Pap smear
Reading File
Finding Sources
Searching PubMed
"cervical cancer screening" AND "Pap smear"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Here is a thorough overview of the Pap smear (Papanicolaou test) based on authoritative medical textbooks:
Pap Smear (Papanicolaou Test)
What It Is
The Pap smear is a cytologic screening test for cervical cancer introduced by George Papanicolaou in the 1920s. A spatula or brush is used to circumferentially scrape the transformation zone of the cervix - the most common site for neoplastic change. Cells are either:
- Conventional Pap smear: spread directly onto a glass slide and fixed by the examiner
- Liquid-based cytology (LBC): cells are suspended in a vial of liquid preservative, then processed in the lab to remove debris before placement on a slide
Both techniques have equivalent sensitivity and specificity. - Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed.
Why It Works
Most cervical cancers arise from precursor lesions over the course of years, giving a long window for detection. These lesions shed abnormal cells that can be identified microscopically. Virtually all (93-100%) squamous cell cervical cancers contain DNA from high-risk HPV strains. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Bethesda Classification System (Pap Smear Reporting)
Results are reported using the 2001 Bethesda System:
Squamous Cell Abnormalities
| Category | Meaning |
|---|---|
| NILM | Negative for intraepithelial lesion or malignancy (normal) |
| ASC-US | Atypical squamous cells of undetermined significance |
| ASC-H | Atypical squamous cells - cannot exclude HSIL |
| LSIL | Low-grade squamous intraepithelial lesion - equivalent to HPV changes / mild dysplasia (CIN 1) |
| HSIL | High-grade squamous intraepithelial lesion - equivalent to moderate/severe dysplasia (CIN 2, CIN 3, carcinoma in situ) |
| SCC | Squamous cell carcinoma |
Glandular Cell Abnormalities
| Category | Meaning |
|---|---|
| AGC | Atypical glandular cells (endocervical, endometrial, or NOS) |
| AGC favors neoplastic | Higher suspicion |
| AIS | Endocervical adenocarcinoma in situ |
| Adenocarcinoma | Invasive glandular cancer |
Cytologic Appearance
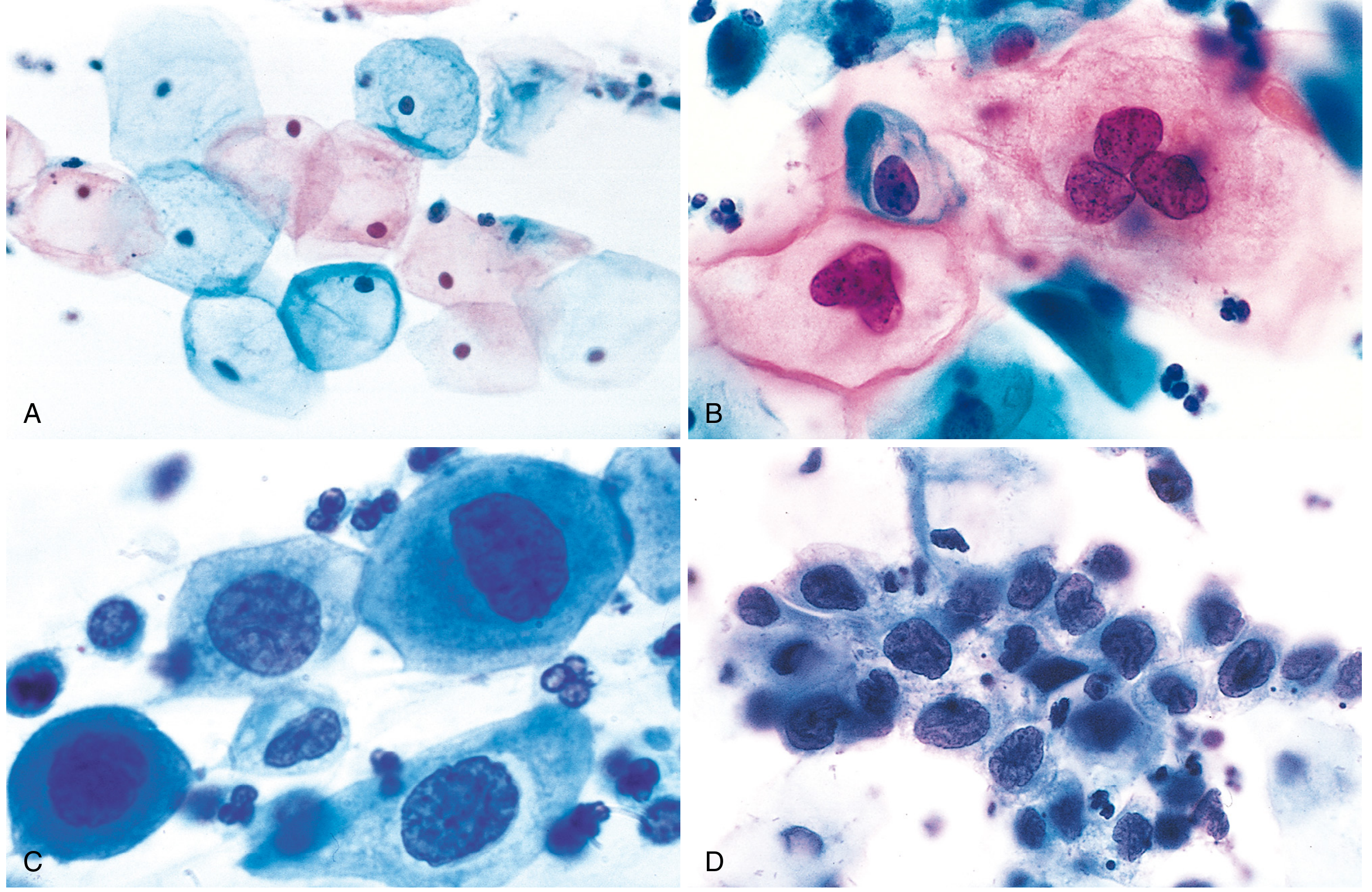
Pap smear cytology (Papanicolaou stain). (A) Normal exfoliated superficial squamous cells. (B) LSIL - koilocytes (HPV-infected cells with perinuclear halos and wrinkled, enlarged nuclei). (C) HSIL. (D) HSIL showing markedly reduced cytoplasm and high nucleus-to-cytoplasm ratio. Note how the N:C ratio progressively worsens from A to D, reflecting loss of cellular differentiation. - Robbins, Cotran & Kumar
Key cytologic features:
- Koilocytes (LSIL): perinuclear cytoplasmic clearing, wrinkled/raisinoid nuclei - hallmark of HPV infection
- HSIL: increased N:C ratio, hyperchromatic irregular nuclei, scant cytoplasm
Test Performance
| Parameter | LSIL | HSIL |
|---|---|---|
| Sensitivity | ~77% | ~56% |
| Specificity | ~80% | ~97% |
HPV testing is more sensitive but less specific than cytology for CIN 2/3. False-positive rates for HPV testing are higher in women under 35 due to the high prevalence of transient infection. - Symptom to Diagnosis
Screening Guidelines
USPSTF 2018 Recommendations (for average-risk women, no prior CIN 2+, no HIV, no DES exposure):
| Age Group | Recommendation |
|---|---|
| < 21 years | No screening |
| 21-29 years | Cytology (Pap) alone every 3 years |
| 30-65 years | Cytology alone every 3 years, OR HPV test alone every 5 years, OR co-testing (Pap + HPV) every 5 years |
| > 65 years | Discontinue if adequate recent screening and not high-risk |
| Post-hysterectomy (benign indication) | Discontinue screening |
Special Higher-Risk Groups (screen more frequently):
-
HIV-positive women: twice in year 1, then annually
-
Immunosuppressed patients
-
DES daughters
-
Prior CIN 2 or greater: annually for 20 years
-
Berek & Novak's Gynecology; ACOG guidelines
HPV Co-testing and Primary HPV Screening
After age 30, HPV DNA testing can be added to cytology (co-test) or used alone as primary screening. Women who are cytology-negative but HPV-positive for high-risk strains should have repeat cytology every 6-12 months. HPV testing is not recommended under age 30 due to high rates of transient HPV infection in younger women. - Robbins, Cotran & Kumar
Abnormal Result Management
When a Pap smear is abnormal:
- Colposcopy - magnified examination of the cervix after application of acetic acid (highlights abnormal areas as "aceto-white" lesions)
- Directed biopsy of any abnormal areas
- LSIL on biopsy: can be followed conservatively or treated with local ablation (cryotherapy)
- HSIL on biopsy: treated with cervical conization (LEEP or cold knife)
Impact and Importance
Since cervical cytology screening was introduced in the 1950s, cervical cancer deaths in the United States have declined by 70%. Observational studies show a 60-90% reduction in cervical cancer incidence and 20-60% reduction in mortality with screening. Many cervical cancers in the US occur in women who have never been screened. - Histology: A Text and Atlas; Symptom to Diagnosis
HPV Vaccination (Complementary Prevention)
HPV vaccination is recommended for all children and adults aged 9-26 years, and for selected adults aged 27-45 years. The current US vaccine covers 9 HPV types (including the high-risk types 16 and 18 responsible for most cervical cancers). Vaccination does not eliminate the need for Pap screening. - Robbins, Cotran & Kumar
Recent evidence (2026): A systematic review (PMID 42142346, Acta Cytologica, May 2026) evaluated liquid-based cytology vs. conventional cytology in cervical cancer screening - this is the most current comparative data on Pap smear techniques.
Haematological changes during pregnancy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hematological changes" AND pregnancy
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Here is a comprehensive review of haematological changes during pregnancy, drawn from multiple authoritative textbooks:
Haematological Changes During Pregnancy
1. Blood Volume
| Parameter | Change | Timing |
|---|---|---|
| Total blood volume | +35-50% | Peaks ~32-34 weeks |
| Plasma volume | +45-55% (1200-1600 mL above baseline) | Begins at 6-8 weeks, peaks at 32 weeks |
| Red cell mass | +20-30% (250-450 mL) | Gradual rise throughout |
Plasma volume expansion begins as early as 6-8 weeks of gestation, reaches a maximum of 4700-5200 mL at 32 weeks. The mechanism is thought to involve nitric oxide-mediated vasodilation, which activates the renin-angiotensin-aldosterone system, driving sodium and water retention. Importantly, plasma volume expansion exceeds the rise in red cell mass - this disproportionate increase is the basis of physiological anaemia of pregnancy. - Creasy & Resnik's Maternal-Fetal Medicine
2. Red Blood Cells and Haemoglobin
Physiological Anaemia of Pregnancy
Because plasma volume increases more than red cell mass, haemodilution occurs:
- Haemoglobin falls to a normal nadir of around 11.6 g/dL at term (Hb < 11 g/dL at any point is pathological)
- Haematocrit decreases, reaching its lowest point in the mid-third trimester
- This is not a pathological state - overall oxygen delivery is maintained by the concurrent rise in cardiac output (+30-50%)
The dilutional effect also reduces blood viscosity, which may protect against thromboembolism and improve intervillous placental perfusion. - Miller's Anesthesia, 10e; Creasy & Resnik
Erythropoiesis
- Increased red cell production is driven by placental chorionic somatomammotropin, progesterone, and possibly prolactin
- These hormones stimulate erythropoietin release, increasing erythropoiesis
- 2,3-Diphosphoglycerate (2,3-DPG) in erythrocytes increases, which shifts the oxygen dissociation curve to the right, reducing maternal haemoglobin's oxygen affinity and facilitating oxygen transfer to the fetus
Iron Demands
Pregnancy creates a total iron requirement of approximately ~1000 mg:
| Use | Amount |
|---|---|
| Increased erythropoiesis (maternal) | ~500 mg |
| Fetal iron transfer | ~300 mg |
| Normal daily losses | ~200 mg |
This is why iron deficiency is the most common cause of anaemia in pregnancy. - Creasy & Resnik
Blood Loss Compensation at Delivery
The expanded blood volume (~1000-1500 mL above baseline at term) provides a buffer against:
- Vaginal delivery: estimated blood loss 300-500 mL
- Caesarean section: estimated blood loss 800-1000 mL
- After delivery, uterine contraction provides an autotransfusion of >500 mL, which partially offsets delivery losses. - Miller's Anesthesia
3. White Blood Cells (Leukocytes)
- Leukocytosis (WBC > 10,000/mm³) is normal and physiological in pregnancy - it is not a sign of infection
- The normal WBC range in pregnancy extends to 13,000/mm³
- WBC rises further during labour, with the degree of rise proportional to the duration of elapsed labour
- After delivery, WBC may fall in the first postpartum week but may take weeks to months to return to pre-pregnancy values
- This physiological leukocytosis is predominantly due to increased neutrophil count (neutrophilia)
- Mild leukocytosis up to 16,900/μL can be seen in normal pregnancy - Creasy & Resnik; Miller's Anesthesia
Clinical note: The normally elevated WBC in pregnancy makes interpretation of leucocytosis challenging. A high WBC in a pregnant patient must be interpreted in context, as it may represent normal physiology rather than infection or inflammation.
4. Platelets
-
Platelet count usually remains normal but may decrease by ~10% near term due to haemodilution and increased platelet turnover
-
Up to 8% of otherwise healthy pregnant women have a platelet count < 150,000/mm³ - this is called gestational thrombocytopenia
-
Gestational thrombocytopenia:
- Is a diagnosis of exclusion
- Platelet count typically does not fall below 70,000/mm³
- Is not associated with abnormal bleeding
- Resolves spontaneously after delivery
- Must be distinguished from ITP and HELLP syndrome
-
Miller's Anesthesia, 10e; Tietz Textbook of Laboratory Medicine
5. Coagulation System - Hypercoagulable State
Pregnancy induces a pro-coagulant state to protect against haemorrhage at delivery. Changes include:
Clotting Factors
| Factor | Change |
|---|---|
| Fibrinogen (Factor I) | +65% (from ~275 to ~450 mg/dL) |
| Factor VII | Marked increase |
| Factor VIII | Increases |
| Factor IX | Increases |
| Factor X | Increases |
| Factors II, V | Unchanged |
| Factor XI | Slight decrease |
| Factor XIII | Slight decrease |
| Prothrombin | Unchanged |
Anticoagulant Proteins
| Protein | Change |
|---|---|
| Antithrombin III | Decreased |
| Protein S | Decreased |
| Protein C | Unchanged |
Lab Tests
- PT and PTT both shorten by approximately 20% (reflecting a hypercoagulable state)
- ESR rises significantly (mainly due to the increase in fibrinogen)
- Thromboelastography (TEG/ROTEM) at term shows decreased clot formation time (R), decreased K time, increased α angle, and increased maximum amplitude (MA) - all reflecting enhanced clot formation. These changes begin as early as the first trimester. - Tietz Laboratory Medicine; Miller's Anesthesia
Overall Risk
Despite the dilutional effect on platelets, the net result of all coagulation changes is an approximately 5-fold increase in thromboembolic risk compared to non-pregnant women. - Tietz Textbook of Laboratory Medicine
6. Summary Table
| Haematological Parameter | Change in Pregnancy |
|---|---|
| Plasma volume | +45-55% |
| Red cell mass | +20-30% |
| Haemoglobin | -20% (nadir ~11.6 g/dL) |
| Haematocrit | Falls (lowest at mid-third trimester) |
| WBC | Increases to 13,000/mm³ (up to 16,900 in late pregnancy) |
| Platelets | Unchanged or slight fall (-10%); gestational thrombocytopenia in 8% |
| Fibrinogen | +65% |
| Factors VII, VIII, IX, X | All increased |
| Factors XI, XIII | Slight decrease |
| Antithrombin III | Decreased |
| Protein S | Decreased |
| PT/PTT | Shortened (~20%) |
| 2,3-DPG | Increased (right shift of O₂ curve) |
| ESR | Markedly elevated |
| VTE risk | ~5x above non-pregnant baseline |
- Morgan & Mikhail's Clinical Anesthesiology 7e; Creasy & Resnik's Maternal-Fetal Medicine; Miller's Anesthesia 10e; Tietz Laboratory Medicine 7e
Recent evidence (2024): A narrative review (PMID 39280542, Cureus, 2024) assessed the impact of these haematological changes on maternal and fetal outcomes, confirming that pathological deviations from these physiological norms - particularly severe anaemia - are associated with increased maternal and fetal mortality.
This is a shared conversation. Sign in to Orris to start your own chat.