity controls the infection → Ghon complex undergoes progressive fibro-calcification
Progressive Primary TB:
- Occurs in immunocompromised (especially HIV+ with CD4 < 200 cells/µL), severely malnourished
- No granuloma formation (cannot mount CD4+ T cell response)
6. Secondary (Reactivation) Tuberculosis
- Arises in a previously sensitized host
- May follow primary TB (reactivation of dormant lesions, even decades later) or reinfection
- Only < 5% of primary disease progresses to secondary TB
Key Features:
| Feature | Primary TB | Secondary TB |
|---|---|---|
| Host | Unsensitized | Previously sensitized |
| Location | Lower upper lobe / upper lower lobe (subpleural) | Apex of upper lobe (bilateral) |
| Lymph node involvement | Prominent (Ghon complex) | Less prominent |
| Cavitation | Uncommon | Common (erodes airways) |
| Granulomas | Yes (once CMI develops) | Yes, more vigorous |
| Infectivity | Low | High (sputum contains bacilli) |
| Tuberculin test | Converts positive | Already positive |
Morphology of Secondary TB:
- Initial lesion: small (<2 cm) consolidation, 1-2 cm from apical pleura
- Sharply circumscribed, firm, gray-yellow areas with central caseation + peripheral fibrosis
- Active lesions: coalescent granulomas with central caseation (histologically)
- Resolution leaves fibrocalcific scars
Histological appearances of TB:
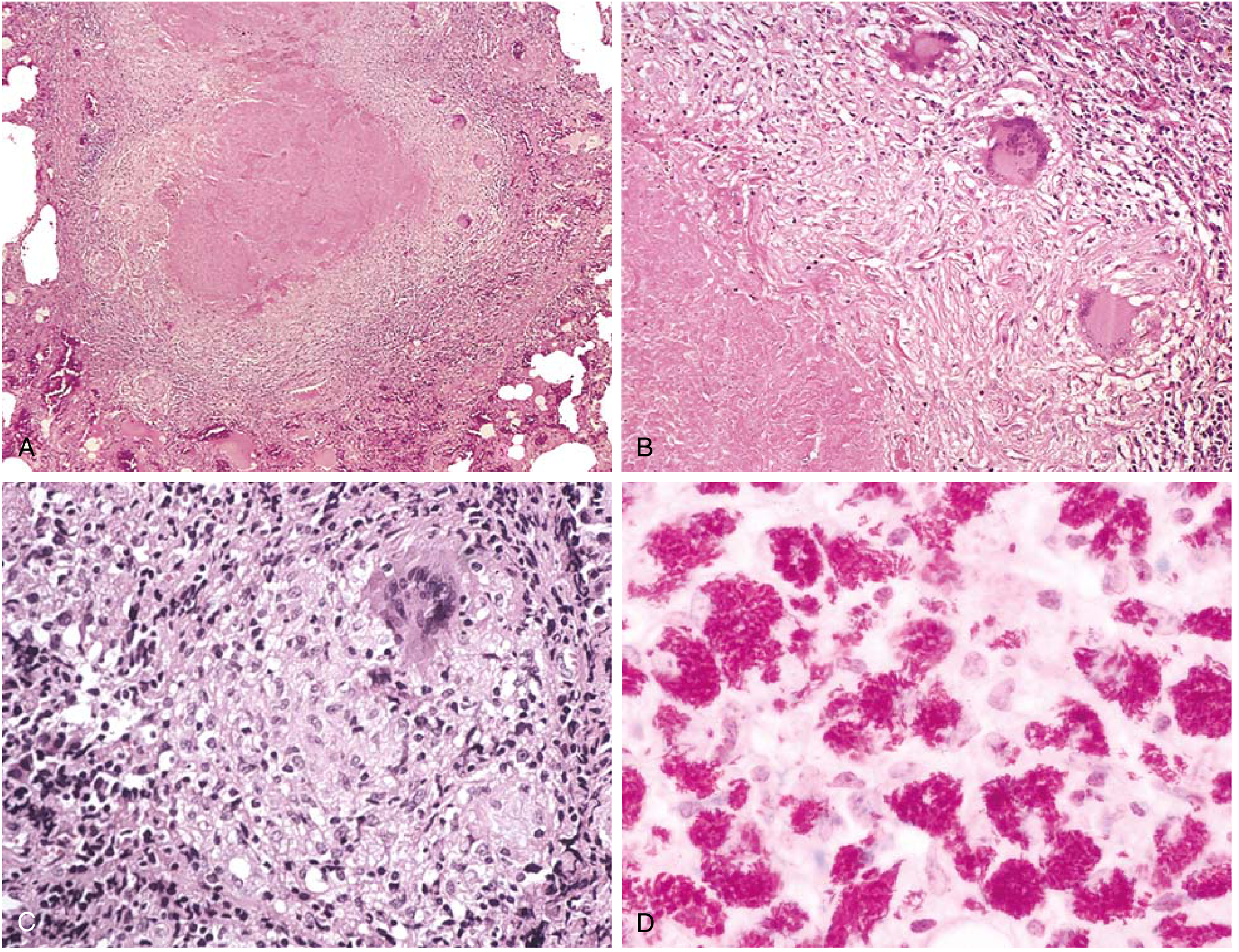
- A: Low-power - central caseating necrosis surrounded by granulomatous inflammation
- B: Fibrous wall with caseous necrosis
- C: High-power - epithelioid histiocytes + Langhans giant cell
- D: Acid-fast bacilli (red rods on ZN stain)
7. Complications / Forms of Progressive TB
| Complication | Mechanism / Notes |
|---|---|
| Miliary TB | Hematogenous dissemination → millet seed-sized granulomas in lungs, liver, spleen, bone marrow, meninges |
| Caseous pneumonia | Liquefied caseum spills into airways → consolidation of an entire lobe |
| Cavitary TB | Drainage of caseum into bronchus → cavity formation (most infectious) |
| Tuberculous pleuritis | Pleural effusion from rupture of a subpleural focus |
| TB meningitis | Spread from miliary TB to meninges |
| Pott's disease | Vertebral TB - most common form of skeletal TB |
| Scrofula | Cervical lymphadenopathy from TB |
| TB in HIV | Extrapulmonary TB >50% when CD4 <200; atypical presentation |
8. Diagnosis
| Test | Details |
|---|---|
| Tuberculin (Mantoux) test | Intradermal PPD (purified protein derivative); induration read at 48-72 hrs; positive = delayed hypersensitivity (Th1 mediated) |
| IGRA (IFN-γ release assay) | In vitro; T cells stimulated with MTb antigens; IFN-γ measured; less affected by BCG |
| Sputum smear (ZN stain) | Acid-fast bacilli (AFB); rapid, cheap, but low sensitivity |
| Sputum culture (gold standard) | Lowenstein-Jensen medium; slow (4-8 weeks); confirms diagnosis |
| CBNAAT/GeneXpert MTB/RIF | Rapid molecular test; detects MTb + rifampicin resistance simultaneously |
| Chest X-ray | Upper lobe infiltrates, cavitation (secondary); hilar adenopathy + lower lobe consolidation (primary) |
False-negatives for tuberculin test: viral infections, sarcoidosis, malnutrition, Hodgkin lymphoma, overwhelming TB, immunosuppression (anergy)
False-positives: atypical mycobacterial infections
- Medical Microbiology 9e; Robbins & Kumar Basic Pathology, p. 476
9. Treatment
Standard Regimen (RNTCP/NTEP - India):
| Phase | Duration | Drugs | Mnemonic |
|---|---|---|---|
| Intensive phase | 2 months | Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) | 2 HRZE |
| Continuation phase | 4 months | Isoniazid (H) + Rifampicin (R) | 4 HR |
Total duration: 6 months for new pulmonary TB
Drug Mnemonics:
- RIPE = Rifampicin, Isoniazid, Pyrazinamide, Ethambutol (first-line drugs)
- SHREK = Streptomycin, isoniazid (H), Rifampicin, Ethambutol, piraZinamide (second-line and reserve)
Key Side Effects:
| Drug | Important Side Effect |
|---|---|
| Isoniazid (INH) | Peripheral neuropathy (→ give pyridoxine/B6), hepatotoxicity |
| Rifampicin | Orange-red discoloration of urine/secretions, hepatotoxicity, enzyme inducer |
| Pyrazinamide | Hyperuricemia (gout), hepatotoxicity |
| Ethambutol | Optic neuritis (color blindness, visual acuity loss) |
| Streptomycin | Ototoxicity, nephrotoxicity |
Drug-Resistant TB:
-
MDR-TB: resistant to at least Isoniazid + Rifampicin (the two most effective drugs)
-
XDR-TB: MDR-TB + resistance to any fluoroquinolone + at least one of bedaquiline/linezolid
-
Treatment: 18-20 months with second-line agents
-
Medical Microbiology 9e; Sherris & Ryan's Medical Microbiology
10. Prevention and Control
BCG Vaccine:
- Bacillus Calmette-Guérin (BCG) - live attenuated M. bovis
- Given at birth (part of UIP in India)
- Protective efficacy: 28-60% (mainly prevents disseminated/miliary TB and TB meningitis in children)
- Does not prevent adult pulmonary TB reliably
DOTS (Directly Observed Treatment Short-course):
- 5 components of DOTS strategy:
- Political commitment
- Case detection by sputum smear microscopy
- Standardized short-course chemotherapy under direct observation
- Regular, uninterrupted drug supply
- Standardized recording and reporting system
RNTCP / NTEP (India):
- India's National TB Elimination Programme (NTEP) aims to eliminate TB by 2025 (5 years ahead of the global target of 2030)
- Nikshay portal for TB case notification
- Ni-kshay Poshan Yojana - nutritional support Rs 500/month to TB patients
Chemoprophylaxis:
-
Isoniazid preventive therapy (IPT) for 6-9 months for high-risk contacts (household contacts of smear-positive cases, HIV-positive patients)
-
Park's Textbook of Preventive and Social Medicine
11. Extrapulmonary TB - Key Points for Exams
| Site | Clinical Features |
|---|---|
| Lymph nodes (most common extrapulmonary) | Cervical scrofula; matted, painless nodes; collar-stud abscess |
| Pleura | Exudative pleural effusion; lymphocytic; ADA elevated |
| Spine (Pott's disease) | Gibbus deformity; paraplegia possible |
| Kidney | Sterile pyuria (WBCs in urine, negative routine culture) |
| Meninges | TB meningitis; basal meningitis; CN palsies |
| Intestine | Ileocaecal region most common; malabsorption, obstruction |
| Miliary | Multiple organ involvement; fever, hepatosplenomegaly, choroidal tubercles on fundus |
12. Quick Revision Points (High-yield for BHMS Exams)
- Causative organism: M. tuberculosis - acid-fast bacillus
- Stain: Ziehl-Neelsen (ZN stain) - red on blue background
- Ghon complex = Ghon focus + hilar lymph node involvement (primary TB)
- Secondary TB: apex of upper lobe, cavitation, high infectivity
- Granuloma components: Epithelioid histiocytes + Langhans giant cells + caseous necrosis + lymphocytes
- Immunity: Th1 / CD4+ T cells (cell-mediated immunity); IFN-γ is the key cytokine
- Tuberculin test: delayed hypersensitivity (Type IV) - read at 48-72 hours
- Treatment: 2 HRZE + 4 HR (6 months total for new cases)
- Most common site of extrapulmonary TB: lymph nodes (cervical)
- Most common site of skeletal TB: vertebral column (Pott's disease)
- MDR-TB = resistant to INH + Rifampicin
- BCG: live attenuated M. bovis
- Key side effect to remember: Ethambutol → optic neuritis; INH → peripheral neuropathy; Rifampicin → orange urine
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Medical Microbiology 9e; Sherris & Ryan's Medical Microbiology; Park's Textbook of Preventive and Social Medicine
This is a shared conversation. Sign in to Orris to start your own chat.