Role of external and middle ear in physiology of hearing in detail for pg ent exam Long question according to standard ent textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Role of the External and Middle Ear in the Physiology of Hearing
(Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Shambaugh Surgery of the Ear, Cummings Otolaryngology)
Introduction
The peripheral auditory system converts airborne acoustic energy into mechanical vibrations and then into fluid pressure waves in the cochlea. The key challenge is the acoustic impedance mismatch at the air-fluid interface: if sound were to hit the cochlear fluid directly, ~99.9% of its energy would be reflected, causing a 30 dB loss. The external and middle ears together act as a transformer system to overcome this mismatch, delivering sound to the inner ear with minimal energy loss.
I. THE EXTERNAL EAR
1. Components
The external ear comprises:
- The pinna (auricle)
- The external auditory meatus (EAM)
- The external auditory canal (EAC) - approximately 25-26 mm long in adults
- The outer surface of the tympanic membrane
2. The Pinna
a. Vestigial but functional in humans
The pinna is vestigial in man with non-functional auricular muscles. In lower mammals (especially predators), mobile pinnae allow active sound localization and energy focusing. Despite this, the human pinna still makes several contributions:
b. Sound Localization
- The unique morphology of the pinna and its position on the craniofacial skeleton transform incoming sounds with delay paths that depend on the direction of the sound source
- This creates head-related transfer functions (HRTFs) - frequency and direction-dependent modifications that the auditory cortex uses to localize sound in the vertical plane (elevation) and to distinguish front from back
- Interaural time differences (ITD) and interaural level differences (ILD) are both influenced by pinna morphology
c. Frequency-Specific Resonance
- When coupled with the EAM and EAC, the pinna-canal unit provides frequency-specific resonance that helps compensate for the impedance mismatch at the air-fluid interface
- This is a preparatory gain mechanism before sound reaches the middle ear
d. Clinical Significance
- A dysmorphic pinna may reflect underlying EAC and middle ear dysmorphy (developmental co-origin in utero)
- Pinna deformities demand audiovestibular workup - in Down syndrome, 3.5 pinna defects per ear are found on average (vs. 2.5 in non-Down), all associated with conductive hearing loss
- Pinna landmarks (antihelix, concha) are anchors for behind-the-ear hearing aid retention; dysmorphic pinnae may preclude standard fitting
3. External Auditory Canal (EAC)
a. Structure
The EAC is an open-ended tube approximately 25-26 mm long, with:
- An outer cartilaginous third (contains sebaceous and ceruminous glands)
- An inner bony two-thirds
- Two constrictions: at the cartilage-bone junction, and 5 mm before the tympanic membrane (the isthmus)
b. Acoustic Resonance - The Most Important Acoustic Function
The EAC acts as a resonant tube open at one end. A tube open at one end resonates at a frequency where its length equals one-quarter of the wavelength (lambda/4 resonator).
Resonant frequency = c / (4L)
Where c = speed of sound (~340 m/s) and L = effective length of canal (~25 mm):
Resonant frequency ≈ 340 / (4 × 0.025) = ~3,400 Hz (~3.4 kHz)
This resonance produces a gain of approximately 10-15 dB at around 2.7-3.4 kHz at the tympanic membrane compared to the sound field. When combined with the pinna, head, and torso contributions, the total external ear pressure gain reaches up to ~20 dB in the 2-4 kHz range - which is precisely the frequency range most important for speech intelligibility (consonant perception).
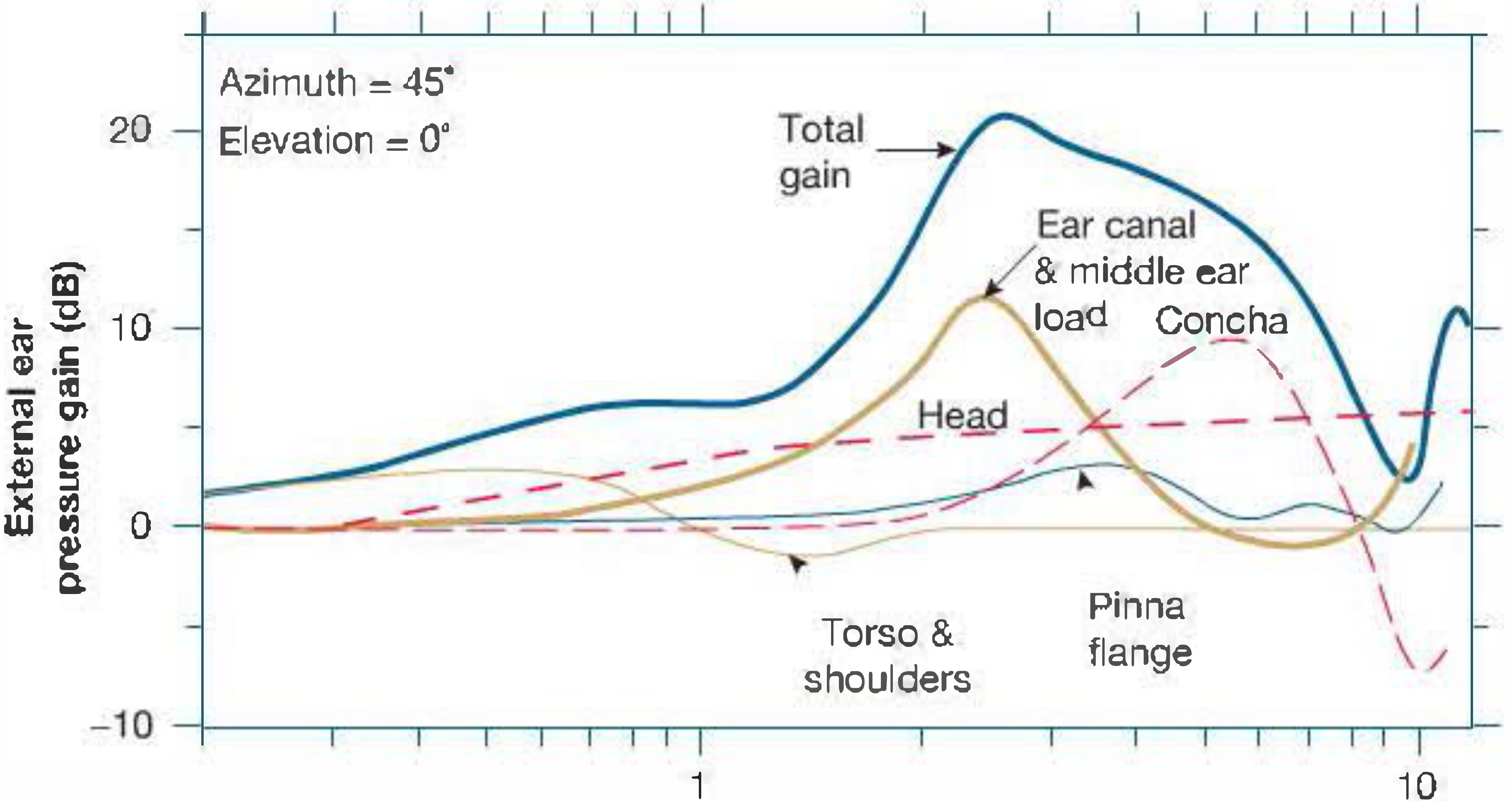
The figure shows the cumulative contributions of the head/torso, pinna flange, concha, and ear canal + middle ear load to the total external ear pressure gain (after Shaw). Maximum gain of ~20 dB occurs around 2.5 kHz.
c. Gain Distribution
The total external ear gain is the sum (in dB) of:
| Component | Gain |
|---|---|
| Head and torso diffraction | ~5 dB (broadband, increasing with frequency) |
| Pinna flange | ~5 dB (directionally dependent, peaks at 4-5 kHz) |
| Concha resonance | ~10 dB (peaks around 5 kHz) |
| Ear canal resonance + middle ear load | ~10-12 dB (peaks at 2.5-3 kHz) |
| Total | ~20 dB at 2-3 kHz |
d. Practical Implications
- Complete occlusion of the EAC by impacted wax causes up to 40 dB conductive hearing loss, with an initial high-frequency shift starting around 2 kHz (loss of resonant gain)
- In occlusive hearing aid moulds, the lost resonant gain must be incorporated into the prescription
- Cerumen serves non-acoustic functions: lubrication, antimicrobial protection, lateral migration of dead skin
II. THE MIDDLE EAR
1. Components
- Tympanic membrane (TM)
- Ossicular chain (malleus, incus, stapes)
- Middle ear muscles (tensor tympani, stapedius)
- Eustachian tube
- Oval window and round window
- Middle ear ligaments and mucosal folds
The middle ear is best understood as a band-pass mechanical filter with maximum transfer function between 1-3 kHz, determined by the stiffness and mass of its components.
2. The Air-Fluid Impedance Mismatch Problem
Acoustic impedance (Z) = pressure / volume velocity = ρc (density × speed of sound)
- Impedance of air: ~415 Pa·s/m
- Impedance of cochlear fluid (water-like): ~1.5 × 10⁶ Pa·s/m
At a direct air-fluid interface, only ~0.1% of sound energy is transmitted - equivalent to a 30 dB loss. The external and middle ears together recoup approximately 25-30 dB of this, making efficient hearing possible.
3. The Middle Ear Transformer Mechanism
The middle ear overcomes impedance mismatch through three mechanisms:
A. Hydraulic (Area) Ratio - The Principal Mechanism
The most important transformer within the middle ear is the ratio of the effective vibrating area of the tympanic membrane to the area of the stapes footplate.
- Effective vibrating area of TM: ~55 mm² (Bekesy calculated effective area ~55 mm²)
- Area of stapes footplate: ~3.2 mm²
- Area ratio = ~17:1 (Scott-Brown's gives 18:1; Shambaugh gives 17:1)
Pressure = Force / Area. If the same force (from the same sound wave) is concentrated onto a much smaller area, the pressure is amplified proportionally:
Pressure gain = 17-18× = ~24-25 dB
This is the hydraulic or area ratio.
B. Ossicular Lever Ratio
The ossicular chain acts as a Class I lever, with the fulcrum formed by the anterior and posterior malleal ligaments.
- Handle of the malleus (manubrium) is longer than the long process of the incus
- Lever ratio = 1.3:1 (Bekesy's calculation)
- This provides an additional ~2 dB gain
C. Buckling (Curved Membrane) Effect of the Tympanic Membrane
The tympanic membrane is not flat - it is cone-shaped and curved. When it vibrates, the curved membrane has a buckling action that provides an additional mechanical advantage, estimated to contribute a factor of ~2× (an additional ~6 dB). This is sometimes called the "catenary" or "lever" action of the curved membrane.
Note: The buckling effect is debated in the literature and not uniformly quantified, but is accepted as a contributor.
4. Total Transformer Ratio
Combining the two primary, well-established mechanisms (Scott-Brown's, Shambaugh):
| Mechanism | Ratio | Gain (dB) |
|---|---|---|
| Area ratio (TM:stapes footplate) | 17-18:1 | ~24-25 dB |
| Ossicular lever ratio | 1.3:1 | ~2 dB |
| Combined (hydraulic × lever) | ~22:1 | ~27 dB |
"Bekesy calculated the effective vibrating surface of TM area compared with stapes footplate area to be 17:1 and the lever effect of the ossicular chain 1.3:1. The 17:1 hydraulic ratio × the 1.3 lever ratio yields a total increase of pressure at the oval window of 22 times, termed the sound-pressure transformer ratio of the normal human ear and equates to approximately 27 dB gain."
- Shambaugh Surgery of the Ear
5. The Tympanic Membrane
Structure and Vibration:
- The TM has two parts: the pars tensa (tight, fibrous, the primary vibrating portion) and the pars flaccida (Shrapnell's membrane, less tight)
- The outer (canal) surface shows a uniphasic response with little pressure variation
- The inner (middle ear) surface shows a multiphasic response with significant pressure variation - due to the non-uniform structure providing multiple integrated multilever mechanical advantage
- A travelling wave is set up in the TM, mainly collected at the rim and conducted to the umbo, then coupled to the manubrium of the malleus
- At low frequencies (<1 kHz): membrane transfers energy by uniform movement to the malleus
- At high frequencies: movement is more complex, with partial shunting by the middle ear
- Reflectance of the membrane is high at low frequencies (<1 kHz) and lowest between 1-4 kHz - meaning maximum energy delivery to the cochlea occurs in this speech-critical range
- Above 15 kHz, reflectance again rises toward total, suggesting the middle ear limits sound propagation at very high frequencies
Clinical point: Tympanic membrane perforations reduce the pressure difference across the membrane, shunt volume velocity to the middle ear cavity, and remove sound protection from the round window. Hearing loss is proportional to perforation size and inversely proportional to frequency (greatest at low frequencies). Central perforations preserve the rim (energy transfer conduit), so hearing is better preserved than marginal perforations.
6. The Ossicular Chain
Ossicles: Malleus (lateral, attached to TM at umbo), incus (middle), stapes (medial, footplate in oval window)
Joints:
- Incudomalleal joint: saddle joint, rigid at speech frequencies, allowing malleus and incus to move as a unit
- Incudostapedial joint: lenticular process of incus + capitulum of stapes; allows some independent stapes movement
Mechanics:
- The ossicles act as a series of coupled levers transmitting vibrations from the TM to the oval window
- The manubrium of the malleus and the long process of the incus have different lengths, constituting the lever system
Ossicular coupling (Fig. 48.13 from Scott-Brown's) demonstrates how the three ossicles are anatomically arranged to transfer mechanical energy efficiently from a large area (TM) to a small area (footplate).
7. The Middle Ear Space and Pressure Regulation
Middle ear as a band-pass filter:
- Stiffness of the middle ear system (determined by TM, ossicular ligaments, air column compression): limits low-frequency transmission (stiffness-dominated below resonance)
- Mass of the system (dominated by ossicles): limits high-frequency transmission (mass-dominated above resonance)
- Maximum energy transfer between 1-3 kHz (resonant frequency range)
Role of the Eustachian tube:
- Maintains air pressure equalization between middle ear and nasopharynx
- Tubal opening is best demonstrated at 6-8 kHz (high-frequency sounds), evolutionarily appropriate since consonant-containing speech sounds are in the high-frequency range
- Eustachian tube dysfunction (e.g., early OME): deprivation of air increases stiffness → low-frequency conductive hearing loss
- Progression to fluid (glue ear): increased mass → high-frequency hearing loss
8. The Middle Ear Muscles
A. Tensor Tympani
- Innervation: Trigeminal nerve (V₃ - medial pterygoid nerve)
- Attachment: To the handle (manubrium) of the malleus
- Action: Pulls malleus anteriorly, tensing the TM
- Activation: Low electrical activity in response to sound; primarily active with tactile EAC/facial stimulation, swallowing, anticipation of loud sounds, startle (all involve bony skull movement that can stimulate the cochlea)
- Disorder: "Tensor tympani syndrome" - audible thump in ear (rare)
B. Stapedius
- Innervation: Facial nerve (VII)
- Attachment: To the neck of the stapes
- Action: Pulls annular ligament of the footplate; stiffens the ossicular chain
- Activation: Primarily responds to high-intensity, low-frequency sounds (~0.8 kHz); bilateral reflex even with unilateral stimulation
The Acoustic (Stapedial) Reflex:
- Reflex arc: auditory stimulus → cochlear nerve → cochlear nuclei → superior olivary complex → facial motor nucleus → stapedius → stiffens ossicular chain
- Moves stapes ~50 micrometers
- Increases impedance of the middle ear system
- Attenuates sound reaching the cochlea, especially at low frequencies, by 10-15 dB
- Effectively protects the cochlea from loud, low-frequency sounds and preserves perception of high-frequency consonant-containing speech in a noisy environment
- Pre-vocalization (efferent) reflex: both muscles contract before speech to protect the ear from one's own voice (bone-conducted stimulation via the skull)
- Latency is ~25-150 ms; therefore the reflex cannot protect against sudden impulse noise (e.g., gunshot)
- The reflex is abolished in: middle ear disease, facial nerve palsy (ipsilateral), auditory neuropathy
Clinical use of the acoustic reflex (tympanometry):
- Presence/absence indicates integrity of the reflex arc
- Useful to distinguish middle ear disease from sensorineural/neural pathology
- Preserved in cochlear SNHL (reflex usually present, may be at lower SL - "reflex decay" in retrocochlear pathology)
9. The Middle Ear Windows
A. Oval Window
- Sealed by the stapes footplate and annular ligament
- The primary site of preferential sound energy delivery to the cochlea
- At higher frequencies, the middle ear cavity occasionally shunts this preference
B. Round Window
- Covered by the secondary tympanic membrane (flexible)
- Functions as a pressure relief valve: when the stapes footplate moves inward (via the oval window), the round window membrane moves outward
- This out-of-phase movement is essential for the cochlear travelling wave - cochlear fluid is incompressible, so fluid displacement at the oval window must be accommodated by an equal displacement at the round window
- The pressure difference between oval and round windows drives cochlear fluid movement and is the essential stimulus for inner ear transduction
- The intact tympanic membrane protects the round window from sound reaching it directly in phase with the oval window (which would cancel the pressure differential and abolish hearing)
C. "Third Window" Concept
- Virtual third windows (vestibular aqueduct, bony skull, ossicular inertia) can shunt some energy from the middle ear
- Pathological third windows (e.g., superior semicircular canal dehiscence, perilymph fistula, dilated vestibular aqueduct): absorb or shunt preferential oval window energy, producing:
- Decreased air-conduction thresholds
- Improved (paradoxically enhanced) bone-conduction thresholds
- A "false" or spurious air-bone gap on audiometry
III. SUMMARY - THE COMPLETE SOUND PATHWAY
Airborne sound wave
↓
Pinna (localization, frequency-specific resonance, HRTF)
↓
External Auditory Canal (resonance at ~3 kHz, +10-15 dB gain)
↓
Tympanic membrane (vibrates; multilever buckling; area 55 mm²)
↓
Ossicular chain: Malleus → Incus → Stapes (lever ratio 1.3:1)
↓
Stapes footplate (area 3.2 mm²) → Oval window
[Transformer ratio ~22:1 = ~27 dB gain]
↓
Cochlear fluid: pressure wave (oval window in, round window out)
↓
Basilar membrane travelling wave → Hair cell transduction
↓
VIII nerve → Auditory cortex
IV. APPLIED POINTS FOR PG ENT EXAM
| Condition | Mechanism | Effect |
|---|---|---|
| Total TM perforation | Loss of transformer ratio + loss of round window protection | Up to 40-45 dB CHL |
| Ossicular discontinuity behind intact TM | No lever/area mechanism; both windows protected | Up to 60 dB CHL (maximum CHL) |
| Otosclerosis (stapes fixation) | Increased stiffness at footplate | Low-frequency CHL initially; Carhart's notch at 2 kHz |
| Glue ear (OME) | Increased mass (fluid) | High-frequency CHL; increased stiffness (air deprivation) causes low-frequency loss early |
| Tympanosclerosis | Loss of multilever action, but rim integrity preserved | Hearing preserved if oval window distribution intact |
| SCC dehiscence / Large vestibular aqueduct | Pathological 3rd window | Spurious air-bone gap, low-frequency CHL |
| Facial nerve palsy | Loss of stapedius reflex | Hyperacusis, loss of acoustic reflex |
| Hearing aid fitting | Relies on understanding EAC resonance and pinna gain | Occlusion effect must be compensated |
References:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Ed. - "Applied Physiology of Hearing" (Soumit Dasgupta), pp. 619-625
- Shambaugh Surgery of the Ear - "Physiology of Middle Ear" (Block 1, pp. 78-80; Block 5, p. 492)
- Cummings Otolaryngology Head and Neck Surgery - Middle Ear Physiology section
This is a shared conversation. Sign in to Orris to start your own chat.