BER
Asking for Preferences
BER gastrointestinal
Reading File
Finding Sources
Finding Sources
Searching the Web
basic electrical rhythm BER gastrointestinal physiology slow wave
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Here is the full answer:
Basic Electrical Rhythm (BER) of the Gastrointestinal Tract
Definition
The Basic Electrical Rhythm (BER) - also called the slow wave or pacesetter potential - is the intrinsic, continuous, rhythmic oscillation in membrane potential that occurs spontaneously in GI smooth muscle. It is generated by specialized pacemaker cells called the Interstitial Cells of Cajal (ICC), located in the myenteric plexus between the circular and longitudinal muscle layers.
The BER is maintained by Na⁺-K⁺-ATPase activity, and the resting membrane potential averages approximately -56 mV.
Key Characteristics
| Feature | Detail |
|---|---|
| Origin | Interstitial Cells of Cajal (ICC) |
| Nature | Subthreshold oscillations (do NOT by themselves cause contraction) |
| Ionic basis | Slow wave phase: Na⁺ influx; Spike potential: Ca²⁺ influx (depolarization) + K⁺ efflux (repolarization) |
| Role | Sets the maximum possible frequency of contractions at each GI segment |
The BER itself rarely causes muscle contraction. Contraction only occurs when spike (action) potentials are superimposed on the depolarizing crest of the BER waves - these spikes allow significant Ca²⁺ entry, which activates calmodulin and triggers actin-myosin interaction.
BER Frequency Along the GI Tract
The BER shows a frequency gradient from proximal to distal:
| Segment | BER Frequency |
|---|---|
| Stomach | ~3-4 / min |
| Duodenum | ~12 / min |
| Distal ileum | ~8 / min |
| Cecum | ~2 / min |
| Sigmoid colon | ~6 / min |
This gradient is physiologically important - it ensures that peristaltic contractions move in an aboral (oral to anal) direction, since a wave generated proximally propagates faster than one generated more distally.
BER Diagram
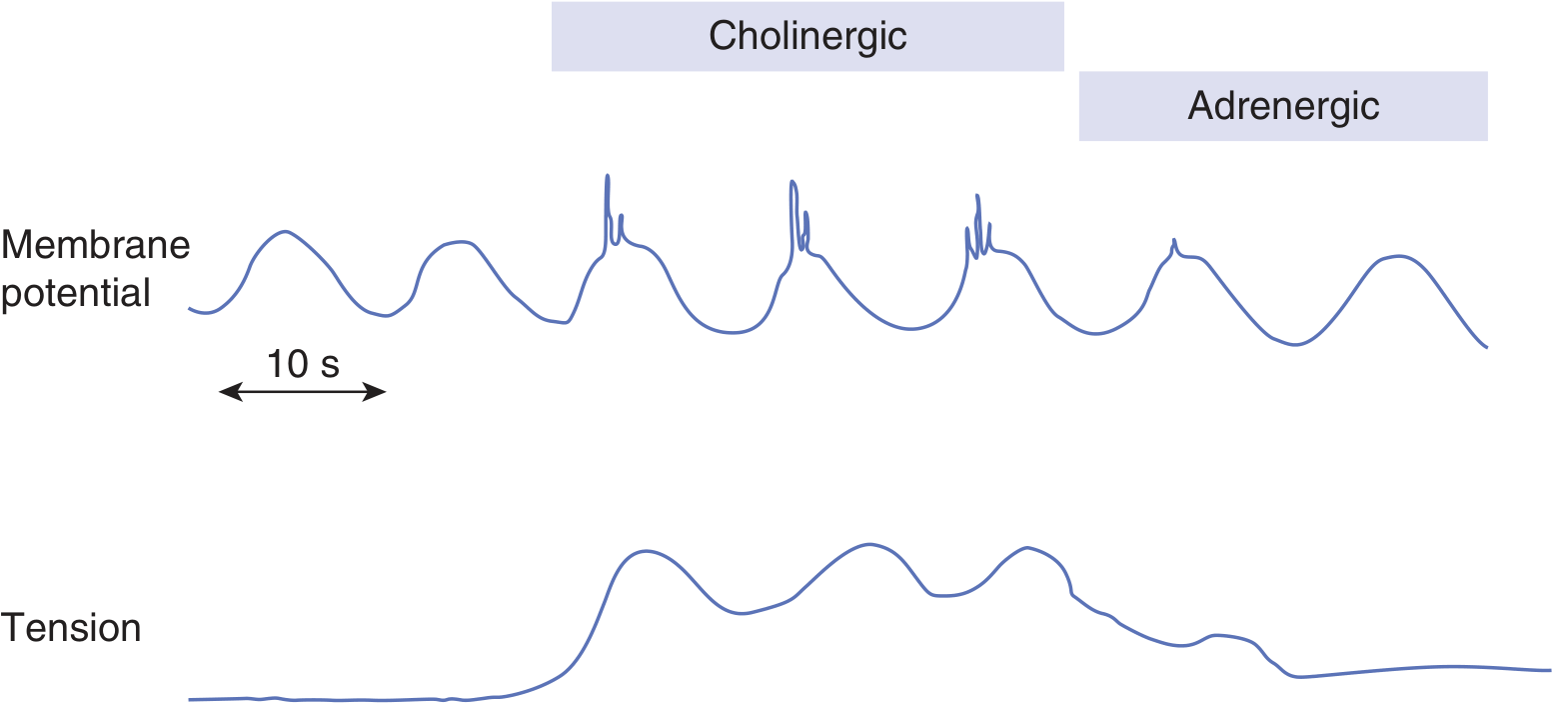
BER of gastrointestinal smooth muscle. Top: Membrane potential showing spike potentials under maximal cholinergic tone (contraction) and inhibition under adrenergic tone. Bottom: Associated changes in muscle tension. - Ganong's Review of Medical Physiology
Modulation of the BER
Factors that increase spike potentials (pro-contractile):
- Acetylcholine (parasympathetic) - increases the number of spikes and muscle tension
- Membrane stretch (e.g., distension)
- GI hormones (e.g., gastrin, motilin)
Factors that decrease spike potentials (inhibitory):
- Norepinephrine / Epinephrine (sympathetic) - hyperpolarize the membrane, suppress spikes and reduce tension
- VIP (Vasoactive Intestinal Peptide)
Functional Roles
-
Peristalsis - BER waves in the stomach wall initiate mixing waves every 15-20 seconds, progressing toward the antrum. After vagotomy or transection, peristalsis becomes irregular and chaotic, highlighting the BER's role in coordination.
-
Segmentation (mixing contractions) - The maximum frequency of segmentation contractions in the small intestine is determined by BER frequency; contractions can only occur during the depolarizing phase of the waves.
-
Gastric emptying - BER-driven constrictor rings force antral contents toward the pylorus ("pyloric pump") and cause retroulsion (mixing).
-
Aborad propulsion gradient - The duodenum-to-ileum frequency gradient ensures net distal movement of luminal contents.
Tonic vs. Rhythmic Contractions
The BER governs rhythmic (phasic) contractions. Some GI segments instead show tonic contractions (e.g., lower esophageal sphincter, ileocecal valve), which are NOT associated with BER but arise from:
- Continuous repetitive spike potentials
- Hormonal partial depolarization
- Continuous Ca²⁺ entry independent of membrane potential changes
Clinical Relevance
- Hypothyroidism: BER frequency that generates peristaltic waves in the duodenum decreases, slowing small bowel transit and potentially causing constipation or myxedema megacolon. (Sleisenger & Fordtran's GI and Liver Disease)
- Diabetic gastroparesis / loss of ICC: Destruction or reduction of ICCs (as seen in diabetes) disrupts BER generation, leading to disordered motility.
- Post-vagotomy: Irregular, chaotic peristalsis results because the coordination of BER with neural input is lost.
- Migrating Motor Complex (MMC): During fasting, the MMC (initiated by motilin every ~90 min) superimposes on the BER to create organized sweeping contractions that clear the gut.
Sources: Ganong's Review of Medical Physiology (26th ed.), p. 498 | Guyton and Hall Textbook of Medical Physiology | Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Mulholland and Greenfield's Surgery
Achlasia cardia
Finding Sources
Searching the Web
achalasia cardia pathophysiology diagnosis treatment 2024
Reading File
Searching PubMed
achalasia esophagus treatment guidelines
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from the textbooks. Here is the full answer:
Achalasia Cardia
Definition
Achalasia is a primary esophageal motility disorder characterized by two hallmark features:
- Impaired (failed) relaxation of the Lower Esophageal Sphincter (LES) with swallowing
- Aperistalsis in the smooth muscle esophagus
These result from loss of ganglion cells within the myenteric (Auerbach's) plexus in the wall of the smooth muscle esophagus, including the LES.
Epidemiology
- Incidence: ~1-2 per 100,000 per year
- Peak age: 30-60 years; bimodal distribution (young adults + elderly)
- Equal sex distribution
- Can occur at any age, including children
Etiopathogenesis
Pathological Mechanism
The core defect is degeneration of inhibitory ganglion neurons in the myenteric plexus. These neurons normally:
- Mediate deglutitive inhibition (LES relaxation via NO and VIP)
- Coordinate sequential peristalsis in the esophageal body
Their loss explains both hallmark abnormalities - impaired LES relaxation and aperistalsis.
What is lost:
- NO synthase (nitric oxide - the primary inhibitory neurotransmitter)
- VIP (Vasoactive Intestinal Peptide)-staining neurons at the gastroesophageal junction
- Partial preservation (or loss) of excitatory cholinergic neurons
Key evidence: CCK normally stimulates inhibitory neurons to relax the LES - in achalasia it paradoxically increases LES pressure, confirming inhibitory neuron absence.
Etiology
Evidence increasingly points to an autoimmune process in genetically susceptible individuals:
- Myenteric plexus infiltrate is predominantly cytotoxic T cells
- Antibodies against myenteric neurons detected in serum
- Association with specific HLA alleles
- Suspected trigger: HSV-1 (Herpes Simplex Virus type 1) - a chronic/latent infection
- The degree of ganglion cell loss parallels disease duration
Secondary Causes (Pseudoachalasia)
- Chagas disease (Trypanosoma cruzi) - also affects heart, brain, GI tract
- Malignancy (especially esophageal/GEJ carcinoma) - must be excluded in patients >60 years with short symptom duration and significant weight loss
- Allgrove (Triple A) Syndrome - achalasia + alacrima + adrenal insufficiency
Chicago Classification (HRM Subtypes)
| Type | Description | Treatment Response |
|---|---|---|
| Type I (Classic) | Complete aperistalsis, no pressurization; late disease | Moderate - 81% success LHM |
| Type II (With compression) | Aperistalsis + panesophageal pressurization; early disease | Best - up to 100% PD, 93% LHM |
| Type III (Spastic) | Premature/spastic contractions distally; unique pathogenesis (inflammation without destruction) | Poor with PD (~40%); better with LHM (86%) or POEM |
Type II represents early disease before progressive esophageal dilatation; Type I is end-stage.
Clinical Features
Symptoms (in decreasing frequency):
| Symptom | Frequency |
|---|---|
| Dysphagia - both solids AND liquids | ~95% |
| Regurgitation of undigested food | ~70% |
| Heartburn (from food stasis/fermentation, NOT acid reflux) | 40-50% |
| Chest pain (thought to be from esophageal distension/longitudinal muscle spasm) | 40-50% |
| Weight loss | Variable |
| Aspiration pneumonia | Up to 10% in advanced cases |
Important pearls:
- Dysphagia is simultaneous to both solids and liquids from the onset (unlike mechanical obstruction = solids first)
- Onset is gradual, present for years before diagnosis
- Regurgitation is non-bilious, non-acid, mixed with copious mucoid saliva - may occur hours after eating
- "Heartburn" is from bacterial fermentation of retained food, not GERD - many patients are mistakenly treated with PPIs for years
- Chest pain may improve spontaneously over time unlike dysphagia
Eckardt Score (severity assessment)
Attributes 0-3 points each to: dysphagia, regurgitation, weight loss, chest pain (total 0-12). Score ≤3 = treatment success.
Diagnosis
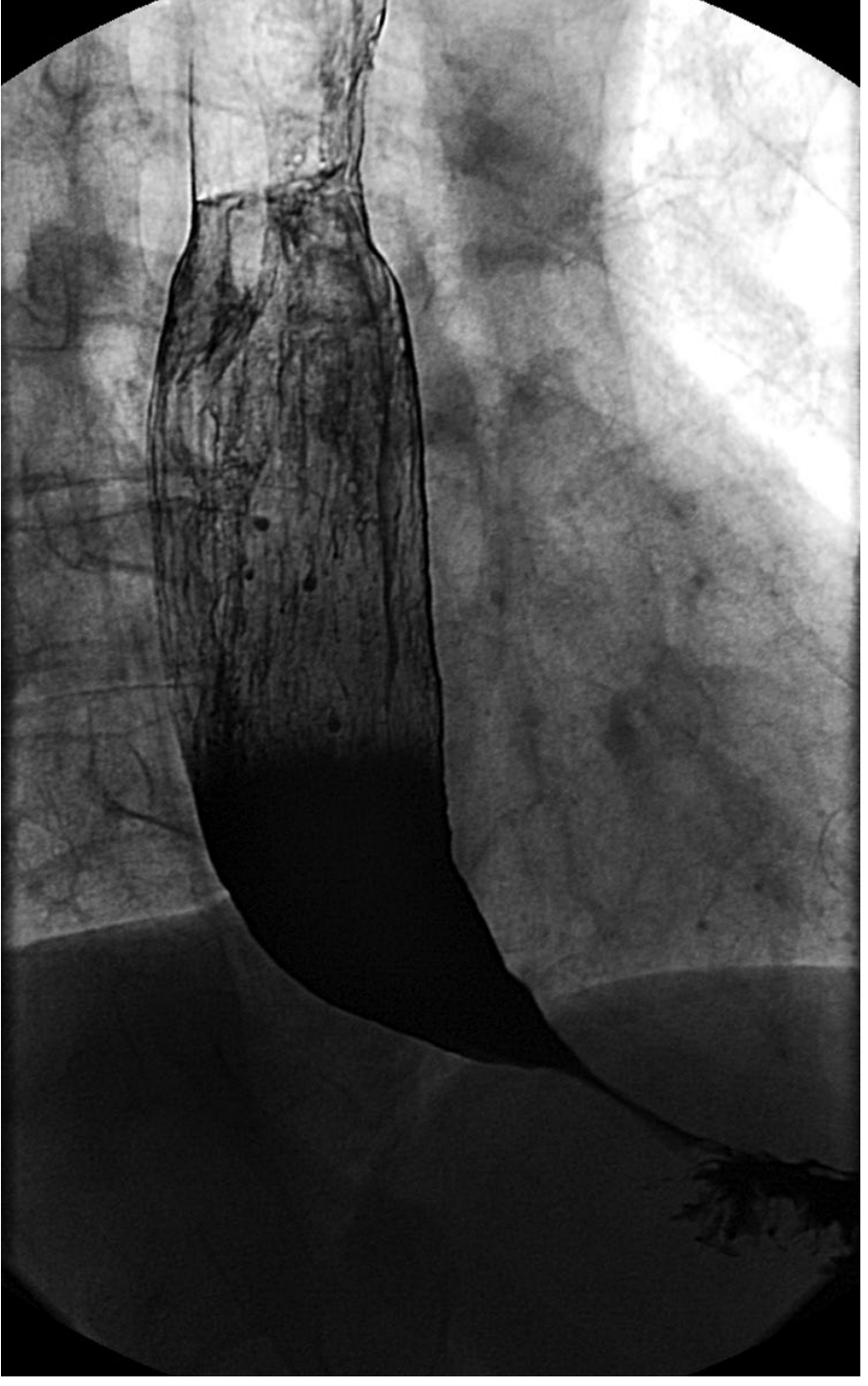
1. Barium Swallow
- First-line imaging; provides anatomic information
- Classic finding: "Bird-beak" deformity - dilated proximal esophagus tapering smoothly at the distal end/GEJ
- Other features: air-fluid level, slow emptying into stomach, tertiary contractions
- Can show sigmoid esophagus (advanced disease with massive dilatation + tortuosity) - important for surgical planning
- May be normal in ~30% of early cases
Barium swallow showing dilated esophagus with characteristic narrowing at the LES:
2. Endoscopy (EGD)
- Performed first in all patients with dysphagia to exclude malignancy (pseudoachalasia)
- Findings: retained food/saliva (~60%), esophagitis from food stasis, Candida infection
- Normal in ~40% of patients
- Classic feel: "pop" or resistance on passing scope through LES - scope passes with gentle pressure
3. High-Resolution Manometry (HRM) - Gold Standard
- Most sensitive test; establishes diagnosis AND subtype (Type I/II/III)
- Key findings:
- Impaired LES relaxation - elevated integrated relaxation pressure (IRP >15 mmHg)
- Aperistalsis in the esophageal body
- Elevated LES resting pressure (often >45 mmHg)
- Essential for Chicago Classification subtyping
4. Functional Lumen Imaging Probe (FLIP)
- Newer complementary tool
- Uses impedance planimetry to assess esophageal compliance and distensibility
- Useful when manometry is non-classic but suspicion remains high
5. Ambulatory pH Monitoring
- Reserved for patients complaining of heartburn
- Distinguishes true GERD from food-fermentation pseudoreflux
- Achalasia shows: slow progressive pH drift below 4 (fermentation), NOT discrete reflux events
Treatment
Treatment is palliative - the underlying neuropathology cannot be reversed. Goal: reduce LES pressure to allow gravity-assisted esophageal emptying.
Pharmacologic (Temporizing - Poor Efficacy)
- Calcium channel blockers: Sublingual nifedipine (30-40 mg/day before meals) - side effects (flushing, hypotension, headache) limit use
- Nitrates: Isosorbide dinitrate sublingually before meals - headache is common
- Sildenafil: Blocks PDE-5, raises cGMP, relaxes smooth muscle - short duration, high cost
- All reduce LES pressure modestly; best used as temporizing measures or in frail patients unfit for definitive therapy
Botulinum Toxin Injection (Endoscopic)
- Mechanism: Irreversibly inhibits ACh release from presynaptic cholinergic terminals
- Technique: 80-100 units injected in 4 quadrants at the LES
- Efficacy: 80% symptom relief at 1 month; drops to 40% at 12 months
- Not durable - effect reversed by new axon growth
- Repeated injections cause local fibrosis - increases technical difficulty and mucosal perforation risk if LHM later needed
- Reserved for: elderly/frail patients who are poor candidates for PD, LHM, or POEM
Pneumatic Dilation (PD)
- Disrupts circular muscle of LES by forceful balloon distension to ≥3 cm diameter
- Graded approach: start with 30 mm, escalate to 35 mm and 40 mm for persistent symptoms
- Rigiflex dilators - non-compliant cylindrical balloons passed over guidewire, positioned fluoroscopically
- Efficacy: ~86% success at 2 years; 82% at 5 years (comparable to LHM)
- ~25% of patients require repeat dilations
- Risk of perforation: ~1% (comparable to LHM)
- Best for Type II achalasia (100% efficacy in some series)
- Poor response predictors: age <40, male sex, Type I or III, large esophageal diameter, post-dilation LES pressure >10 mmHg
Laparoscopic Heller Myotomy (LHM)
- Surgical division of the circular muscle fibers of the LES and cardia (6 cm on esophagus, 2-3 cm onto stomach)
- Always combined with partial fundoplication (Dor or Toupet) to prevent post-op GERD
- Efficacy: ~90% overall; best in Type II, lower in Type I and III
- Durable results; 5-year success ~84%
- Risk of perforation ~1%; post-op GERD ~10-15%
- Superior to PD for Type III achalasia (~86% vs. ~40%)
POEM - Per Oral Endoscopic Myotomy
- Endoscopic technique pioneered by Dr. Haruhiro Inoue (2008)
- Submucosal tunnel created endoscopically; circular muscle fibers divided from inside
- Advantages over LHM: no external incisions, longer myotomy possible (especially useful for Type III), shorter recovery
- Particularly effective for Type III (spastic) achalasia because a longer myotomy can be extended proximally
- Main drawback: higher rate of post-procedural GERD (no fundoplication routinely added)
- Recent meta-analysis (2024) shows comparable efficacy to LHM with fundoplication; POEM has lower dysphagia recurrence but higher reflux rates
Esophagectomy
- Last resort for end-stage/sigmoid achalasia that has failed all other treatments
- Also indicated if malignancy cannot be excluded
Complications
| Complication | Notes |
|---|---|
| Aspiration pneumonia | From chronic regurgitation; up to 10% advanced cases |
| Esophageal candidiasis | From food stasis |
| Squamous cell carcinoma | Long-term risk (~3-8% over decades); mechanism: chronic mucosal irritation from food stasis and fermentation |
| Megaesophagus / Sigmoid esophagus | End-stage dilatation with tortuosity |
| Airway compromise | Rare; dilated esophagus compresses membranous trachea |
Summary: Treatment Algorithm
Achalasia diagnosed (HRM subtyped)
|
├── Type I or II → Pneumatic Dilation (first-line) OR LHM
| └── Type II specifically: PD ~100% effective
|
├── Type III (spastic) → LHM or POEM preferred (PD inferior)
|
├── Poor surgical candidate / elderly frail → Botox injection
|
└── End-stage sigmoid esophagus → Esophagectomy
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Sabiston Textbook of Surgery (p. 1705-1706) | Ganong's Review of Medical Physiology | Clinical Gastrointestinal Endoscopy, 3e | S Das Manual of Clinical Surgery | PMID 38775883 (Heller vs. POEM meta-analysis, 2024)
This is a shared conversation. Sign in to Orris to start your own chat.