Explain neuroanatomy core concepts
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I have comprehensive content from authoritative textbooks. Now I'll compose the full neuroanatomy core concepts guide.
Neuroanatomy: Core Concepts
Sources: Neuroanatomy through Clinical Cases, 3rd Ed. | Gray's Anatomy for Students | Rosen's Emergency Medicine
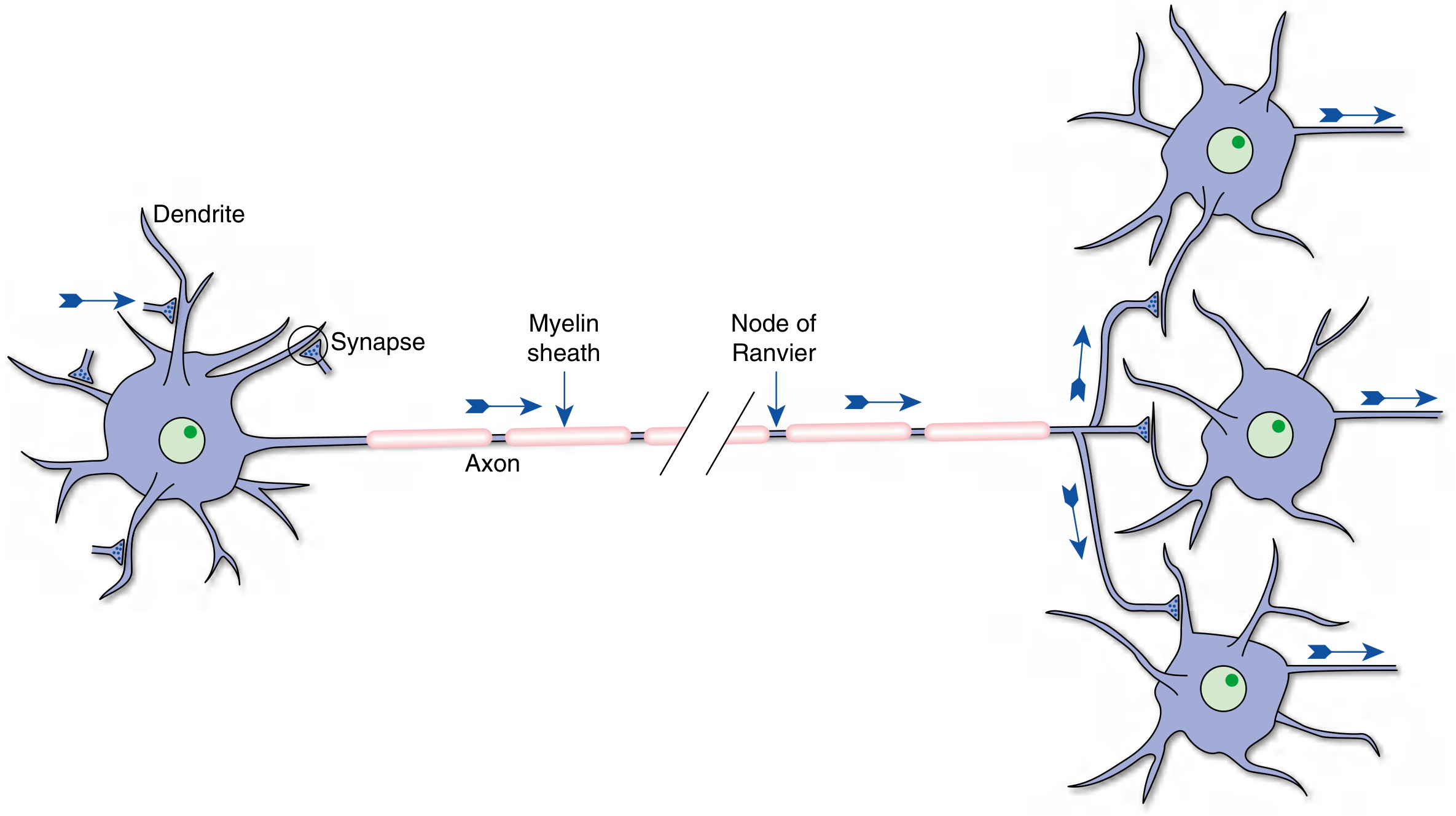
1. The Neuron - Basic Unit
The neuron is the fundamental signaling cell of the nervous system. Its key structural components are:
| Part | Description | Primary Function |
|---|---|---|
| Dendrites | Tapered extensions of cell body | Collect information from other neurons |
| Soma (cell body) | Contains nucleus, Golgi apparatus, Nissl substance | Synthesize macromolecules; integrate electrical signals |
| Axon | Single, cylindrical; may be myelinated or unmyelinated | Conduct signals to other neurons |
| Axon terminals | Vesicle-filled apposition to part of another neuron | Transmit information via neurotransmitters |
Saltatory conduction: In myelinated axons, the action potential jumps from one node of Ranvier to the next, dramatically increasing conduction velocity. The myelin sheath is produced by oligodendrocytes (CNS) and Schwann cells (PNS). - Neuroanatomy through Clinical Cases, 3rd Ed.
2. CNS vs. PNS Division
The nervous system divides into two large systems:
- Central Nervous System (CNS): Brain + spinal cord
- Peripheral Nervous System (PNS): All nerves outside the CNS (spinal nerves, cranial nerves, autonomic ganglia)
Functionally, this further divides into:
- Somatic nervous system - conscious sensation and voluntary skeletal muscle control
- Visceral (autonomic) nervous system - homeostatic regulation of internal organs, involuntary
- Sympathetic ("fight-or-flight")
- Parasympathetic ("rest-and-digest")
3. The Cerebral Hemispheres and Lobes
The brain's outer surface (cerebral cortex) is folded into ridges called gyri and grooves called sulci. Deep grooves are called fissures. This folding massively increases surface area.
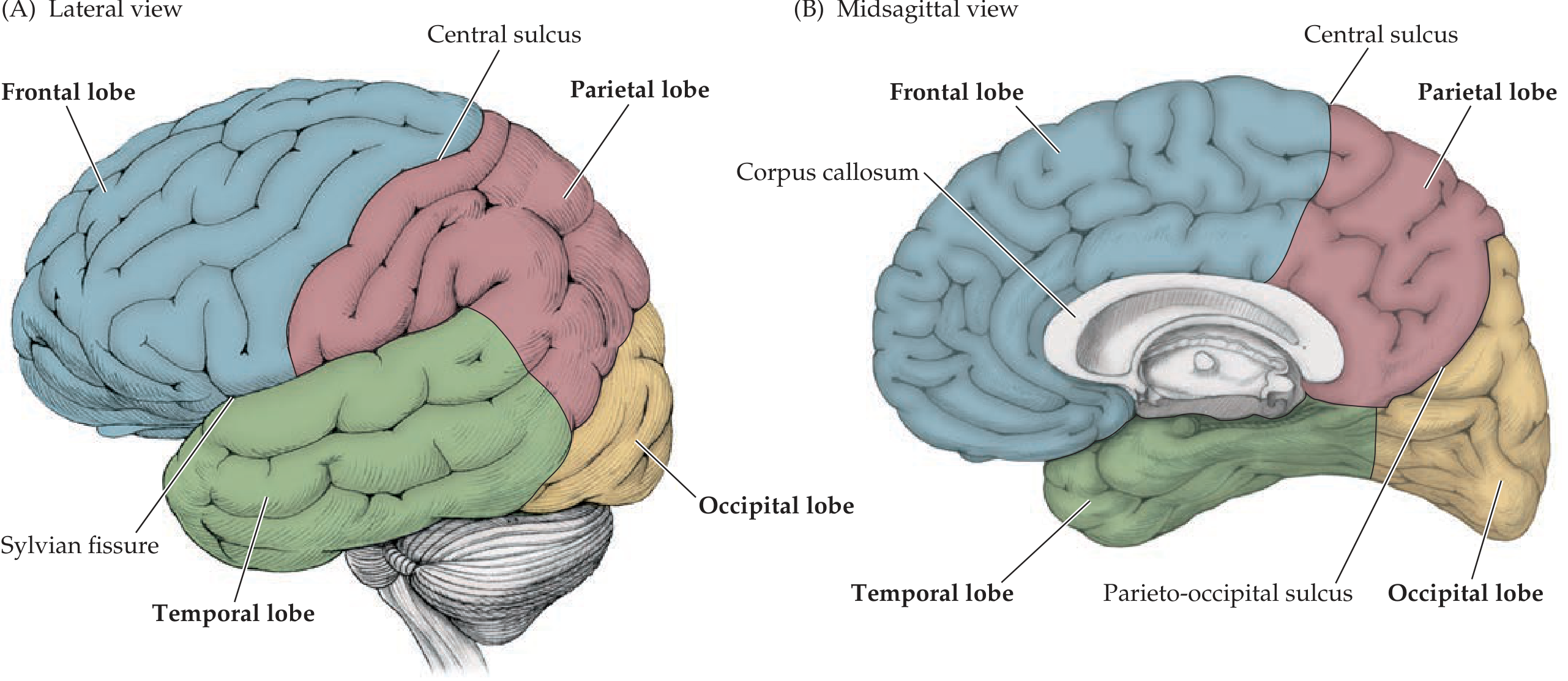
The Four Major Lobes
| Lobe | Boundaries | Key Functions |
|---|---|---|
| Frontal | Anterior to central sulcus (of Rolando); above Sylvian fissure | Voluntary movement (primary motor cortex, precentral gyrus), executive function, speech production (Broca's area, dominant hemisphere), personality |
| Parietal | Behind central sulcus; above Sylvian fissure | Somatosensory processing (postcentral gyrus), spatial awareness, reading |
| Temporal | Below Sylvian fissure | Auditory processing, language comprehension (Wernicke's area, dominant hemisphere), memory (hippocampus) |
| Occipital | Posterior; separated from parietal by parieto-occipital sulcus | Visual processing (primary visual cortex surrounds calcarine fissure) |
Two other cortical regions deserve mention:
- Insular cortex: Buried within the Sylvian fissure; involved in interoception, taste, and pain
- Corpus callosum: A C-shaped band of white matter that connects the two hemispheres - Neuroanatomy through Clinical Cases, 3rd Ed.
4. Cortical Layers and Brodmann Areas
The neocortex (90%+ of the cortex) has 6 layers (I through VI, surface to deep):
| Layer | Name | Key Connections |
|---|---|---|
| I | Molecular layer | Dendrites + axons from other layers |
| II | Small pyramidal | Cortical-cortical connections |
| III | Medium pyramidal | Cortical-cortical connections |
| IV | Granular layer | Receives thalamic inputs |
| V | Large pyramidal | Outputs to brainstem, spinal cord, basal ganglia |
| VI | Polymorphic layer | Outputs back to thalamus |
The thickness of each layer varies by function. The primary motor cortex has a thick layer V (large Betz cells sending long corticospinal axons) but a thin layer IV. The primary visual cortex has the opposite - thin V, thick IV (the "line of Gennari").
Brodmann's cytoarchitectonic map (1909) numbered 52 cortical areas based on microscopic appearance. Key areas:
| Brodmann Area | Functional Area | Location |
|---|---|---|
| 4 | Primary motor cortex | Precentral gyrus |
| 1, 2, 3 | Primary somatosensory cortex | Postcentral gyrus |
| 6 | Premotor / supplementary motor | Anterior to precentral gyrus |
| 17 | Primary visual cortex | Banks of calcarine fissure |
| 41/42 | Primary auditory cortex | Superior temporal gyrus (Heschl's gyri) |
| 44/45 | Broca's area (speech production) | Inferior frontal gyrus |
| 22 | Wernicke's area (speech comprehension) | Superior temporal gyrus |
- Neuroanatomy through Clinical Cases, 3rd Ed.
5. Subcortical Structures
Thalamus
The thalamus is the "relay station" of the brain. Nearly all sensory information (except smell) passes through it before reaching the cortex. Key nuclei:
| Nucleus | Input | Output |
|---|---|---|
| VPL (ventral posterolateral) | Somatic sensation from trunk/limbs | Somatosensory cortex |
| VPM (ventral posteromedial) | Somatic sensation from head (CN V) | Somatosensory cortex |
| Lateral geniculate body | Optic tract | Primary visual cortex |
| Medial geniculate body | Auditory (inferior colliculus) | Primary auditory cortex |
| VL posterior | Cerebellum (dentate nucleus) | Motor cortex |
| VL anterior | Globus pallidus (basal ganglia) | Supplementary motor area |
- Gray's Anatomy for Students
Basal Ganglia
The basal ganglia are deep gray matter nuclei that modulate movement (and cognition). Key components:
- Caudate + Putamen = Striatum (main input)
- Globus pallidus (internal segment = main output; external segment = indirect pathway relay)
- Substantia nigra pars compacta - dopaminergic input to striatum (lost in Parkinson's disease)
- Subthalamic nucleus - part of the indirect pathway
- The output of the basal ganglia (via globus pallidus internus) goes to the thalamus (VL/VA), which feeds back to frontal cortex
Hypothalamus
Located below the thalamus; controls autonomic functions, hormone release (via pituitary), thermoregulation, hunger, thirst, and circadian rhythms.
Limbic System
Includes the hippocampus (memory formation), amygdala (emotional processing, fear), cingulate gyrus, mammillary bodies, and related cortices. Together they form the Papez circuit for memory and emotion.
6. Brainstem
The brainstem runs from the diencephalon above to the spinal cord below, organized rostral to caudal as:
- Midbrain (mesencephalon)
- Pons
- Medulla oblongata
It houses cranial nerve nuclei III-XII (CN I and II arise from the forebrain and thalamus respectively). Key concept: The brainstem is a conduit for ALL ascending and descending tracts - even a small lesion here causes devastating deficits.
Brainstem Functions at Each Level
| Level | Key Structures | Clinical Relevance |
|---|---|---|
| Midbrain | CN III (oculomotor), IV (trochlear); substantia nigra; red nucleus; superior/inferior colliculi; cerebral peduncles | Pupillary light reflex; vertical gaze; CN III palsy with "down-and-out" eye |
| Pons | CN V (trigeminal), VI (abducens), VII (facial), VIII (vestibulocochlear); corticospinal fibers; medial lemniscus; PPRF (gaze center) | Locked-in syndrome; facial palsy; horizontal gaze palsy |
| Medulla | CN IX (glossopharyngeal), X (vagus), XI (accessory), XII (hypoglossal); pyramidal decussation; medullary cardiovascular/respiratory centers | Lateral medullary (Wallenberg) syndrome; herniation causing respiratory arrest |
The reticular formation runs through the central brainstem from medulla to midbrain. The rostral portion (pontomesencephalic) maintains consciousness via the ascending reticular activating system (ARAS). Lesions here cause coma. - Neuroanatomy through Clinical Cases, 3rd Ed.
7. Cerebellum
The cerebellum sits posteriorly, connected to the brainstem by three peduncles:
- Superior cerebellar peduncle - main OUTPUT (to contralateral red nucleus and thalamus)
- Middle cerebellar peduncle - input from contralateral pons (corticopontocerebellar pathway)
- Inferior cerebellar peduncle - input from ipsilateral spinal cord (spinocerebellar tracts) and vestibular nuclei
Functional zones:
- Vermis: axial/truncal coordination
- Paravermis (intermediate hemisphere): limb coordination
- Lateral hemisphere: motor planning, cognitive functions
The cerebellum uses the deep cerebellar nuclei (dentate, interposed, fastigial) as its output. It does not initiate movement but fine-tunes it. Cerebellar lesions cause ipsilateral ataxia (no decussation before reaching ipsilateral motor cortex).
8. Spinal Cord
The spinal cord extends from the foramen magnum to the L1-L2 vertebral level in adults (conus medullaris), where it continues as the cauda equina (nerve roots). The subarachnoid space extends to S2, providing the safe zone for lumbar puncture (usually at L3-L4 or L4-L5).
Cross-sectional anatomy:
- Gray matter (butterfly shape): anterior horn (motor neurons), posterior horn (sensory relay), lateral horn (T1-L2: sympathetic preganglionic; S2-S4: parasympathetic)
- White matter: organized into dorsal, lateral, and ventral funiculi containing ascending/descending tracts
Key Spinal Cord Tracts
| Tract | Location in Cord | Decussation Point | Carries | Clinical |
|---|---|---|---|---|
| Dorsal columns (fasciculus gracilis + cuneatus) | Posterior (ipsilateral) | At medulla (sensory decussation) | Fine touch, vibration, proprioception | Ipsilateral loss below lesion |
| Lateral corticospinal tract | Lateral column (ipsilateral below decussation) | At medullary pyramids (pyramidal decussation) | Voluntary motor commands | Ipsilateral weakness below lesion |
| Lateral spinothalamic tract | Lateral column (contralateral) | At the spinal cord level of entry (1-2 segments above) | Pain, temperature | Contralateral loss 1-2 levels below lesion |
| Anterior spinocerebellar | Anterior lateral | Double-crosses | Proprioception to cerebellum | Involved in ataxia |
Clinically important patterns:
-
Brown-Sequard syndrome (hemi-cord lesion): ipsilateral weakness + ipsilateral dorsal column loss + contralateral pain/temperature loss
-
Central cord syndrome: hands weaker than legs; bladder dysfunction
-
Anterior cord syndrome: bilateral weakness + pain/temperature loss; preserved vibration/proprioception
-
Gray's Anatomy for Students
9. Cranial Nerves Summary
| CN | Name | Type | Main Function |
|---|---|---|---|
| I | Olfactory | Sensory | Smell |
| II | Optic | Sensory | Vision |
| III | Oculomotor | Motor | Eye movement (SR, IR, MR, IO), pupillary constriction, eyelid elevation |
| IV | Trochlear | Motor | Superior oblique (intorsion, depression) |
| V | Trigeminal | Mixed | Face sensation (V1/V2/V3), mastication |
| VI | Abducens | Motor | Lateral rectus (abduction) |
| VII | Facial | Mixed | Facial expression, taste (anterior 2/3 tongue), lacrimation/salivation |
| VIII | Vestibulocochlear | Sensory | Hearing + balance |
| IX | Glossopharyngeal | Mixed | Taste (posterior 1/3), parotid salivation, carotid sinus/body |
| X | Vagus | Mixed | Parasympathetics to thorax/abdomen, phonation, swallowing |
| XI | Accessory | Motor | SCM + trapezius |
| XII | Hypoglossal | Motor | Tongue movement |
Memory rule: "Some Say Marry Money But My Brother Says Bad Business Marry Money" (S=Sensory, M=Motor, B=Both)
10. Blood Supply
Arterial Supply
The brain receives blood from two systems that unite at the Circle of Willis:
- Internal carotid arteries → Anterior circulation (ACA + MCA)
- ACA supplies medial frontal and parietal lobes (leg > arm area)
- MCA supplies lateral frontal, parietal, temporal lobes (face + arm > leg area; Broca's and Wernicke's areas)
- Vertebrobasilar system → Posterior circulation (PCA + cerebellar arteries)
- PCA supplies occipital lobe, inferior temporal, thalamus
- PICA (from vertebral) supplies lateral medulla and inferior cerebellum (Wallenberg syndrome when occluded)
- AICA, SCA supply mid/superior cerebellum
Perforating (lenticulostriate) arteries branch from the MCA to supply the basal ganglia and internal capsule - occlusion causes lacunar infarcts.
Venous Drainage
Cortical veins drain into dural venous sinuses:
-
Superior sagittal sinus (dominant) → transverse sinus → sigmoid sinus → internal jugular vein
-
Cavernous sinus receives ophthalmic veins; contains CN III, IV, V1, V2, VI and the carotid artery within its walls
-
Three key superficial veins: superficial middle cerebral vein (to cavernous sinus), superior anastomotic vein of Trolard (to superior sagittal sinus), inferior anastomotic vein of Labbé (to transverse sinus)
-
Gray's Anatomy for Students
11. Meninges and CSF
Three meningeal layers enclose both brain and spinal cord:
- Dura mater - tough outer layer; forms folds (falx cerebri, tentorium cerebelli) and venous sinuses
- Arachnoid mater - middle avascular layer; potential subdural space between dura and arachnoid
- Pia mater - inner vascular layer adherent to brain surface; forms denticulate ligaments on spinal cord
CSF is produced by the choroid plexus in the ventricles (~500 mL/day; ~150 mL circulating at any time). Flow: lateral ventricles → foramen of Monro → third ventricle → cerebral aqueduct of Sylvius → fourth ventricle → foramina of Luschka and Magendie → subarachnoid space → absorbed at arachnoid granulations into the venous sinuses.
12. Key Clinical-Anatomical Correlations
| Lesion Site | Neurological Signs |
|---|---|
| Internal capsule | Contralateral hemiplegia + hemisensory loss (all fibers tightly packed) |
| Broca's area (dominant inferior frontal) | Expressive aphasia (non-fluent; comprehension intact) |
| Wernicke's area (dominant superior temporal) | Receptive aphasia (fluent but nonsensical; poor comprehension) |
| Substantia nigra (bilateral) | Parkinson's disease (resting tremor, rigidity, bradykinesia) |
| Cerebellar hemisphere | Ipsilateral limb ataxia, intention tremor, dysmetria |
| Lateral medulla (Wallenberg) | Ipsilateral face pain/temperature loss + contralateral body pain/temperature loss, dysphagia, Horner's syndrome |
| CN III palsy | Ipsilateral ptosis, mydriasis (blown pupil), "down-and-out" eye |
| Temporal lobe (bilateral hippocampus) | Anterograde amnesia |
Key Principle: Neuroanatomy is organized around two questions: Where is the lesion? (localization) and What is the lesion? (etiology). Mastering the tracts, nuclei, and vascular territories lets you answer the first question from the patient's clinical findings alone - before any imaging. - Neuroanatomy through Clinical Cases, 3rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.