
IMG_9560.jpeg
Explain uses of epidemiology in detail and in simple language use notes as a primary source and use park if needed to explain any topic
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have all 7 uses from both your notes and Park's. Here is the complete, detailed, simple-language explanation:
14 - Uses of Epidemiology
(Based on your notes + Park's Textbook of Preventive and Social Medicine)
Epidemiology is not just about finding the cause of disease. Morris (1975) identified 7 distinct uses of epidemiology. Five of these go well beyond just searching for causes - they bring epidemiology right into the everyday concerns of modern medicine. Think of epidemiology as both a detective (finding causes) and a planner (organizing health services).
1. To Study the Rise and Fall of Disease in the Population (Historical Study)
Simple idea: Look at the past to understand the present and predict the future.
The health and disease pattern in a community is never constant - it keeps changing over time. Epidemiology tracks these changes.
Examples from Park's:
- Coronary heart disease (CHD) was first recognized as an "epidemic" through epidemiology.
- Later, accidents, cancer, and diabetes were also found to be behaving like epidemics.
- Old diseases like smallpox were conquered, but new ones like AIDS, Legionnaires' disease, and Lassa fever appeared - epidemiology played a major role in identifying these.
What your notes say: Study of disease profiles and time trends in human population.
Why it matters: By studying trends over time, we can make projections into the future and identify emerging health problems before they become catastrophic.
2. Community Diagnosis
Simple idea: Just like a doctor diagnoses a sick patient, epidemiology "diagnoses" the health of an entire community.
Community diagnosis means identifying and quantifying (measuring) health problems in a community in terms of:
- Mortality rates (death rates)
- Morbidity rates (illness rates)
- Ratios and comparisons between groups
What your notes say: Identification and quantification of health problems in a community in terms of mortality and morbidity rates and ratios.
Three key purposes from Park's:
- Set priorities - knowing which diseases are most common helps decide where to focus resources.
- Benchmark - the measurements become a yardstick to evaluate health services later.
- New knowledge - reveals new information about disease distribution, causes, and prevention.
Community diagnosis also includes understanding the social, cultural, and environmental background of the community. That is why epidemiology is called the "diagnostic tool of community medicine."
3. Planning and Evaluation of Health Services
Simple idea: Use disease data to plan what health services a community needs, and then check if those services actually worked.
Planning (from Park's):
Epidemiological information about how diseases are distributed over time and place provides the fundamental basis for:
- Planning the number of hospital beds needed for specific diseases.
- Planning immunization campaigns and screening programs.
- Planning sanitary services and health manpower.
Without this data, countries have wasted resources - for example, too many hospitals were built in developing countries without knowing what diseases actually existed in those communities.
Evaluation (from Park's):
Any measure taken to control disease must be evaluated afterward:
- Did the hepatitis vaccine reduce disease? By how much?
- Was the cost worth it? (Cost-effectiveness studies)
- The development of randomized controlled trials (RCTs) has made evaluation on a firm scientific basis possible.
What your notes say: Epidemiological information about the distribution of health problems over time and place provides the fundamental basis for planning and developing the health services and for assessing the impact of these services.
4. Evaluation of Individual Risks
Simple idea: Tells us how likely a specific person or group is to get a disease, based on their characteristics.
Epidemiologists calculate two important types of risk:
| Risk Type | What it means | Example |
|---|---|---|
| Relative Risk | How many times more likely is a person with factor X to get disease vs. without | Smokers are X times more likely to get lung cancer |
| Attributable Risk | How much of the disease is caused by the factor | How many lung cancer cases are directly due to smoking |
Examples from Park's:
- Risk of bearing a child with Down syndrome (mongolism) - related to mother's age.
- Risk of hereditary disorders.
- Risk assessment comparing smokers vs. non-smokers for cancer and CHD.
What your notes say: Epidemiologists calculate relative risk and attributable risk for a factor related to be a cause of the disease.
5. Syndrome Identification
Simple idea: Epidemiology helps confirm whether a group of symptoms/signs that doctors observe together really do belong together as a recognized syndrome.
What your notes say: Medical syndromes are identified by observing frequently associated findings in individual patients.
From Park's - key insight:
- About 3000 syndromes are described in pediatric literature, but a primary (root) defect is known in only about 20% of them.
- Epidemiology can define, refine, and even correct misconceptions about syndromes by studying large groups of people.
Examples:
- Gastric vs. Duodenal ulcer: Before 1920, the two types of peptic ulcer were not well differentiated. Epidemiological data showed a "poverty gradient" in gastric ulcer but not in duodenal ulcer - this helped distinguish the two as separate diseases.
- Patterson-Kelly syndrome (association between difficulty swallowing and iron-deficiency anemia): when tested by epidemiological methods, the association was not confirmed - correcting a clinical misconception.
- Epidemiology has also explored whether distinct subtypes of essential hypertension exist based on plasma renin levels.
6. Completing the Natural History of Disease
Simple idea: A hospital doctor only sees sick patients who came to hospital. Epidemiology studies everyone in the community - the mild cases, the severe ones, those who never reached hospital - giving a much fuller picture of how a disease actually behaves.
What your notes say: Epidemiologists by studying disease patterns in the community in relation to agent, host, and environmental factors are in a better position to fill up the gaps in the natural history of disease.
Classic example from Park's:
- Epidemiology revealed that one-third to two-thirds of all deaths from ischemic heart disease are sudden (occurring within less than one hour of onset).
- Hospital studies could never have discovered this because most of these victims never reached the hospital.
- This finding gave a huge push to the development of intensive coronary care units (ICUs).
The epidemiologist studies all cases in a defined population - regardless of severity or whether they sought medical care. This gives the broadest possible perspective of a disease.
7. Searching for Causes and Risk Factors
Simple idea: Epidemiology links diseases to interpopulation differences - age, sex, diet, occupation, habits - to find out what is causing the disease.
What your notes say: Epidemiology, by relating disease to interpopulation differences and other attributes, tries to identify the causes of disease.
Examples from Park's:
- Rubella (German measles) causes congenital defects in newborns.
- Thalidomide is a teratogenic drug (causes birth defects).
- Cigarette smoking causes lung cancer.
- Exposure of premature babies to high oxygen causes retrolental fibroplasia (a blinding eye condition).
For chronic diseases (e.g., heart disease, diabetes, cancer):
Finding a single cause is rarely possible. Instead, epidemiology introduced the powerful concept of "risk factors" - multiple contributing factors that increase the probability of disease. This concept completely transformed how we study and prevent chronic diseases.
Quick Summary Table
| # | Use | Core Idea |
|---|---|---|
| 1 | Rise and fall of disease | Track disease trends over time to predict future problems |
| 2 | Community diagnosis | Measure and quantify health problems in a population |
| 3 | Planning and evaluation | Plan health services based on data; evaluate if they work |
| 4 | Individual risk evaluation | Calculate relative risk and attributable risk for individuals |
| 5 | Syndrome identification | Confirm or refute clinical syndromes using population studies |
| 6 | Natural history of disease | Fill the gaps in disease knowledge by studying the whole community |
| 7 | Causes and risk factors | Link disease to exposures, habits, and attributes to find causes |
Source: Park's Textbook of Preventive and Social Medicine (Morris, 1975 - 7 Uses of Epidemiology), Cross-referenced with your notes (Chapter 14, Topic 4 - Epidemiology, Disease Transmission and Immunization).

image.jpg
Explain isolation and quarantine in detail and in simple language
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
I now have everything from Park's. Here is the complete, detailed, simple-language explanation of both topics:
7 - Isolation
What is Isolation?
Simple definition: Isolation means separating a sick (infected) person from healthy people, for as long as they can spread the disease, so that the infection does not pass from them to others.
The official definition from Park's:
"Separation, for the period of communicability of infected persons or animals from others, in such places and under such conditions as to prevent or limit the direct or indirect transmission of the infectious agent from those infected to those who are susceptible."
Key point: Isolation is the oldest communicable disease control measure.
Think of it like this: If you have a contagious cold and you stay in your room so your family doesn't catch it - that is isolation in the simplest sense.
Purpose of Isolation
The goal is to protect the community by stopping the transfer of infection from the reservoir (the sick person) to susceptible (not-yet-immune) healthy people.
Types of Isolation
There are 4 types, and the right type is chosen based on how the disease spreads and how severe it is:
| Type | What it means | When used |
|---|---|---|
| 1. Standard Isolation | Basic precautions for most infections (hand hygiene, masks, gloves) | Most routine infectious diseases |
| 2. Strict Isolation | Maximum separation - private room, full PPE (gown, mask, gloves), limited visitors | Highly contagious diseases - e.g., pneumonic plague, severe VHF (Ebola) |
| 3. Protective Isolation | Protects the patient from the environment, not the other way around | Immunocompromised patients (e.g., post-chemotherapy, bone marrow transplant) who are at risk from others' germs |
| 4. High Security Isolation | Reserved for extremely dangerous diseases with no cure/vaccine; highest level facilities | Viral hemorrhagic fevers, novel pathogens |
Note: For each patient, the relative risks to the patient and to others should both be assessed before choosing the type. Hospital isolation is better than home isolation wherever possible. Today, isolation is only recommended when the risk of transmission is exceptionally serious.
Diseases Where Isolation is Needed
From your notes (diseases requiring isolation):
- Diphtheria
- Tuberculosis (TB)
- Herpes zoster (chickenpox/shingles)
- Cholera
- Staphylococcal pharyngitis
- Polio
- Leprosy
- Pneumonic plague
Periods of Isolation (How Long?)
The duration depends on the disease's communicability period and whether treatment can cut it short:
| Disease | Isolation Period |
|---|---|
| Measles | From onset of catarrhal (runny nose/cough) stage through the 3rd day of rash |
| Cholera and Diphtheria | 3 days after tetracycline started, until culture is negative |
| Influenza | 3 days after onset |
| Polio | 2 weeks (adults) and 6 weeks (children) |
| TB | Until 3 weeks of chemotherapy completed |
| Chickenpox and Herpes zoster | Up to 6 days after onset of rash (until all lesions crusted) |
Isolation by Ring Immunization
Sometimes, instead of physically isolating the sick person, we surround them with immune people. This creates a protective "ring" or barrier of immunity through which the infection cannot spread.
How it works:
Encircling the infected person with a barrier of immune persons through whom the infection is unable to spread.
Real-world examples:
- This method was used to eradicate smallpox worldwide in the 1960s-70s.
- It is being applied for measles control and eradication in North America.
When Isolation Fails
Isolation does not work well in all diseases. It has failed as a control measure in:
- Tuberculosis (TB)
- Leprosy
- Sexually Transmitted Diseases (STDs)
Why does it fail?
- These diseases have large numbers of subclinical (no-symptom) cases.
- People spread the disease before they are even diagnosed.
- High carrier rates make physical isolation impractical.
What replaced physical isolation in these diseases?
- Chemical Isolation - This means rapidly treating cases in their own homes and making them non-infectious as quickly as possible using drugs. The person stays home but is rendered non-contagious by treatment.
Limitations of Isolation (Summary)
- Cases are usually diagnosed only after the disease has already spread widely.
- In diseases with large subclinical components (e.g., polio, Hepatitis A), even rigid isolation won't stop spread.
- Highly infectious diseases spread before diagnosis (e.g., mumps).
- Isolation may give a false sense of security.
Because of all these limitations, modern disease control replaces isolation with surveillance in most situations. Isolation is now only justified when the risk of transmission is exceptionally serious.
8 - Quarantine
What is Quarantine?
Simple definition: Quarantine means restricting the movement of HEALTHY people who have been exposed to a communicable disease, for a period no longer than the disease's longest incubation period, so they do not spread it if they turn out to be infected.
The official definition from Park's:
"The limitation of freedom of movement of such well persons or domestic animals exposed to communicable disease for a period of time not longer than the longest usual incubation period of the disease, in such manner as to prevent effective contact with those not so exposed."
KEY DIFFERENCE from Isolation:
| Feature | Isolation | Quarantine |
|---|---|---|
| Who is it applied to? | Sick / infected person | Healthy person exposed to disease |
| Purpose | Stop sick person spreading disease | Prevent potentially exposed person from spreading disease if they develop it |
| Duration | Period of communicability | Longest incubation period of the disease |
Think of it like this: During COVID-19, if someone tested positive - they were isolated. If someone was a close contact but had no symptoms yet - they were quarantined for 14 days (the incubation period).
Where is Quarantine Applied?
Quarantine is applied to:
- Ships
- Aircrafts
- Trains
- Road vehicles
- Containers
...to prevent the spread of disease, reservoirs, or vectors of disease across borders.
Types of Quarantine
Quarantine has 3 components:
1. Absolute Quarantine
- This is the classical, complete definition above.
- Complete limitation of the freedom of movement of exposed persons for the full incubation period of the disease.
- Example: Keeping all ship passengers confined for the full incubation period of a disease suspected on board.
2. Modified Quarantine
- A selective, partial limitation of freedom of movement.
- Not everyone is fully restricted - only specific activities or settings are limited.
- Example: Excluding children from school after exposure to measles or chickenpox, but allowing adults to continue working (since the risk in adults may be different).
3. Segregation
- Defined as: "The separation for special consideration, control or observation of some part of a group of persons from the others, to facilitate control of a communicable disease."
- Example: Removing susceptible (non-immune) children to homes of immune persons during an outbreak so the susceptibles are protected.
- The group being separated here is not necessarily exposed - they are simply susceptible (at risk because they lack immunity).
Current Status of Quarantine
"Quarantine as a method of disease control has become outdated and has been replaced by Active Surveillance."
- Park's Textbook
Why has it become outdated?
- Better, faster techniques of early diagnosis are now available.
- Effective treatment can render people non-infectious quickly.
- Modern surveillance systems (active case finding, contact tracing) are far more efficient.
- Strict quarantine was very disruptive socially and economically.
Summary Comparison Table
| Feature | Isolation | Quarantine |
|---|---|---|
| Applied to | Infected/sick person | Healthy exposed person |
| Goal | Prevent spread from sick to healthy | Prevent spread if exposed person develops disease |
| Duration | Period of communicability | Longest incubation period |
| Types | Standard, Strict, Protective, High security | Absolute, Modified, Segregation |
| Current status | Used only for exceptionally serious infections | Largely replaced by active surveillance |
| Alternative | Chemical isolation (rapid treatment) | Active surveillance, contact tracing |
Source: Park's Textbook of Preventive and Social Medicine, pp. 104, 136-137 (Sections 4 and 6 - Control of Reservoir). Cross-referenced with your notes (Topics 7 and 8, Chapter on Disease Transmission and Immunization).

image.jpg
Explain this in detail and simple language
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I have everything needed including the actual diagrams from Park's. Here is the complete, simple-language explanation:
Cold Chain Monitoring - Shake Test & Vaccine Vial Monitor (VVM)
(Page 74 of your notes - Cold Chain topic)
Background: Why Do We Monitor Vaccines?
Vaccines are delicate. They can be damaged by two things:
- Too much heat - kills the live organisms in the vaccine
- Freezing - damages certain vaccines (especially those containing aluminium adjuvants like DTP, Hepatitis B, TT)
The tools we use to detect this damage are:
- The Shake Test - detects freeze damage
- The Vaccine Vial Monitor (VVM) - detects heat damage
Part A: Shake Test
What is the Shake Test?
A simple test to find out whether a freeze-sensitive vaccine has been accidentally frozen (exposed to temperature below 0°C) and is therefore damaged and unsafe to use.
Why does freezing damage vaccines?
From your notes:
"When a vaccine freezes, its alum (aluminium) content gets loose and sediments faster than a non-frozen vaccine."
Simple explanation: Many vaccines (like DTP, Hepatitis B, TT) contain aluminium salts as an adjuvant (a substance that boosts the immune response). When the vaccine freezes, these aluminium particles clump together and break apart - forming larger, heavier particles. After thawing, these damaged particles settle to the bottom (sediment) much faster. A normal, never-frozen vaccine settles slowly.
How to Do the Shake Test - Step by Step
You need TWO vials:
| Vial | What it is | How to prepare |
|---|---|---|
| Control Vial (Frozen Vial) | A known-damaged vaccine - your reference for "definitely damaged" | Take a vial of the SAME vaccine, SAME manufacturer, SAME batch number. Freeze it solid at -20°C overnight. Let it thaw completely. Do NOT heat it. |
| Suspect Vial (Test Vial) | The vaccine you are unsure about - the one you want to test | Take the vaccine vial you suspect may have been frozen |
Procedure:
- Hold both vials (control + suspect) together between thumb and forefinger
- Shake both vigorously for 10-15 seconds (your notes say 5-15 mins for observation, Park's says 10-15 seconds shaking)
- Place both vials side by side on a flat surface
- Observe for 30 minutes - watch how the sediment settles in each vial
How to Read the Shake Test Result
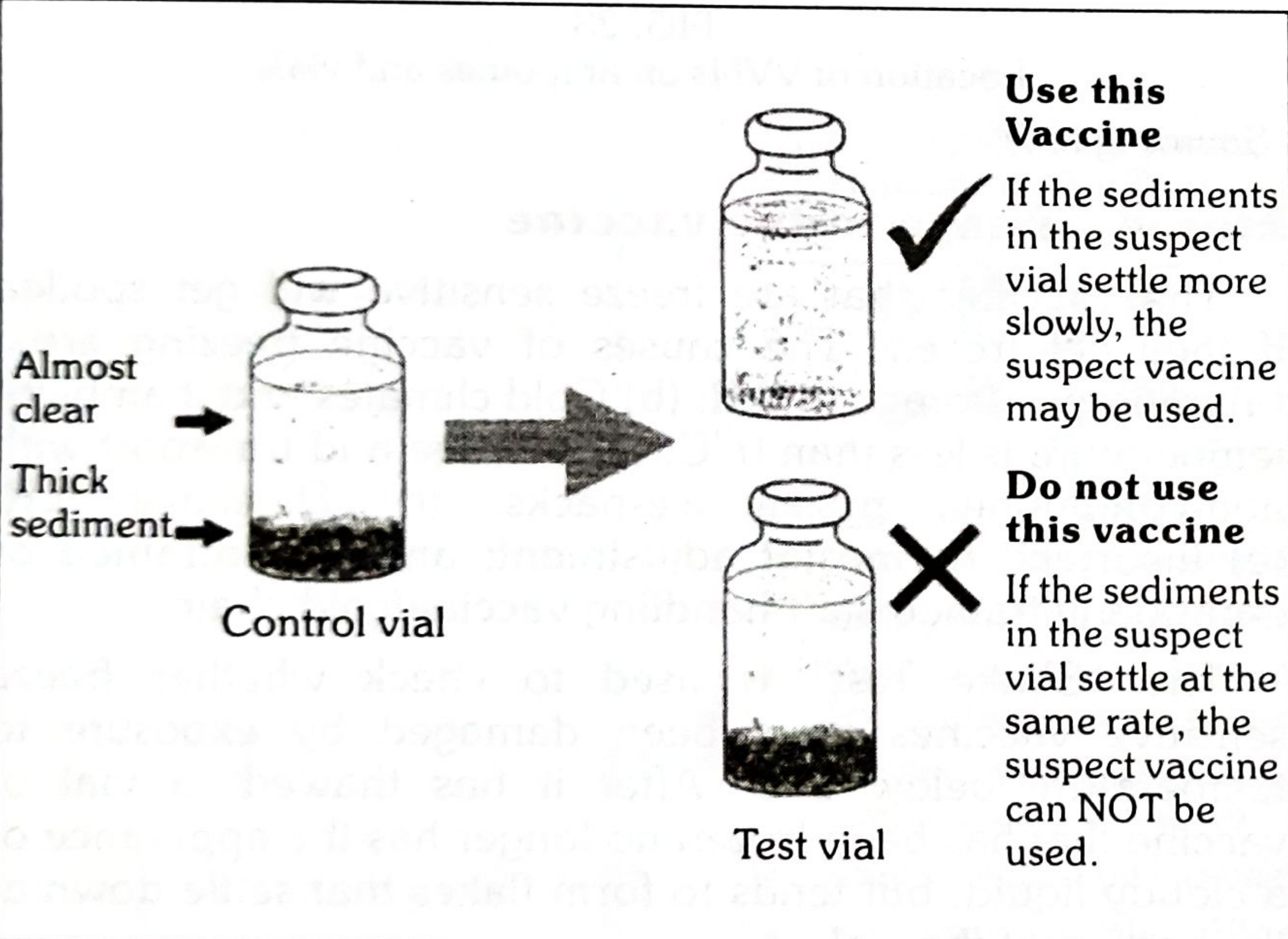
| What you see | What it means | Decision |
|---|---|---|
| Suspect vial sediments SLOWER than control vial | Vaccine was NOT frozen - it is intact | ✅ USE IT - vaccine is safe |
| Suspect vial sediments at the SAME RATE as control vial | Vaccine WAS frozen and damaged | ❌ DO NOT USE - notify supervisor |
| Suspect vial sediments FASTER than control vial | Vaccine WAS frozen and severely damaged | ❌ DO NOT USE - notify supervisor |
Simple memory trick:
- Control vial = known damaged = settles fast (thick sediment at bottom, almost clear above)
- If your test vial settles like the damaged one = it IS damaged = throw it out
- If your test vial settles slower = it was never frozen = still good
Part B: Vaccine Vial Monitor (VVM)
What is a VVM?
A VVM is a small sticker/label made of heat-sensitive material (para-toluene sulphonate) that is placed directly on the vaccine vial by the manufacturer.
From Park's:
"A VVM is a chemical indicator label attached to the vaccine container by the vaccine manufacturer. As the container moves through the supply chain, the VVM records its cumulative heat exposure through a gradual change in colour."
Simple explanation:
Think of a VVM like a "heat diary" for the vaccine. Every time the vaccine is exposed to heat, the VVM quietly records it by slowly changing colour. By looking at the colour, you can tell at a glance whether the vaccine has been damaged by heat.
What does a VVM look like?
It has two parts:
- Outer circle - stays the same colour always (reference)
- Inner square - made of heat-sensitive material; this is the only part that changes colour with heat exposure
The inner square starts lighter than the outer circle and gradually darkens as heat accumulates.
The 4 Stages of VVM Colour Change
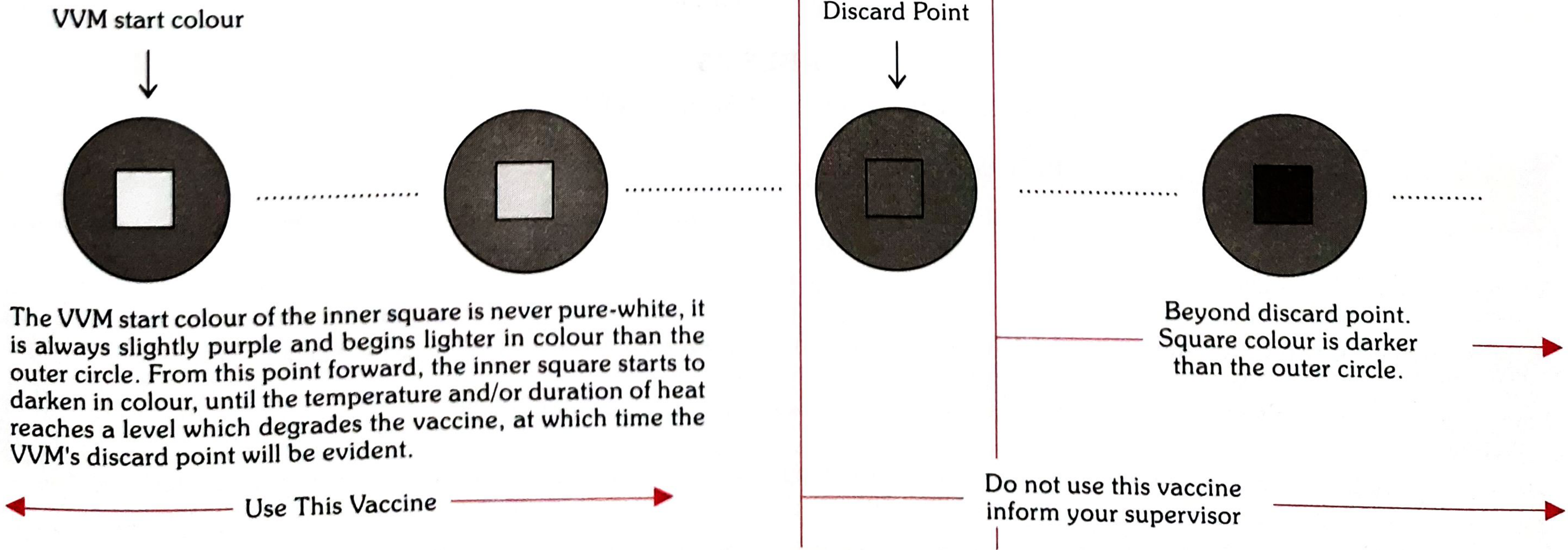
| Stage | What you see | Decision |
|---|---|---|
| Stage 1 | Inner square is lighter (white/light) than outer circle | ✅ USE the vaccine |
| Stage 2 | Inner square is still lighter (light blue) than outer circle | ✅ USE the vaccine |
| Stage 3 | Inner square colour matches (equals) the outer circle | ❌ DO NOT USE - discard point reached |
| Stage 4 | Inner square is darker (purple/black) than outer circle | ❌ DO NOT USE - beyond discard point |
Simple rule to remember:
Inner square lighter than outer circle = GOOD = USE IT Inner square same or darker than outer circle = BAD = DISCARD IT
What VVM Tells You - 3 Uses
- Ensures safety - Heat-damaged vaccines are NOT given to patients (main purpose)
- Prioritizes usage - A vaccine with more heat exposure (darker VVM) should be used BEFORE a vaccine with less heat exposure, even if the more-exposed one has a longer expiry date
- Guides decisions after cold chain breaks - Helps decide which vaccines can still be safely kept and used after a power cut or refrigerator failure - reduces unnecessary wastage
Important: VVM only measures heat exposure - it does NOT detect freezing damage. That is why the Shake Test exists separately.
4 Types of VVM
| Type | What the number means |
|---|---|
| VVM2 | Inner square reaches discard colour in 2 days at 37°C constant |
| VVM7 | Reaches discard colour in 7 days at 37°C |
| VVM14 | Reaches discard colour in 14 days at 37°C |
| VVM30 | Reaches discard colour in 30 days at 37°C |
The number = how heat-sensitive the vaccine is. A VVM2 vaccine is very heat sensitive (gets damaged fast), so it needs very careful cold storage. A VVM30 vaccine can tolerate heat a little longer.
2 Locations of VVM on Vaccine Vial
This is important for deciding how long an opened vial can be kept:
| Location | Where VVM is placed | Rule for opened vial |
|---|---|---|
| Location 1 | VVM is on the label of the vaccine vial | Once opened, can be kept for up to 28 days for subsequent immunization sessions |
| Location 2 | VVM is on the cap or neck of the ampoule (not on label) | Once opened, must be discarded at the end of the immunization session or within 6 hours of opening - whichever comes first |
Hold-Over Time (from your notes)
Hold-over time = The time taken by a Cold Chain Equipment (CCE - e.g., ILR/refrigerator) to raise its temperature to the maximum limit during loss of power.
This tells you how long the equipment can maintain safe temperatures even after power goes off. Important for planning during power cuts.
Dial Thermometer
- Used to monitor the temperature of the cold chain at the PHC (Primary Health Centre)
- Kept in the ILR (Ice-Lined Refrigerator)
- Twice daily temperature recording is done
- Works on the principle of thermocouple (two dissimilar metals that generate voltage difference with temperature change)
- Cold storage temperature: +8°C to +15°C (for cold boxes/cold rooms - not ILR which is +2 to +8°C)
Quick Summary
| Tool | Detects | Principle | Result interpretation |
|---|---|---|---|
| Shake Test | Freeze damage | Frozen vaccine's alum settles faster | Slower than control = SAFE; Same/faster = DISCARD |
| VVM | Heat damage | Para-toluene sulphonate darkens with heat | Inner square lighter = SAFE; Same or darker = DISCARD |
| Dial thermometer | Real-time temperature | Thermocouple | Used at PHC, recorded twice daily |
Source: Park's Textbook of Preventive and Social Medicine, pp. 125-126 (Shake Test and VVM sections, Cold Chain chapter). Cross-referenced with your notes (Page 74, Cold Chain topic).

image.jpg
Explain the part before shake test in short
The part before the Shake Test on your notes (page 73) covers Hold-over time, Dial Thermometer, and Cold Storage Temperature. I already have this content from the previous session - no need to search again. Here is a short, simple explanation:
Before the Shake Test (Page 73 - Immunization & Cold Chain)
1. Hold-Over Time
What it is: The time a cold chain equipment (CCE) - like a refrigerator or ILR - can maintain safe vaccine temperatures after the power goes off.
Simple example: If your fridge's hold-over time is 4 hours, it means even after the electricity cuts out, it will keep vaccines cold for 4 more hours before the temperature rises to a dangerous level.
Why it matters: In areas with frequent power cuts, you need equipment with a longer hold-over time to protect vaccines.
2. Dial Thermometer
What it does: Monitors the temperature of the cold chain at the PHC (Primary Health Centre).
4 key facts to remember:
| Point | Detail |
|---|---|
| Where it is kept | Inside the ILR (Ice-Lined Refrigerator) |
| How often recorded | Twice daily temperature recordings |
| Principle | Works on the principle of thermocouple (two different metals joined together - when temperature changes, a small voltage is produced, which is converted to a temperature reading) |
| Purpose | Ensures the cold chain is being maintained at the correct temperature |
3. Cold Storage Temperature
- +8°C to +15°C - This is the temperature for cold storage (cold boxes, walk-in cold rooms used at higher levels of cold chain)
- Remember: ILR at PHC level maintains +2°C to +8°C (for most vaccines)
In one line: Hold-over time tells you how long equipment survives a power cut; the dial thermometer (kept in ILR, recorded twice daily, based on thermocouple) monitors the temperature; and cold storage is maintained at +8 to +15°C.

image.jpg
Explain social security in detail and simple language
Finding Sources
Finding Sources
Reading File
This is a shared conversation. Sign in to Orris to start your own chat.