How does pulse oximetry works
Reading File
Finding Sources
Searching the Web
pulse oximetry mechanism how it works beer-lambert law
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-illustrated answer. Here it is:
How Pulse Oximetry Works
The Core Principle: Beer-Lambert Law
Pulse oximetry is rooted in the Beer-Lambert law, which states that the concentration of an unknown solute in a solution can be determined by measuring how much light it absorbs. Applied to blood, the law means that the intensity of light transmitted through a vascular bed decreases exponentially as a function of hemoglobin concentration and the path length the light travels through tissue. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
The key insight is that oxyhemoglobin (O2Hb) and deoxyhemoglobin (Hb) absorb light differently depending on wavelength:
- At 660 nm (red light): deoxyhemoglobin absorbs significantly more than oxyhemoglobin (deoxygenated blood looks darker/more red-absorbing)
- At 940 nm (near-infrared light): oxyhemoglobin absorbs significantly more than deoxyhemoglobin
Two LEDs in the probe sequentially flash at these two wavelengths. A photodetector on the opposite side (transmission oximetry - e.g., fingertip) measures how much light passes through. - Barash Clinical Anesthesia, 9e
Isolating the Arterial Signal: AC vs. DC
The biggest challenge is that light also passes through skin, bone, connective tissue, and venous blood - none of which you want to measure. The device solves this elegantly using pulsatility:
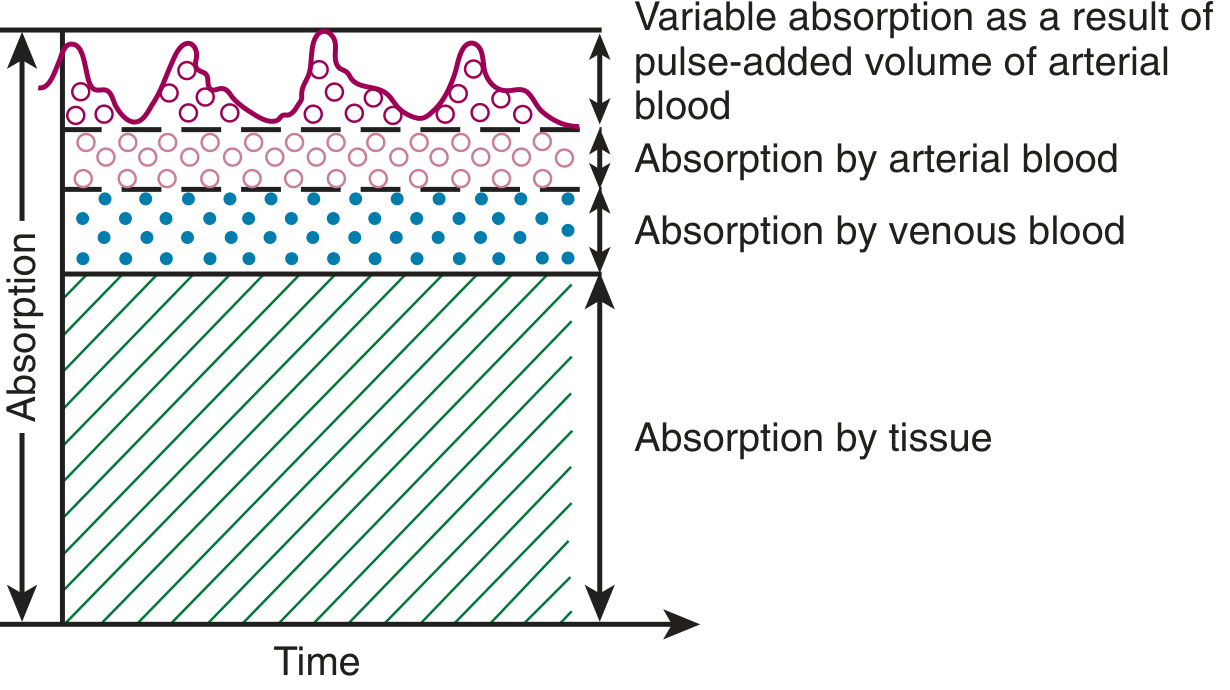
As the diagram shows, total light absorption has two components:
- DC (direct current) component - constant, non-pulsatile absorption from tissue, venous blood, and resting arterial blood
- AC (alternating current) component - the small, rhythmically pulsing increase in absorption that occurs with each heartbeat as a bolus of arterial blood enters the tissue bed
The pulse oximeter uses only the AC component and divides it by the DC baseline at each wavelength. This strips out everything except the arterial blood signal. - Miller's Anesthesia, 10e
The R Value Calculation
The device computes a ratio R:
R = (AC₆₆₀ / DC₆₆₀) ÷ (AC₉₄₀ / DC₉₄₀)
This ratio is then matched against an internally stored empirical calibration curve (derived by having healthy volunteers breathe progressively hypoxic gas mixtures to achieve saturations between 70-100%) to read out SpO₂.
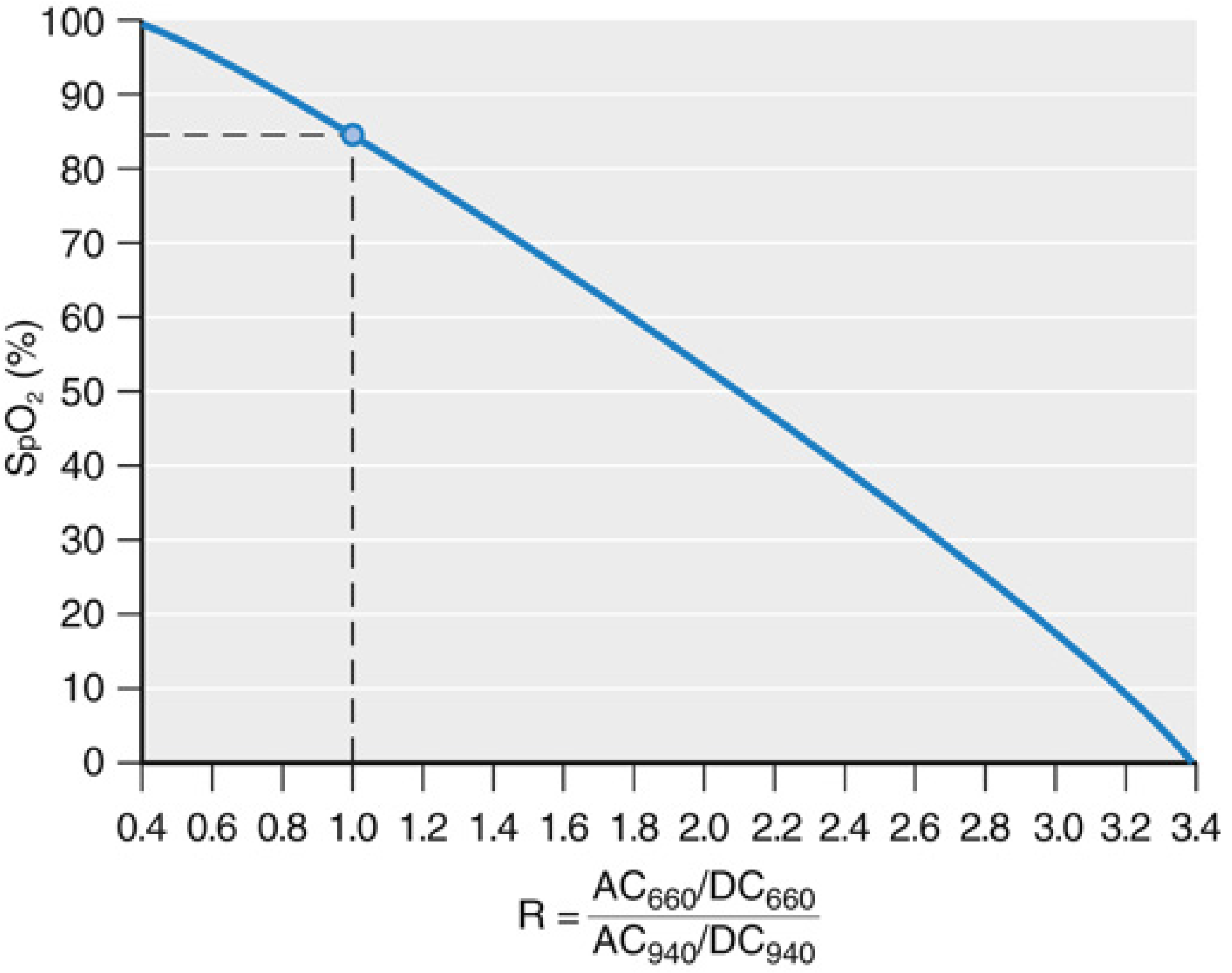
As seen in the graph, higher R values (more red-light absorption relative to infrared) correspond to lower SpO₂. At R ≈ 1.0, SpO₂ is approximately 85%. - Miller's Anesthesia, 10e
Functional vs. Fractional Saturation
Standard pulse oximeters use only 2 wavelengths, so they can only distinguish 2 substances. They report functional saturation:
SpO₂ = HbO₂ / (HbO₂ + Hb) × 100%
This is not the same as fractional saturation (SaO₂) measured by a lab co-oximeter, which uses 4+ wavelengths to also account for carboxyhemoglobin (COHb), methemoglobin (MetHb), and other species:
SaO₂ = HbO₂ / (HbO₂ + Hb + COHb + MetHb) × 100%
- Barash Clinical Anesthesia, 9e | Roberts and Hedges' Emergency Medicine
Transmission vs. Reflectance Oximetry
| Type | Configuration | Common location |
|---|---|---|
| Transmission | Emitter and detector on opposite sides | Fingertip, toe, earlobe |
| Reflectance | Emitter and detector on same side | Forehead, chest |
Reflectance oximetry is gaining popularity because it can be placed over a wider range of vascular beds. - Miller's Anesthesia, 10e
Photoplethysmography (Bonus Feature)
Because the AC signal represents the volume pulse of blood, the pulse oximeter waveform is also a photoplethysmograph (PPG). The shape and amplitude of this waveform can reflect changes in intravascular volume, vessel wall distensibility, and cardiac output - making it useful beyond just SpO₂.
Limitations and Sources of Error
| Problem | Effect |
|---|---|
| Carboxyhemoglobin (CO poisoning) | COHb absorbs at 660 nm similarly to O2Hb - SpO₂ reads falsely high (at 70% COHb, SpO₂ may still read 90%) |
| Methemoglobin | MetHb absorbs red and infrared equally (1:1 ratio) - SpO₂ is driven toward ~85% regardless of true saturation |
| Poor perfusion / low pulse pressure | Weak or absent AC signal - unreliable or no reading |
| Dark skin pigmentation | Documented to cause "occult hypoxemia" - in one large dataset, prevalence was 12-17% in Black patients vs. 3-6% in White patients with SpO₂ 92-96% masking true SaO₂ <88% |
| Nail polish (blue/green) | Can interfere with light transmission |
| Motion artifact | Spurious AC signals |
| SpO₂ <70% | Below calibration range - values are unreliable |
| Insensitive to ventilation | A patient with normal SpO₂ may still be hypoventilating and hypercapnic |
- Goldman-Cecil Medicine | Barash Clinical Anesthesia, 9e
Accuracy
The FDA requires root mean square error ≤3.0% for transmission sensors (fingertip, earlobe) and ≤3.5% for reflectance sensors, over the range of 70-100% SpO₂. Most devices achieve ±2-3%. The device cannot reliably measure below 70% SpO₂ since the calibration curves don't extend there. - Miller's Anesthesia, 10e | Goldman-Cecil Medicine
In summary: pulse oximetry works by shining two wavelengths of light through tissue, isolating the pulsatile arterial component of light absorption, computing the ratio (R) of absorption changes at 660 nm and 940 nm, and mapping that ratio to SpO₂ via a pre-loaded calibration curve. The physics (Beer-Lambert law) + the pulsatile isolation trick + the empirical calibration is what makes it work - and also explains each of its clinical failure modes.
This is a shared conversation. Sign in to Orris to start your own chat.