
1000182128.jpg
Explain this
analyse_media
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a full clinical explanation of the image and the exam-style questions:
What is seen in this picture?
Spider Angioma (also called spider nevus, vascular spider, or nevus araneus)
The image shows a classic spider angioma on the skin of a chronic alcoholic patient presenting with abdominal distension. You can see:
- A central red arteriole ("body" of the spider)
- Multiple fine radiating vessels spreading outward like the legs of a spider
This is the textbook appearance. Here is a reference image from Harrison's showing the same finding in a cirrhosis patient:
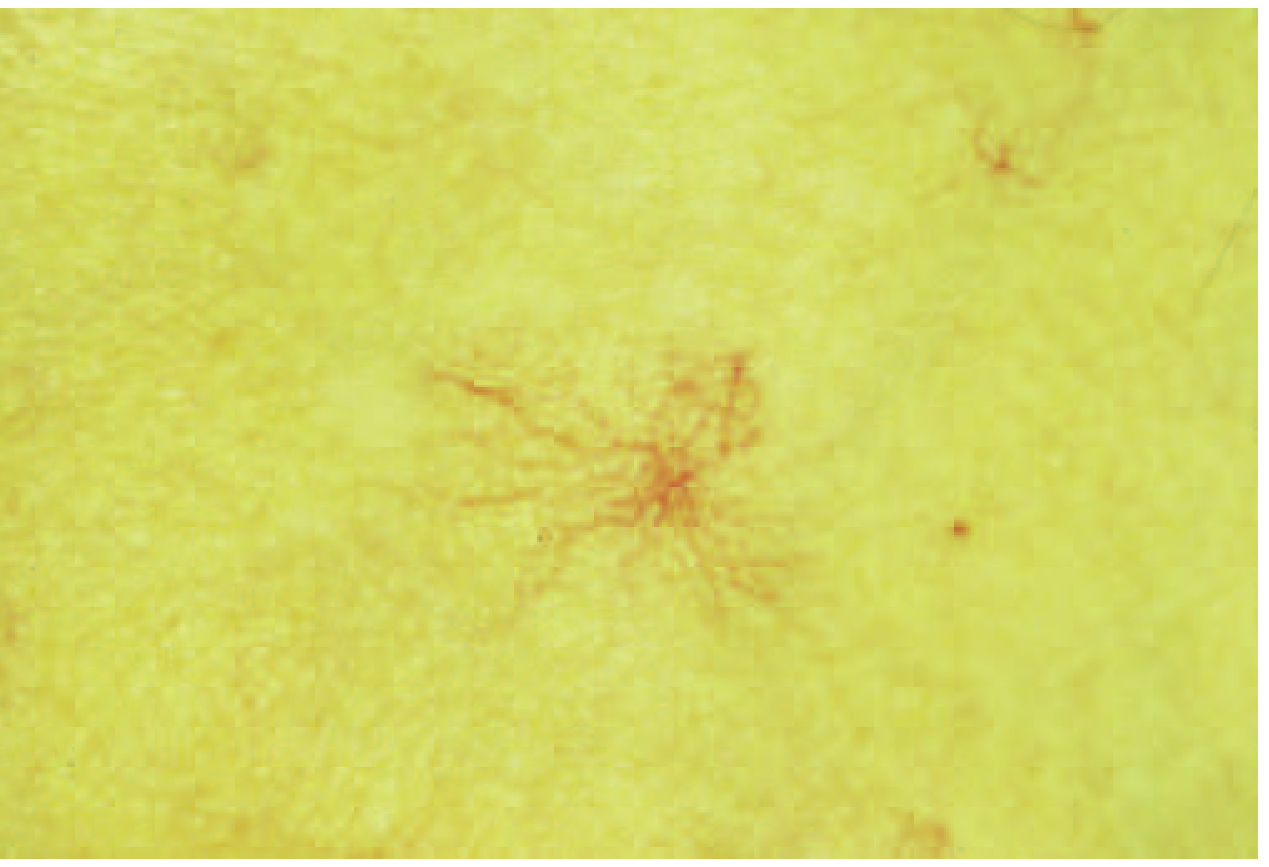
A bedside diagnostic trick: press on the center - the lesion blanches completely, and when you release, blood refills from the center outward.
Pathophysiology (Why does this happen?)
In chronic alcohol-related liver disease / cirrhosis:
- The damaged liver fails to metabolize estrogen, leading to hyperestrogenism
- Elevated estrogens + increased circulating angiogenic factors (VEGF, basic FGF) drive dilation of the central arteriole and formation of the radiating vessels
- Spider angiomas appear predominantly in the distribution of the superior vena cava - face, neck, upper chest, upper arms
About one-third of patients with chronic liver disease will develop spider nevi, and their frequency increases with worsening liver fibrosis. - Yamada's Textbook of Gastroenterology, 7e
Differential Diagnosis
| Condition | How to distinguish |
|---|---|
| Simple telangiectasia | Linear fine vessels, no central arteriole, no pulsation |
| Hereditary Hemorrhagic Telangiectasia (Osler-Weber-Rendu) | Multiple telangiectasias on lips, tongue, fingertips; family history; recurrent epistaxis |
| Cherry angioma | Dome-shaped red papule, does NOT radiate legs, does not blanch from center |
| Unilateral nevoid telangiectasia | Follows a dermatomal distribution |
| Venous lake | Dark blue, compressible, on sun-exposed areas (ear, lips) |
| Basal cell carcinoma | Pearly rolled edge, associated ulceration, telangiectasias are over the tumor |
The key distinguishing feature of spider angioma is the pulsatile central arteriole and centrifugal blanching on pressure. - Andrews' Diseases of the Skin, Clinical Dermatology
Treatment
1. Treat the underlying liver disease (primary)
- Alcohol cessation - most important; spider angiomas can involute with disease improvement
- Nutritional support (thiamine, folate, multivitamins)
- Management of portal hypertension and ascites:
- Dietary sodium restriction
- Diuretics: spironolactone (first-line) +/- furosemide
- Large-volume paracentesis for tense ascites
- Evaluate for liver transplantation in advanced disease
- Screen for varices (upper GI endoscopy) and hepatocellular carcinoma (USS + AFP)
2. Local treatment of the spider angioma (cosmetic/secondary)
- Pulsed dye laser (PDL) - most effective, no scarring
- Electrodesiccation / electrocautery - effective in experienced hands
- Cryotherapy - alternative option
Note: In this patient's context (abdominal distension = likely ascites from cirrhosis), systemic management is the priority. Cosmetic treatment is secondary. - Andrews' Diseases of the Skin; Harrison's Principles of Internal Medicine, 22e
Full Clinical Picture of Alcohol-Associated Cirrhosis
Spider angiomas in this patient are part of a wider constellation of signs. Other findings to look for include:
- Palmar erythema - peripheral erythema of palms
- Terry's nails - white nails with distal pink band
- Jaundice / scleral icterus
- Gynecomastia + testicular atrophy (males) - due to hyperestrogenism
- Parotid enlargement
- Caput medusae - dilated periumbilical veins (portal hypertension)
- Ascites - the abdominal distension this patient presented with
- Dupuytren's contracture
- Leukonychia / half-and-half nails
The classic triad of spider angiomas + palmar erythema + pallid nails with distal hyperemic bands should strongly raise suspicion for cirrhosis. - Harrison's Principles of Internal Medicine, 22e
This is a shared conversation. Sign in to Orris to start your own chat.