Optical coherence tomography in ent
optical coherence tomography ENT otolaryngology
optical coherence tomography ENT otolaryngology applications 2024 2025
PMID: 38032064
https://almclinmed.ru/jour/article/view/17554
optical coherence tomography middle ear tympanic membrane larynx
Optical Coherence Tomography (OCT) in ENT
What is OCT?
- Resolution: 1-15 µm axially (far higher than ultrasound or MRI)
- Imaging depth: ~1-2 mm into tissue
- Non-ionizing, non-contact, real-time imaging
- Can be integrated with endoscopes, surgical microscopes, or handheld probes
OCT Technologies Used in ENT
| Type | Principle | ENT Use |
|---|---|---|
| Time-domain OCT (TD-OCT) | Moving reference mirror | Early research; slower |
| Spectral-domain OCT (SD-OCT) | Fourier-transform analysis; no moving parts | Most widely used clinically |
| Swept-source OCT (SS-OCT) | Tunable laser source; greater depth | Deep tissue/middle ear |
| OCT Angiography (OCTA) | Detects blood flow via phase variance | Vascular assessment of mucosa, TM |
| Polarization-sensitive OCT (PS-OCT) | Tissue birefringence | Collagen/fibrosis detection, laryngeal tumors |
| Doppler OCT | Frequency shift from moving particles | Mucociliary clearance measurement |
ENT Applications
1. Larynx and Vocal Cords (Most Advanced Application)
- Distinguishing benign vs. malignant lesions: Endoscopic OCT used in combination with microlaryngoscopy significantly increases sensitivity for detecting malignancy and grading precancerous lesions compared to microlaryngoscopy alone
- "Optical biopsy": OCT provides virtual histological sections without tissue removal; studies are ongoing to determine whether it can replace excisional biopsy
- Diagnosis of small epithelial lesions: OCT has received support as a tool for diagnosing smaller glottic epithelial lesions, guiding resections, and monitoring the larynx after therapy (e.g., radiotherapy or surgery)
- Vocal fold subepithelial architecture: Quantitative OCT can distinguish unique vocal fold subepithelial architectural patterns
- Vocal cord leukoplakia: Machine learning-assisted handheld OCT (2025 data) has shown promise for real-time intraoperative classification of vocal cord leukoplakia

2. Middle Ear and Tympanic Membrane
- Tympanic membrane imaging: Structural assessment of the TM layers (outer squamous epithelium, fibrous middle layer, inner mucosal layer); detection of TM perforations and retraction pockets
- Middle ear effusion (Otitis Media with Effusion): OCT can visualize middle ear contents through an intact TM - detecting fluid, biofilm, or normal air. This is a major potential advance, as diagnosis currently relies on clinical judgment and tympanometry
- Cholesteatoma: OCT can differentiate cholesteatoma matrix from granulation tissue and middle ear contents
- Ossicular chain visualization: Promontory, ossicles, and chorda tympani can be imaged; tympanic cavity masses and their vascularization degree assessed via SD-OCT and OCTA
- OCT-guided cochleostomy: Temporal bone experiments showed OCT can image cochlear structures to guide cochleostomy technique in cochlear implant surgery
- Cochlear implant electrode placement: Intracochlear OCT guidance for electrode array insertion (active research area as of 2025)
- Cochlear mechanics research: High-speed OCT measures basilar membrane and outer hair cell displacement gain in living cochleae
3. Sinonasal Mucosa
- Morphological pattern recognition: OCT identifies distinct structural patterns in the mucosa specific to individual diseases (e.g., chronic rhinosinusitis, rhinitis subtypes)
- Mucosal structural changes after treatment: OCT can monitor structural response to medical therapy (steroids, biologics) or surgical procedures (FESS)
- Mucociliary clearance measurement: Doppler OCT can measure ciliary beat frequency and mucus flow in real time - relevant for primary ciliary dyskinesia, CF, and post-surgical assessment
- Nasal mucosa in vivo: In vivo OCT of nasal mucosa was first demonstrated in 2006
4. Pharynx and Tonsils
- OCT can assess tonsillar crypt architecture and peritonsillar tissue microstructure
- Research has explored OCT imaging in tonsillopharyngitis and parapharyngeal space lesions
- OCT angiography can monitor microvascular changes in pharyngeal inflammation (capillary permeability, vascular stasis, exudation as markers of inflammation severity)
5. Salivary Glands and Oral Cavity
- Structural imaging of salivary gland ducts and parenchyma (relevant for Sjogren's, obstructive sialadenitis)
- Assessment of oral mucosal lesions, leukoplakia, and early malignancy detection
Technical Configurations for ENT
| Configuration | Details |
|---|---|
| Endoscopic OCT probes | Miniaturized probes compatible with standard rigid or flexible endoscopes |
| Surgical microscope-integrated | Integrated with operating microscope for intraoperative use (larynx, ear) |
| Handheld probes | For outpatient clinic or bedside use (vocal cords, tympanic membrane) |
| Otoscope-integrated | Specially designed for TM and middle ear imaging |
| Catheter-based | For subglottic or tracheal imaging |
Advantages of OCT in ENT
- Non-invasive / non-ionizing - no radiation exposure
- Real-time imaging - immediate intraoperative feedback
- Histological resolution - can reveal epithelial thickness, basement membrane integrity, subepithelial architecture
- "Optical biopsy" - may reduce need for surgical biopsy in select cases
- Functional imaging - Doppler OCT assesses mucociliary clearance; OCTA assesses microvascular flow
- Compatible with existing endoscopes - relatively straightforward integration
Limitations
- Limited penetration depth (~1-2 mm) - cannot assess deep tissue or cartilage infiltration
- Motion artifacts - significant issue in the moving larynx
- Interpreter expertise - requires training to read OCT images
- Not yet standard of care in any ENT subspecialty
- Evidence base is still limited - most studies are small and exploratory
- Cost - specialized probes and systems add expense
Current Status and Future Directions
- AI/machine learning-assisted OCT interpretation (particularly for laryngeal lesion classification)
- OCTA integration for microvascular mapping in ENT tumors and inflammatory conditions
- OCT-guided cochlear implant surgery (active clinical trials in 2025)
- Portable/handheld OCT devices for office-based ENT practice
Recent evidence note: A 2023 systematic review (PMID 38032064) confirmed OCT's potential for sinonasal imaging but concluded that current evidence quality is low to moderate and larger controlled studies are needed before routine clinical adoption.
Narrow band imaging
narrow band imaging larynx head neck
narrow band imaging NBI ENT larynx pharynx head neck surgery 2024 2025
PMID: 33213196
Narrow-Band Imaging (NBI) in ENT
Principle and Technology
- Depth of light penetration is wavelength-dependent - shorter wavelengths penetrate shallower
- Hemoglobin has peak absorption at specific wavelengths - blue (~415 nm) and green (~540 nm) light
| Wavelength | Color | Visualizes |
|---|---|---|
| 415 nm | Blue | Superficial capillary networks (mucosal surface) |
| 540 nm | Green | Subepithelial/deeper vessels |
Background and Origin
The Key Concept: Intraepithelial Papillary Capillary Loops (IPCLs)
- Dilatation
- Tortuosity
- Irregular caliber
- Abnormal looping/branching patterns
- Destruction of loop architecture
ENT Applications
1. Larynx (Primary and Best-Studied Application)
- Glottic leukoplakia: NBI reveals the vascular pattern beneath the white surface, allowing differentiation between benign keratosis and carcinoma in situ/invasive cancer. A systematic review (Campo et al., PMID 33213196) of 312 patients with 382 vocal cord leukoplakia lesions showed NBI accuracy for predicting malignancy ranged from 81% to 97.8%
- Precancerous lesions and carcinoma in situ: NBI better defines lesion margins and reveals satellite lesions not visible on white light

- Sensitivity: 89%
- Specificity: 93%
- PPV: 91% | NPV: 92% | Accuracy: 90% (Ni et al. classification)
- Even higher values in post-radiotherapy/chemoradiotherapy surveillance, reducing the need for tissue biopsy in these cases
- Transoral laser microsurgery (TLM): NBI identifies precise resection margins during surgery for early glottic cancer, reducing positive margins and recurrence
- Directing biopsies: NBI highlights the most "suspicious" areas under leukoplakia, improving biopsy yield
- Recurrent respiratory papillomatosis (RRP): The ELS classification system can differentiate papilloma from malignant lesions based on the angle of the turning points of perpendicular vascular changes
- Higher accuracy than white-light in detecting second tumors in the oropharynx and hypopharynx after treatment
- Detects radiation-induced mucosal changes and recurrence
2. Hypopharynx and Oropharynx
3. Oral Cavity
- Assessment of oral potentially malignant disorders (leukoplakia, erythroplakia, submucosal fibrosis)
- Mapping lesion extent before surgical excision
- Biopsy guidance to most dysplastic areas
Vascular Classification Systems
Ni et al. (2011) Classification
European Laryngological Society (ELS) Classification
- Sensitivity: 100%
- Specificity: 95%
- PPV: 100%
- NPV: 96%
NBI vs White-Light Endoscopy: Key Advantages
| Feature | White-Light | NBI |
|---|---|---|
| Mucosal surface detail | Moderate | High |
| Submucosal vessels | Poor | Good |
| Lesion margin delineation | Imprecise | Precise |
| IPCL visualization | No | Yes |
| Satellite lesion detection | Often missed | Enhanced |
| Guides biopsy | No | Yes |
| Needs dye/contrast | No | No |
| Cost | Standard | No extra cost (built-in) |
Limitations
- Learning curve - requires training to interpret aberrant microvascular architecture accurately; significant interobserver variability among untrained users
- Superficial depth only - assesses mucosal and submucosal vasculature; cannot assess the deep extent of tumor invasion (cartilage, muscle) - CT/MRI still needed for staging
- Not a replacement for biopsy - NBI is "optical biopsy" but histology remains the gold standard; NBI guides but does not replace tissue diagnosis
- Motion and secretions - laryngeal movement and mucus can degrade image quality
- Distance-dependent - image quality diminishes with greater endoscope-to-lesion distance; contact or near-contact endoscopy is optimal for IPCL detail
Clinical Role: "Optical Biopsy"
- Pre-operatively: Identifies which patients with leukoplakia need urgent microlaryngoscopy and biopsy vs. watchful waiting
- Intra-operatively: Guides resection margins in TLM
- Post-treatment: Reduces unnecessary biopsies in surveillance by distinguishing radiation changes from recurrence
Recent evidence: A 2022 systematic review (Campo et al., PMID 33213196) confirmed NBI accuracy of 81-97.8% for predicting malignant transformation in vocal cord leukoplakia, concluding NBI helps in the decision-making process on whether to perform biopsy, transoral surgery, or long-term follow-up.
Contact endoscopy
contact endoscopy larynx head neck mucosal
contact endoscopy ENT larynx technique applications 2023 2024 2025
contact endoscopy vocal cord leukoplakia dysplasia diagnosis
Contact Endoscopy in ENT
Definition and Concept
Historical Development
- 1865 - Desormaux: first description of contact endoscopy, observing the vascular network of the bladder mucosa
- 1955 - Jaupitre: contact cystoscopy with photography and cinematography
- 1983 - Hamou: developed microcolpohysteroscopy for cervical pathology in gynaecology
- 1995 - Contact microlaryngoscope developed; study of the larynx using CE initiated
- 2007 - CE combined with Olympus Narrow-Band Imaging (NBI) illumination, enhancing visualization of deeper vessels via selective haemoglobin absorption
Instruments
| Scope | Specs | Site |
|---|---|---|
| Karl Storz 8715 AA | 5.8 mm diameter, 24 cm length, 0° | Larynx / hypopharynx |
| Karl Storz 8715 BA | 5.8 mm diameter, 24 cm, 30° angulation | Difficult laryngeal angles |
| Karl Storz 7215 AA/BA | 4 mm diameter, 18 cm length | Nasal cavity, oral cavity, oro/nasopharynx |
Technique
Staining Protocol
-
Vascular mode (no staining): The contact endoscope is applied directly to the mucosa without staining. The microcirculation is visible with regular light. Adding NBI illumination greatly enhances vascular visualization by improving contrast against surrounding tissues and revealing deeper vessels.
-
Cellular mode (methylene blue staining): The mucosa is stained with methylene blue (contact endoscopy) or Lugol's iodine. The stain lasts 4-5 minutes. At ×60-×150, cells, nuclei, cytoplasm, and the nucleus:cytoplasm ratio can all be assessed in the first three layers of epithelial cells.
Anaesthesia Requirements
- Larynx and hypopharynx: Requires general anaesthesia with endotracheal intubation
- Nasal mucosa, nasopharynx, oral cavity, oropharynx: Can often be performed without anaesthesia (office setting)
Normal Appearances
- Nuclei: Regular, homogeneous, uniformly sized and distributed
- Ciliated epithelium: Visible cilia and regular columnar cell arrangement
- Vascular pattern - vocal cord: Blood vessels run parallel to each other, connected by transverse anastomotic vessels - an arrangement that favours vibratory movement of the vocal mucosa
- Other mucosal sites: Vessels course parallel to the surface, connected by anastomoses forming a plexus; perpendicular vessels (IPCLs) are normal at specific sites (gums, hard palate, superior tongue surface, nasal papillae)
- Glandular orifices scattered throughout the upper aerodigestive tract mucosa
Pathological Patterns
Keratosis
- Isolated cells without nuclei are identified initially
- Individual cells cannot be identified in areas of amorphous or laminar structure
- Different degrees of keratinization can be observed within the same lesion
- Vessels may pass below the keratotic area or surround the leukoplastic lesion
Dysplasia
- Altered nucleus:cytoplasm ratio (dyskaryosis)
- Anisokaryosis (variation in nuclear size)
- Nuclear hyperchromasia
- Abnormal nuclear shape
- Keratosis (may coexist)
- With leukoplakia: heterogeneous cellular population, with multiple pathological alterations visible simultaneously
Carcinoma / Tumour
- Nuclear irregularities: Irregular in size, shape, and colouration
- Disturbed angioarchitecture: Atypical vessels with:
- Differences in calibre and shape
- Ectasias
- Haemorrhages
- Reduced blood flow resulting in thrombosis
- Necrosis in aggressive disease
- Where deep infiltration without surface involvement exists: Normal superficial cells may be seen with vascular alterations only - an important recognition
- Safety margins can be established and transition areas identified
Papilloma (Recurrent Respiratory Papillomatosis)
- CE identifies the extent of papillomatous disease
- Assists with assessing complete removal
- NBI-enhanced CE can differentiate papilloma from malignant degeneration based on vascular turning point angles (ELS classification)
Chronic Inflammation / Infection
- Vascular dilation and proliferation
- Altered cellular arrangement
- Fungal infection with concurrent dysplasia produces specific findings distinguishable from pure dysplasia
- In aggressive inflammation: aberrant vessel shape causing thrombosis and tissue necrosis
Diagnostic Performance
- Sensitivity: 90%
- Specificity: 94%
- Agreement with histopathology: 88% (after appropriate training)
- High efficacy reported for mucosal lesions across multiple sites in the head and neck
- Accuracy for distinguishing dysplasia and malignancy in vocal cord leukoplakia: 81-97.8%
Site-Specific Applications
| Site | Application |
|---|---|
| Larynx / Vocal Cords | Leukoplakia grading, dysplasia detection, carcinoma in situ, tumour margins, RRP extent, post-treatment surveillance |
| Nasal Cavity | Mucosal pathology, polyp characterization, inflammatory vs. neoplastic distinction |
| Nasopharynx | Assessment of nasopharyngeal mucosa; early NPC detection; recurrent NPC post-treatment |
| Oral Cavity | Leukoplakia, erythroplakia, tongue lesions, biopsy guidance |
| Oropharynx | Tonsillar and soft palate lesions, margin delineation |
| Hypopharynx | Performed under GA; tumour extent mapping |
| Trachea | Specialized probes available |
| Thyroid surgery | Recent application: identification of parathyroid glands intraoperatively using CE (comparable to frozen section analysis) |
Advantages
- In vivo, in situ cellular diagnosis - real-time, no tissue removal required
- Non-invasive - avoids complications of unnecessary biopsy, particularly important in irradiated patients where biopsy risks are higher
- Lesion mapping - can survey the entire mucosal surface and identify multicentric disease; maps boundaries of lesion for complete resection
- Intraoperative use - enables resection guidance, safety margin confirmation, and can also be used on the excised specimen to verify complete removal
- No radiation - no ionizing risk
- Combines with NBI - adding NBI illumination dramatically enhances vascular assessment
- Immediate result - findings can be shared immediately and video reviewed collaboratively with pathologist/cytologist
Limitations
- Superficial depth of penetration - only the first 3 layers of epithelium are assessed; deep tissue invasion is not evaluable
- Cannot confidently distinguish intraepithelial neoplasia from invasive carcinoma - both may show dysplastic cellular features; deep invasion cannot be confirmed
- Impaired visualization with keratosis - thick keratin layer prevents cellular assessment of underlying epithelium
- Scarring and chronic inflammation - impairs visualization of malignant cells
- Learning curve - requires significant training to interpret cellular and vascular images correctly; experience needed to handle delicate tissues without trauma
- GA required for larynx/hypopharynx - not fully office-based for the most important application site
- Not a histology replacement - designed as a complement, not substitute; tissue biopsy remains gold standard
Comparison with NBI
| Feature | Contact Endoscopy | NBI |
|---|---|---|
| Magnification | ×60-×150 (cellular) | Standard endoscopic |
| What is visualized | Individual cells + vessels | Vascular patterns only |
| Staining needed | Methylene blue (for cells) | None |
| Cellular detail | Yes | No |
| Vascular detail | Yes (with NBI illumination) | Yes |
| GA required (larynx) | Yes | No (flexible scope) |
| Learning curve | Steep | Moderate |
| Depth assessed | Superficial epithelium | Mucosal + submucosal vessels |
Key point from Scott-Brown's: Contact endoscopy is currently confined to clinical research in the larynx but shows promise for wider clinical application. Its main advantage is avoiding the complications of unnecessary biopsy - particularly in irradiated patients.
Narrow band imaging
Narrow-Band Imaging (NBI) in ENT - Summary
Principle
- 415 nm (blue) - absorbed by superficial capillaries; highlights mucosal surface vessels
- 540 nm (green) - absorbed by deeper submucosal vessels
Key Concept: IPCLs
- Dilatation, tortuosity, irregular caliber
- Abnormal looping and branching
- Destruction of loop architecture
Applications in ENT
| Site | Use |
|---|---|
| Larynx | Leukoplakia grading, carcinoma in situ, tumour margin delineation, biopsy guidance, post-radiotherapy surveillance |
| Hypopharynx / Oropharynx | Synchronous/metachronous second primary tumour detection |
| Oral cavity | Potentially malignant disorder assessment |
- Sensitivity 89%, Specificity 93%, Accuracy 90% (Ni et al. classification)
- ELS classification: Sensitivity 100%, Specificity 95%, PPV 100%, NPV 96%
- Accuracy for vocal cord leukoplakia malignancy prediction: 81-97.8% (Campo et al. 2022, PMID 33213196)
Classification Systems
- Ni et al. (2011) - Detailed IPCL morphology pattern typing
- ELS (European Laryngological Society) - Simpler, clinically practical; recommended standard in Europe; differentiates papilloma from malignancy by vascular turning point angles
Clinical Role
- Pre-op: Identifies which leukoplakia patients need urgent biopsy vs. watchful waiting
- Intra-op: Guides resection margins in transoral laser microsurgery (TLM)
- Post-treatment: Distinguishes radiation change from recurrence, reducing unnecessary biopsies
Limitations
- Superficial depth only - cannot assess deep tumour invasion (CT/MRI still needed for staging)
- Steep learning curve for IPCL interpretation
- Does not replace histological biopsy
Lasers in ent for 10marks question
lasers in ENT otolaryngology types applications physics CO2 KTP Nd:YAG thulium 2024
LASERS IN ENT - 10 Mark Answer
1. Introduction: What is a LASER?
- Monochromatic - single, pure wavelength
- Coherent - all waves in phase (spatial and temporal)
- Collimated - minimal divergence; can be focused to a tiny spot
2. Laser Physics: Key Parameters
| Parameter | Definition | Relevance |
|---|---|---|
| Wavelength | Determines tissue absorption | Selects target chromophore |
| Power (Watts) | Energy output per unit time | Cutting vs. coagulation |
| Power density (W/cm²) | Power / spot area | Determines tissue effect |
| Spot size | Smaller spot = higher power density | Focus = cut; defocus = coagulate |
| Fluence (J/cm²) | Power density × time | Total energy delivered |
| Pulse mode | Continuous wave vs. pulsed | Pulsed reduces thermal damage |
3. Laser-Tissue Interactions
- Reflected - no effect
- Scattered - dispersed; contributes to lateral heating
- Transmitted - passes through without absorption
- Absorbed - the only portion producing surgical effect
| Temperature | Effect |
|---|---|
| 37-60°C | Protein denaturation, enzyme inactivation |
| 60-65°C | Coagulation (haemostasis) |
| 65-90°C | Welding, shrinkage |
| 100°C | Vaporization (water boils) |
| >150°C | Carbonization |
| >300°C | Combustion |
- Photocoagulation - heat coagulates proteins/blood vessels (Nd:YAG, KTP)
- Photovaporization - tissue water vaporized, ablating cells (CO₂, thulium)
- Selective photothermolysis - specific chromophore (haemoglobin/melanin) targeted; surrounding tissue spared (KTP, pulsed dye)
4. Types of Lasers Used in ENT
Lasing Media Classification
- Gas lasers: CO₂, Argon, Helium-Neon
- Solid-state lasers: Nd:YAG (neodymium-doped yttrium aluminum garnet), KTP, Ho:YAG, Thulium:YAG
- Semiconductor/Diode lasers: 810 nm diode
A. CO₂ Laser - The Workhorse of ENT
| Feature | Detail |
|---|---|
| Wavelength | 10,600 nm (far infrared, invisible) |
| Aiming beam | Coaxial He:Ne red laser needed |
| Chromophore | Water (strongly absorbed; 0.03 mm extinction length) |
| Tissue effect | Precise vaporization; minimal scatter |
| Haemostasis | Coagulates capillary-sized vessels only |
| Delivery | Articulating arm + mirrors; micromanipulator + operating microscope; flexible waveguide fiber (newer) |
- Color-independent absorption (works equally on all tissues)
- Minimal lateral thermal damage
- Excellent precision - best soft tissue interaction of any ENT laser
- Can be coupled to operating microscope via micromanipulator
- Cannot be transmitted through standard optical fibres (traditionally)
- Not haemostatic for larger vessels
- Large fibre size (1210 µm); expensive
- Cannot work with flexible endoscopes (until waveguide technology)
- Microlaryngeal surgery: leukoplakia, polyps, nodules, papilloma, granuloma, cysts
- Early glottic carcinoma (transoral laser microsurgery - TLM)
- Subglottic stenosis, laryngotracheal stenosis
- Webs, capillary haemangioma (paediatric airway)
- Laser stapedotomy (otosclerosis)
- Nasal polyp reduction (SwiftLase oscillating device)
- Laryngopharyngeal tumour resection/ablation
B. KTP Laser (Potassium Titanyl Phosphate) - Angiolytic Laser
| Feature | Detail |
|---|---|
| Wavelength | 532 nm (green, visible) |
| Chromophore | Oxyhaemoglobin |
| Tissue effect | Selective photothermolysis of vessels; haemostatic; pulsed and continuous cuts similar to CO₂ |
| Delivery | Flexible optical fibre (300-600 µm) |
| Cost | Low |
- Vocal fold lesions (angiolysis of vascular ectasias, varices)
- Papillomatosis (RRP) - equal to CO₂ for ablation, with added fibre flexibility
- Laser stapedotomy
- Vascular lesions of head and neck
- HHT (hereditary haemorrhagic telangiectasia) - telangiectasia coagulation
- Endonasal DCR
- Nasal/sinus surgery
C. Nd:YAG Laser (Neodymium:YAG)
| Feature | Detail |
|---|---|
| Wavelength | 1064 nm (near infrared, invisible) |
| Chromophore | Cellular proteins; weakly absorbed by water |
| Penetration depth | 2-4 mm deep (deepest of all ENT lasers) |
| Tissue effect | Deep coagulation/necrosis; haemostatic; less precise |
| Delivery | Flexible fibre |
- Tracheobronchial obstruction (tumour palliation via rigid bronchoscope) - most important; haemorrhage control is excellent
- Obstructing oesophageal lesions (palliation)
- Vascular malformations (low-flow venous malformations) of head and neck
- HHT telangiectasia coagulation
- Lymphatic malformations
- Contact Nd:YAG for oral cavity/oropharyngeal tumours (where generous safety margin difficult)
D. Thulium:YAG Laser (Tm:YAG) - Emerging
| Feature | Detail |
|---|---|
| Wavelength | 2010-2013 nm (infrared) |
| Chromophore | Water |
| Tissue effect | Haemostatic; precise cutting |
| Fibre size | 260 µm (smallest available - key advantage) |
| Cost | Lower than CO₂ |
E. Holmium:YAG (Ho:YAG) Laser
| Feature | Detail |
|---|---|
| Wavelength | 2100 nm (infrared) |
| Chromophore | Water |
| Effect | Cutting and ablation; less haemostatic than KTP |
| Delivery | Flexible fibre |
- Endonasal DCR (dacryocystorhinostomy)
- Nasal and sinus surgery
- Turbinate reduction
- Antrostomy
F. Argon Laser
| Feature | Detail |
|---|---|
| Wavelength | 488-514 nm (blue-green, visible) |
| Chromophore | Haemoglobin and melanin |
| Effect | Photocoagulation; selective photothermolysis |
- Laser stapedotomy (historically popular; now largely replaced by KTP/CO₂)
- HHT telangiectasia
- Nasal/sinus surgery
G. Pulsed Dye Laser (PDL)
| Feature | Detail |
|---|---|
| Wavelength | 585 nm |
| Chromophore | Haemoglobin |
| Effect | Selective photothermolysis; haemostatic |
| Delivery | 600 µm fibre |
| Disadvantage | Dye kit unreliable; higher maintenance |
Summary Comparison Table
| Laser | Wavelength | Medium | Chromophore | ENT Use |
|---|---|---|---|---|
| CO₂ | 10,600 nm | Gas | Water | Larynx (workhorse), stapedotomy |
| Thulium | 2010 nm | Solid | Water | Larynx, angiolysis |
| Ho:YAG | 2100 nm | Solid | Water | DCR, sinus, turbinate |
| Nd:YAG | 1064 nm | Solid | Protein | Trachea, vascular malformations |
| Diode | 810 nm | Semiconductor | Haemoglobin | Sinus, nasal, DCR |
| KTP | 532 nm | Solid | Haemoglobin | Larynx, stapedotomy, HHT |
| Argon | 488-514 nm | Gas | Haemoglobin | Stapedotomy (historic), HHT |
| Pulsed dye | 585 nm | Dye | Haemoglobin | Vascular, RRP |
5. ENT-Specific Applications
Laryngology (Most Common)
- RRP (Recurrent Respiratory Papillomatosis): CO₂ laser (92% preference historically); KTP and Nd:YAG equally effective with added fibre delivery; microdebrider now preferred by paediatric surgeons
- Early glottic carcinoma: TLM (Transoral Laser Microsurgery) with CO₂ - organ preservation surgery; equal or superior oncological outcomes to open surgery for T1/T2
- Leukoplakia/dysplasia: CO₂ laser excision
- Subglottic/laryngotracheal stenosis: CO₂ laser radial incisions + dilation
- Benign lesions: Polyps, nodules, granulomas, cysts - CO₂
- Vocal fold scar/ectasia/varices: KTP angiolysis
Otology
- Laser stapedotomy (otosclerosis): CO₂, KTP, or Argon laser
- 4 requirements for safe laser stapedotomy: (1) precise optics, (2) efficient bone/collagen absorption, (3) minimal perilymph heating, (4) no inner ear photon damage
- CO₂ is ideal - strongly absorbed by bone collagen/water; does NOT penetrate perilymph
- KTP/Argon: transmit through perilymph (theoretically more risk but clinical studies show safety)
- Tympanomastoid surgery: CO₂, KTP, Argon - for cholesteatoma, vascular lesions, tumours
- Myringotomy: CO₂ laser myringotomy
Rhinology / Sinonasal
- HHT (Osler-Weber-Rendu disease): KTP, Argon, Nd:YAG, diode - coagulation of telangiectasia
- Turbinate reduction: Ho:YAG, KTP, diode, CO₂
- Nasal polyposis: CO₂ SwiftLase device
- Antrostomy: Ho:YAG, KTP
- Sinonasal tumours: Holmium YAG, Nd:YAG, KTP
- Endonasal DCR: Holmium YAG, KTP, 810 nm diode
Head and Neck / Pharynx
- Tonsillectomy/tonsil reduction: CO₂, diode (laser tonsillotomy)
- Snoring/UPPP: CO₂ (laser-assisted uvulopalatoplasty - LAUP)
- Pharyngeal/hypopharyngeal tumour ablation: CO₂
- Vascular malformations: Nd:YAG, KTP
- Oral cavity tumours: Contact Nd:YAG (where margins difficult)
6. Laser Safety
- Eye protection: Appropriate wavelength-specific goggles for ALL personnel; patient eyes must be shielded
- Airway fire prevention:
- Use laser-resistant (Laser-Flex, Merocel) endotracheal tubes
- Fill cuff with saline + methylene blue (detects cuff breach)
- Reduce FiO₂ to minimum safe level (ideally <30%); avoid N₂O (supports combustion)
- Wet gauze packing around tube
- Endoscopes blackened/matt finish to reduce accidental reflections
- Warning signs + locked doors during laser use
- Laser key held by senior team member - prevents unauthorized use
- Operating room windows must be laser-protected
- Plume extractor essential - laser vapour plume carries viral particles (HPV in RRP laser plume - one documented case of surgeon acquiring laryngeal papilloma)
- Laser safety officer designated in each institution
7. Advantages of Lasers in ENT
- Precision - minimal collateral damage, bloodless field
- Haemostasis - seals capillaries as it cuts
- Reduced postoperative oedema - compared to cold steel surgery
- Simultaneous sterilization - high temperatures destroy bacteria/viruses locally
- Preservation of normal tissue - especially important in the larynx
- Non-contact - no instrument trauma to delicate structures (e.g. ossicles, vocal folds)
- Endoscopic delivery - fibre-based lasers reach previously inaccessible areas
- Office-based surgery - KTP, thulium usable in awake, unsedated patients via flexible endoscope (AULS - Awake Unsedated Laryngeal Surgery)
8. Disadvantages / Complications
- Thermal injury to adjacent normal tissue - CO₂ can damage up to 285 µm into vocal fold lamina propria causing fibrosis
- Scarring - particularly with Nd:YAG (high incidence of scar/blisters)
- Late soft tissue complications in RRP: vocal fold fibrosis, web formation, interarytenoid fibrosis, glottic stenosis (13-45% with repeated CO₂ treatments)
- Airway fire - rare but catastrophic
- Plume inhalation hazard - viral and carcinogenic particles
- Cannot distinguish carcinoma in situ from invasive (tissue still needed for histology)
- High equipment cost
Key points for exam: CO₂ = workhorse (water chromophore, precise, larynx); KTP = vascular/angiolytic + fibre delivery; Nd:YAG = deepest penetration, tracheobronchial palliation; Thulium = emerging, smallest fibre; Laser safety (airway fire prevention) is always examinable.
Radiotherapy and chemotherapy in laryngeal cancers
laryngeal cancer radiotherapy chemotherapy organ preservation guidelines
laryngeal cancer radiotherapy chemotherapy organ preservation RTOG 91-11 current guidelines 2024 2025
PMID: 34953705
Radiotherapy and Chemotherapy in Laryngeal Cancers
1. Introduction
2. Principles of Radiotherapy in Laryngeal Cancer
Why RT Works in Laryngeal Cancer
- Laryngeal SCC is radiosensitive
- Early glottic cancer: excellent blood supply, well-oxygenated - maximally radiosensitive
- No lymphatic drainage at the glottis (T1 glottic does NOT require elective nodal irradiation)
- Supraglottis: rich lymphatics - nodal fields must be included
Radiobiology - The 6 Rs
- Repair of sublethal damage (between fractions)
- Repopulation of surviving cells (accelerated RT reduces this)
- Redistribution of cells through cell cycle
- Reoxygenation of hypoxic cells
- Radiosensitivity of cells varies by histology
- Reactivation (immune)
RT Fractionation
| Scheme | Dose | Fractions | Rationale |
|---|---|---|---|
| Conventional | 66-70 Gy | 33-35 × 2 Gy/day | Standard definitive |
| Hyperfractionation | 81.6 Gy | 68 × 1.2 Gy twice daily | Improved local control (RTOG 9003) |
| Accelerated | 70-72 Gy | Compressed time | Counters tumour repopulation |
| Postoperative (PORT) | 60-66 Gy | Standard fractions | After surgery |
| PORT + high-risk | 66 Gy | + concurrent cisplatin | Positive margins, ECS |
Modern RT Technique: IMRT
- IMRT (Intensity-Modulated Radiotherapy) is the current standard of care
- Allows precise dose sculpting: high dose to tumour + nodal targets, sparing salivary glands, spinal cord, carotid arteries
- Carotid-sparing IMRT being tested in early glottic cancer to reduce long-term CVA risk
- 3D-CRT and VMAT (Volumetric Modulated Arc Therapy) are common implementations
3. Stage-Based Management
EARLY STAGE (T1-T2, N0)
T1 Glottic (Most Favourable)
- Cure rates 75-95% with either RT alone or surgery (transoral laser microsurgery)
- RT is equally effective and favoured to preserve voice in many centres
- University of Florida: RT historically treatment of choice for all T1-T2 glottic cancers
- Local control with RT: T1a ~90-95%, T1b ~85-90%
- Dose: 63-66 Gy in 28-30 fractions (2.25 Gy/fraction preferred by some to improve local control)
- Advantage of RT over TLM: Voice quality often superior (no scarring); no GA required
- Advantage of TLM over RT: Preserves RT for salvage; multiple fractions unnecessary; cost-effective
- Salvage laryngectomy is available if RT fails; ~60-80% salvage rate after RT failure
T2 Glottic
- More controversial; higher RT failure rates (~74% functional larynx preservation at MD Anderson)
- Some advocate primary surgery (partial laryngectomy/TLM) with RT reserved
- RT dose: 66-70 Gy
T1-T2 Supraglottic
- Either RT alone or conservation surgery (supraglottic laryngectomy, TLM, TORS)
- Unlike glottic cancer, bilateral elective nodal irradiation is REQUIRED due to rich lymphatics and high risk of subclinical nodal disease - this increases xerostomia risk
- Contraindications to supraglottic surgery (where RT preferred): arytenoid fixation, bilateral arytenoid involvement, cricoid/thyroid cartilage invasion, tongue base extension to circumvallate papillae, impaired cord mobility
ADVANCED STAGE (T3-T4, Any N)
4. Landmark Trials: The Evidence Base
A. VA Laryngeal Cancer Study (1991) - PIVOTAL
- Population: 332 patients, Stage III (53%) or IV (47%) laryngeal SCC
- Arms:
- Arm 1: Induction cisplatin/5-FU ×2-3 cycles → RT (66-76 Gy) [larynx preservation arm]
- Arm 2: Total laryngectomy + postoperative RT 50-74 Gy [standard arm]
- Non-responders to induction CT → underwent total laryngectomy
- 2-year survival: equivalent at 68% in both arms
- Chemotherapy response rate: 85%
- 66% of survivors in chemoRT arm had a preserved functional larynx at 2 years
- 39% of the overall group were alive at 2 years with functional larynx
B. RTOG 91-11 (2003/2013 Long-term) - DEFINING TRIAL
- Population: 547 (520 analysable) patients, Stage III/IV glottic or supraglottic SCC (T2-T4, no extension to tongue base or through cartilage)
- Three arms:
- Induction cisplatin/5-FU → RT (control arm from VA study)
- Concurrent cisplatin (100 mg/m² day 1, 22, 43) + RT (test arm)
- RT alone (control)
- Primary endpoint: Laryngectomy-Free Survival (LFS)
- Median follow-up: 10.8 years
| Outcome | RT alone | Induction → RT | Concurrent CRT |
|---|---|---|---|
| Larynx preservation | Lowest | Intermediate | Best |
| Locoregional control | Lowest | Intermediate | Best |
| LFS (HR vs RT alone) | Reference | 0.75 (p=0.016) | 0.58 (p<0.001) |
| Overall survival | Similar | Similar | Similar (no difference) |
| Grade ≥3 acute toxicity | 47% | - | 77% |
| Late sequelae | 61% | - | 82% |
- Concurrent cisplatin/RT is superior to induction CT → RT and RT alone for larynx preservation and locoregional control
- No overall survival benefit for any chemotherapy regimen vs RT alone (all three arms equivalent for OS)
- Concurrent CRT is the standard of care for organ preservation in Stage III/IV laryngeal cancer
- Significantly higher toxicity with concurrent CRT
C. RTOG 9501 and EORTC 22931 (Adjuvant CRT)
- Both Phase III trials demonstrated improved locoregional control with cisplatin + postoperative RT vs RT alone in high-risk patients after surgery
- Post-hoc analysis: Positive surgical margins and extracapsular spread (ECS) are the most important indications for adjuvant chemoradiation
- Benefit: +13% improvement in 5-year overall survival
5. Chemotherapy Regimens
Concurrent (Concomitant) Chemotherapy
- Dose: 100 mg/m² IV on days 1, 22, 43 (during RT)
- Mechanism of radiosensitization:
- Inhibits repair of sublethal radiation damage
- Preferentially kills hypoxic cells (complement to RT)
- Inhibits tumour repopulation
- Sterilizes micrometastatic disease outside RT field
- Reduces tumour mass → improved reoxygenation and drug delivery
Induction (Neoadjuvant) Chemotherapy
- Taxane-platinum combinations are superior to PF in terms of:
- Overall survival
- Progression-free survival
- Locoregional and distant failure
- But toxicity is high
- Role of induction CT remains controversial - current use is case-by-case
Adjuvant Chemotherapy
- Randomized trials do not show survival benefit for adjuvant CT alone after curative surgery/RT [Level 1 evidence]
- Therefore, adjuvant CT is not recommended as standard
Palliative / Recurrent / Metastatic Disease
- Objective response rates to methotrexate, docetaxel, paclitaxel: <20%
- Median survival in phase III trials: 5-6 months
- Pembrolizumab (anti-PD-1 checkpoint inhibitor): now FDA-approved for recurrent/metastatic HNSCC - first-line alone (PD-L1 high) or + platinum/5-FU
6. Targeted Biological Agents
Cetuximab (Anti-EGFR Monoclonal Antibody)
- Bonner et al. (2006): Landmark trial - patients with advanced oropharyngeal/laryngeal/hypopharyngeal cancer randomized to RT ± cetuximab
- Result: Cetuximab + RT significantly improved locoregional control and overall survival vs RT alone
- At 3 years: Improved locoregional control (47% vs 34%)
- RTOG 0522: RT + cisplatin vs RT + cisplatin + cetuximab → NO additional benefit from adding cetuximab to cisplatin-based CRT
- Current role: Cetuximab + RT is an option for patients unfit for cisplatin (renal impairment, hearing loss, poor PS)
7. Radiotherapy for Specific Scenarios
Post-Operative RT (PORT) Indications
- T3/T4 tumours
- N2/N3 nodal disease
- Positive or close surgical margins
- Perineural invasion
- Lymphovascular invasion
- Concurrent cisplatin added for: positive margins + ECS (highest-risk)
Subglottic Cancer
- Rare; RT principles same as glottic
- Must include paratracheal and mediastinal nodal fields
- Higher total laryngectomy rate
T4 Disease
- T4a: Total laryngectomy + PORT is recommended (French guidelines)
- Organ preservation attempted in selected T4a if no cartilage destruction or direct tongue base invasion
- T4b: Unresectable; palliative CRT
8. Side Effects
Acute (Transient)
- Mucositis (dose-limiting; grades 1-4)
- Skin reaction (erythema → moist desquamation)
- Xerostomia (saliva loss during RT)
- Dysphagia - worsened with concurrent CT
- Neutropenia, nephrotoxicity, nausea/vomiting (cisplatin)
- Grade ≥3 acute toxicity: 77% with CRT vs 47% with RT alone (RTOG 9111)
Late (Permanent/Delayed)
- Chronic xerostomia (IMRT reduces this)
- Aspiration - dysphagia, silent aspiration, aspiration pneumonia
- Neck fibrosis - especially post-surgery + RT
- Laryngeal oedema - may require tracheostomy
- Arytenoid/laryngeal chondroradionecrosis (rare, serious)
- Mandibular osteoradionecrosis (rare)
- Hypothyroidism (especially after total laryngectomy + PORT)
- Carotid artery disease/CVA - small but significant increased risk; cumulative incidence at 15 years: 2.8% (RT) vs 1.5% (surgery); ~1 excess fatal CVA per 77 patients treated
- Late sequelae: 82% CRT vs 61% RT alone (RTOG 9111)
9. Summary: Treatment by Stage
| Stage | Recommended Treatment |
|---|---|
| Tis | Endoscopic excision or RT |
| T1-T2 N0 Glottic | TLM or RT alone (equivalent) |
| T1-T2 N0 Supraglottic | Conservation surgery or RT ± elective nodal RT |
| T3 N0-N1 | Concurrent cisplatin + RT (organ preservation) or partial laryngectomy |
| T3-T4a N+, resectable | Concurrent CRT or total laryngectomy + PORT ± cisplatin |
| T4a | Total laryngectomy + PORT (± cisplatin for high-risk features) |
| T4b (unresectable) | Concurrent CRT (palliative) |
| Recurrent/metastatic | Pembrolizumab ± platinum/5-FU; palliative RT |
10. Key Points for Exam
- VA Study (1991): Induction cisplatin/5-FU → RT = equivalent OS to total laryngectomy; 66% larynx preservation. No survival advantage but established organ preservation concept.
- RTOG 91-11 (2003): Concurrent cisplatin + RT > induction CT → RT > RT alone for larynx preservation and locoregional control. No OS difference. Concurrent CRT = standard of care for advanced disease.
- Cisplatin 100 mg/m² days 1, 22, 43 = standard concurrent regimen.
- TPF > PF for induction but role of induction remains controversial.
- Cetuximab + RT = option for cisplatin-ineligible patients.
- IMRT = current RT standard; carotid-sparing reduces CVA risk.
- High-risk PORT indications: Positive margins + extracapsular spread → add concurrent cisplatin (RTOG 9501/EORTC 22931).
- Functional organ preservation ≠ preserved organ - a retained but non-functional larynx with aspiration/dysphagia is not true organ preservation.
Photodynamic therapy in ent
photodynamic therapy head neck cancer larynx ENT
photodynamic therapy ENT otolaryngology head neck cancer applications 2024 2025
photodynamic therapy larynx oral cavity nasopharynx head neck cancer
Photodynamic Therapy (PDT) in ENT
1. Definitions and Hierarchy
- Photosensitizer drug
- Light of appropriate wavelength
- Oxygen (molecular O₂)
2. Mechanism of Action
Step-by-Step Process:
- Photosensitizer administered intravenously (for head and neck cancer) or topically (for skin/oral lesions)
- Drug distributes throughout the body
- Photosensitizer preferentially accumulates in tumour tissue and is retained there longer than in normal tissue
- This selective retention is the basis of tumour specificity
- Duration: 3 to 96 hours depending on the photosensitizer used
- Target tissue irradiated with specific wavelength light matched to the photosensitizer's absorption peak
- Light delivered via: direct illumination, endoscope + optical fibres, or laser
- Photosensitizer absorbs photons → excited state
- Excited photosensitizer transfers energy to molecular oxygen
- Generates singlet oxygen (¹O₂) and other reactive oxygen species (ROS)
- Singlet oxygen damages cell membranes and intracellular organelles
- Produces cell death via:
- Direct cytotoxicity (apoptosis/necrosis)
- Vascular disruption (destruction of tumour neovasculature → ischaemia → tumour necrosis)
- Immune-mediated inflammatory response
Critical Requirement: Oxygen
- PDT is oxygen-dependent - hypoxic tumour cells are resistant
- Hypoxia is therefore a limiting factor for PDT efficacy (tumour cells cannot become immune to singlet oxygen)
3. Photosensitizers Used in ENT
First-Generation
| Agent | Details |
|---|---|
| Porfimer sodium (Photofrin®) | Most widely used; IV administration; activated at 630 nm (red light); prolonged skin photosensitivity up to 6 weeks |
| Dihematoporphyrin ether (DHE) | Early porphyrin derivative; historical use |
Second-Generation (More Selective, Less Phototoxicity)
| Agent | Details |
|---|---|
| Temoporfin (Foscan®/mTHPC) | Second-generation; extensively used for H&N cancer; activated at 652 nm; shorter drug-light interval; less skin photosensitivity |
| m-TPHC | Used in H&N cancer trials (Dilkes et al.) |
| ALA (5-Aminolevulinic acid / Levulan®) | Precursor to protoporphyrin IX (PpIX); topical or IV; activated at 635 nm; used for superficial lesions; shorter phototoxicity |
| Methyl aminolevulinate (Metvix®/Metvixia®) | Topical derivative of ALA; red light 630 nm (Aktilite lamp); actinic keratoses, BCC |
| Redaporfin | Newer agent; treatment-resistant oral cavity tumours |
| Verteporfin (Visudyne®) | Primarily ophthalmic (AMD); vascular PDT |
Key Properties of the Ideal Photosensitizer
- Selective and complete uptake by tumour (not normal tissue)
- Appropriate drug-light interval
- Activated at wavelength that penetrates tissue well (~630-800 nm: "optical window")
- No dark toxicity
- Rapid clearance from normal tissue → minimal skin phototoxicity
- Stable and easy to administer
4. Light Delivery in ENT
- Wavelength: Typically 620-680 nm (red spectrum) - this range penetrates tissue most effectively
- Light source: Laser (diode, dye laser) or LED
- Delivery methods:
- Direct illumination (oral cavity, skin)
- Optical fibres through flexible endoscope (oesophagus, larynx, nasopharynx)
- Interstitial fibres (inserted into tumour bulk for deeper lesions)
- Topical illumination (skin/mucosal surface lesions)
5. ENT-Specific Applications
A. Laryngeal Cancer
-
Biel (key series): Treated 25 patients with early squamous cell carcinoma of the larynx
- Complete response achieved in all patients
- 17 of 25 had previously failed radiotherapy - PDT worked after RT failure
- This is a major advantage: PDT efficacy is not affected by prior RT, surgery, or chemotherapy
-
Photofrin PDT: described as a "highly effective option for treating laryngeal tumours"
-
T1 and carcinoma in situ: Complete response rates comparable to standard treatments
- Preserves laryngeal structure and function (voice, swallowing)
- Can be repeated multiple times without cumulative harm
- Works after radiotherapy failure
- Endoscopic delivery via flexible scope
- Outpatient-based in selected cases
B. Oral Cavity and Oropharynx
-
Karakullukcu et al. (major series): 170 patients with early-stage oral cavity and oropharynx neoplasms
- 90% response rate
- 70% complete response (cure) rate
-
Gluckman (historical): Mixed CIS, early, and advanced H&N; oral cavity/oropharynx gave best results:
- 11/13 complete response; 2/13 partial response
- 4 recurrences within 1 year
- Advanced tumours: palliation only; results comparable to standard regimes
-
Biel (pooled summary of 217 patients, early SCC of H&N with PDT):
- 194/217 (89%) complete response
- 23/217 (10.6%) partial response
- 0% failure to respond (every patient showed some response)
-
Oral premalignancy (leukoplakia, erythroplakia):
- PDT can treat widespread premalignant conditions - important given field cancerization concept
- ALA and topical photosensitizers used for superficial lesions
-
5-ALA PDT + platinum-based induction CT: 90.9% overall response rate in locally advanced oral SCC (Wang et al.)
C. Nasopharynx
- Lofgren et al.: 5 patients with circumscribed nasopharyngeal carcinoma
- Drug activated with laser under topical anaesthesia
- 3/5 patients had no evidence of disease at 4 years
- Temoporfin (Foscan®) PDT: Used for recurrent/residual NPC after conventional treatment
- Successful management as palliative measure
- NPC lesions <10 mm depth respond well
- Phase II trials confirm efficacy for persistent/recurrent NPC
D. Oesophagus (Upper Aerodigestive Tract - Relevant to ENT)
- Palliative: Phase II trial (218 patients) - PDT (porfimer sodium) vs Nd:YAG laser ablation
- Equivalent dysphagia improvement
- Fewer perforations with PDT (1% vs 7%, p<0.05) - key safety advantage
- Barrett's with high-grade dysplasia/adenocarcinoma: 43/55 patients had complete ablation at 6 months; but oesophageal stricture in 53% - significant complication
E. Sinonasal
- Inverted papilloma of sinonasal cavity: PDT has been targeted
- Chronic rhinosinusitis (CRS): In vitro and animal studies show PDT reduces Staphylococcus and Pseudomonas biofilms by 99.9% after a single exposure
- However: No human studies exist - no recommendation for routine use (insufficient evidence)
F. Skin / Cutaneous ENT Lesions
- FDA-approved for non-hypertrophic actinic keratoses (face/scalp)
- Used for superficial BCC (basal cell carcinoma) and Bowen's disease
- ALA (Levulan Kerastick): 30-minute incubation → light activation → selective apoptosis of atypical cells
- Particularly useful for ill-defined, multifocal superficial lesions on a background of actinic damage
6. Dilkes et al. (Multi-site H&N Experience)
- Used m-TPHC, Photofrin II, and ALA for squamous carcinoma at multiple head and neck sites
- Treated palliative, primary, and adjunctive forms
- Visible response in nearly all cases
- Complications: local pain at injection site; post-treatment skin photosensitivity (when precautions not taken)
7. Advantages of PDT in ENT
- Selective tumour destruction - photosensitizer retained longer in tumour → reduced normal tissue damage
- Organ and function preservation - structure maintained; voice/swallowing preserved
- Repeatable - can be performed multiple times without cumulative harm (unlike RT)
- Not affected by prior treatment - works after RT, surgery, or chemotherapy failure
- No ionizing radiation
- Minimal systemic toxicity - localised action
- Endoscopic delivery - accessible sites via fibres
- Cells cannot develop resistance to singlet oxygen - unlike chemotherapy resistance
- Outpatient potential - some protocols are office-based
- Dual action: both direct cytotoxicity and vascular disruption
8. Disadvantages and Limitations
- Limited tissue penetration depth (~5-10 mm) - inadequate for bulky/deep tumours; unsuitable for T3/T4 without interstitial delivery
- Skin phototoxicity - major problem; porfimer sodium causes photosensitivity for up to 6 weeks; patient must avoid daylight during and after treatment
- Oxygen dependence - ineffective in hypoxic tumour regions
- Not absolutely tumour-specific - post-PDT specimens show necrosis in tissues beyond the tumour boundary
- Oesophageal stricture - significant complication in 53% of Barrett's/oesophageal patients
- Not widely available - specialized equipment and expertise required
- Uncertainty - optimal photosensitizer, drug-light interval, light dose, and treatment schedule not yet standardized for most ENT indications
- Limited evidence base - most studies are small case series; few randomized trials
9. Current Status and Future Directions
- Current role in ENT: Primarily for early-stage, superficial lesions of larynx, oral cavity, and nasopharynx, and for salvage after RT failure
- Field cancerization advantage: ENT mucosal surface shares common carcinogenic exposure - PDT can treat widespread premalignant change across multiple sites simultaneously
- Endoscopic access makes upper aerodigestive tract ideal for PDT delivery
- Determining optimal photosensitizer-disease combinations
- Role as primary, adjunctive, or palliative therapy
- Nanoparticle-based photosensitizers - improved tumour targeting, deeper penetration
- Photochemical internalization (PCI) - enhanced drug delivery into cells
- Photoimmunotherapy - combining PDT with immune checkpoint activation
- PDT + chemotherapy combinations (5-ALA + platinum: 90.9% response in oral SCC)
- Biofilm eradication in CRS - awaiting human trials
Key points from Scott-Brown's: "PDT requires administered drug, light and oxygen." "Skin phototoxicity and limited tissue penetration are the current PDT shortcomings." "PDT has a future place in head and neck cancer management."
Premalignant lesions of larynx and their treatment
laryngeal premalignant lesions dysplasia management treatment
laryngeal premalignant lesions leukoplakia dysplasia classification treatment guidelines 2024 2025
PMID: 37030937
Premalignant Lesions of the Larynx and Their Treatment
1. Definition and Significance
- Incidence: 2-10 per 100,000 population
- Male predominance (M:F = 8:1)
- Peak age: 50-70 years
- Malignant transformation rates: 11-25% overall
- 30% of patients with dysplastic lesions that progress to invasive cancer eventually require total laryngectomy
2. Aetiology and Risk Factors
| Risk Factor | Details |
|---|---|
| Smoking (most important) | Dose-dependent; carcinogens in tobacco smoke cause direct mucosal damage |
| Alcohol | Synergistic with smoking; multiplicative risk |
| Laryngopharyngeal reflux (LPR) | Acid/pepsin causes posterior laryngeal mucosal injury |
| HPV (types 16, 18) | Less important in glottis than oropharynx; HPV-associated dysplasia tends to be non-keratinizing |
| Occupational | Asbestos, dust, chemical exposure |
| Voice abuse | Chronic irritation |
| Chronic laryngitis | Perpetuates epithelial change |
3. Clinical Presentation
- Hoarseness (most common; any hoarseness >3 weeks must be investigated)
- Dysphonia
- Throat irritation / chronic cough
- Often asymptomatic - discovered incidentally
| Type | Appearance | Risk |
|---|---|---|
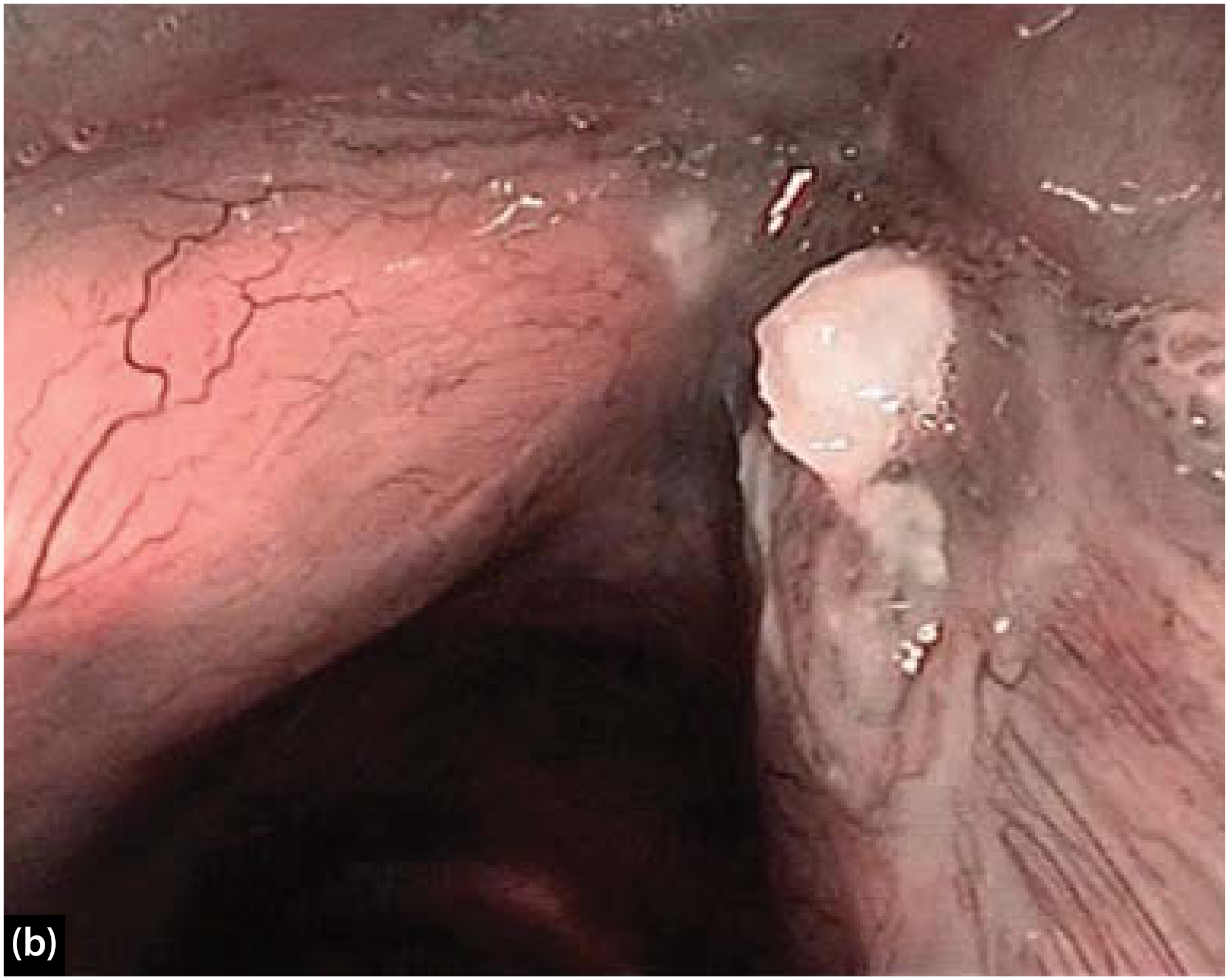
| Leukoplakia | White patch/plaque (keratin production, abnormal for laryngeal squamous epithelium) | Variable |
| Erythroplakia | Red, velvety patch (enhanced vascularity) | High risk - despite less visually impressive |
| Leukoerythroplakia / speckled | Mixed red and white | Intermediate-high |
Key point: Erythroplakia, despite appearing less dramatic, has a much higher probability of representing severe dysplasia/CIS than leukoplakia. The extent of keratinization does not correlate with the degree of underlying dysplasia.
- Erythroplakia or speckled pattern
- Surface granularity
- Large surface area
- Irregular margins
- Rapid growth
- Firmness/induration (suggests invasive change)
4. Histopathological Classification
WHO 2017 Classification (4th Edition, Head and Neck Tumours) - Current Standard
| Grade | Old Terminology | Features |
|---|---|---|
| Low-grade SIL (Low-grade dysplasia) | Mild dysplasia, squamous hyperplasia | Relatively low malignant potential |
| High-grade SIL (High-grade dysplasia) | Moderate dysplasia, severe dysplasia, CIS | High-risk premalignant lesion |
Morphological Criteria (WHO/Cummings Table 105.2):
- Stratification preserved; augmentation of basal/parabasal cells in the lower half of epithelium only
- Minimal cellular atypia; slightly enlarged nuclei, uniformly distributed chromatin
- Rare mitoses near basal layer only; few dyskeratotic cells
- Immature epithelial cells occupying lower half to full epithelial thickness
- Abnormal maturation; disordered stratification and polarity
- Conspicuous cellular and nuclear atypia
- Increased N:C ratio
- Mitoses at or above suprabasal layer with or without atypical forms
- Basement membrane intact (distinguishes from invasive carcinoma)
Historical Classification Systems (for comparison)
| System | Categories |
|---|---|
| WHO 1978 (SIN) | SIN I (mild), SIN II (moderate), SIN III (severe dysplasia/CIS) |
| Kleinsasser (1963) | Hyperplasia without atypia → moderate/severe → carcinoma in situ |
| Ljubljana Classification | Basal/parabasal hyperplasia (low risk) vs. atypical/risky hyperplasia (high risk) |
5. Malignant Transformation Rates
| Histology | Malignant Transformation Rate |
|---|---|
| No dysplasia (leukoplakia only) | 3.8% |
| Mild to moderate dysplasia | 10.1% |
| Severe dysplasia / CIS | 18.1% |
| Overall (meta-analysis) | 14% |
| Mean time to malignant transformation | Variable; years |
Important: Even lesions without dysplasia carry a 3.8% risk of cancer → long-term follow-up is warranted for ALL laryngeal premalignant lesions.
6. Investigations
Essential
- Flexible laryngoscopy - office-based; assess lesion morphology, vocal cord mobility, extent
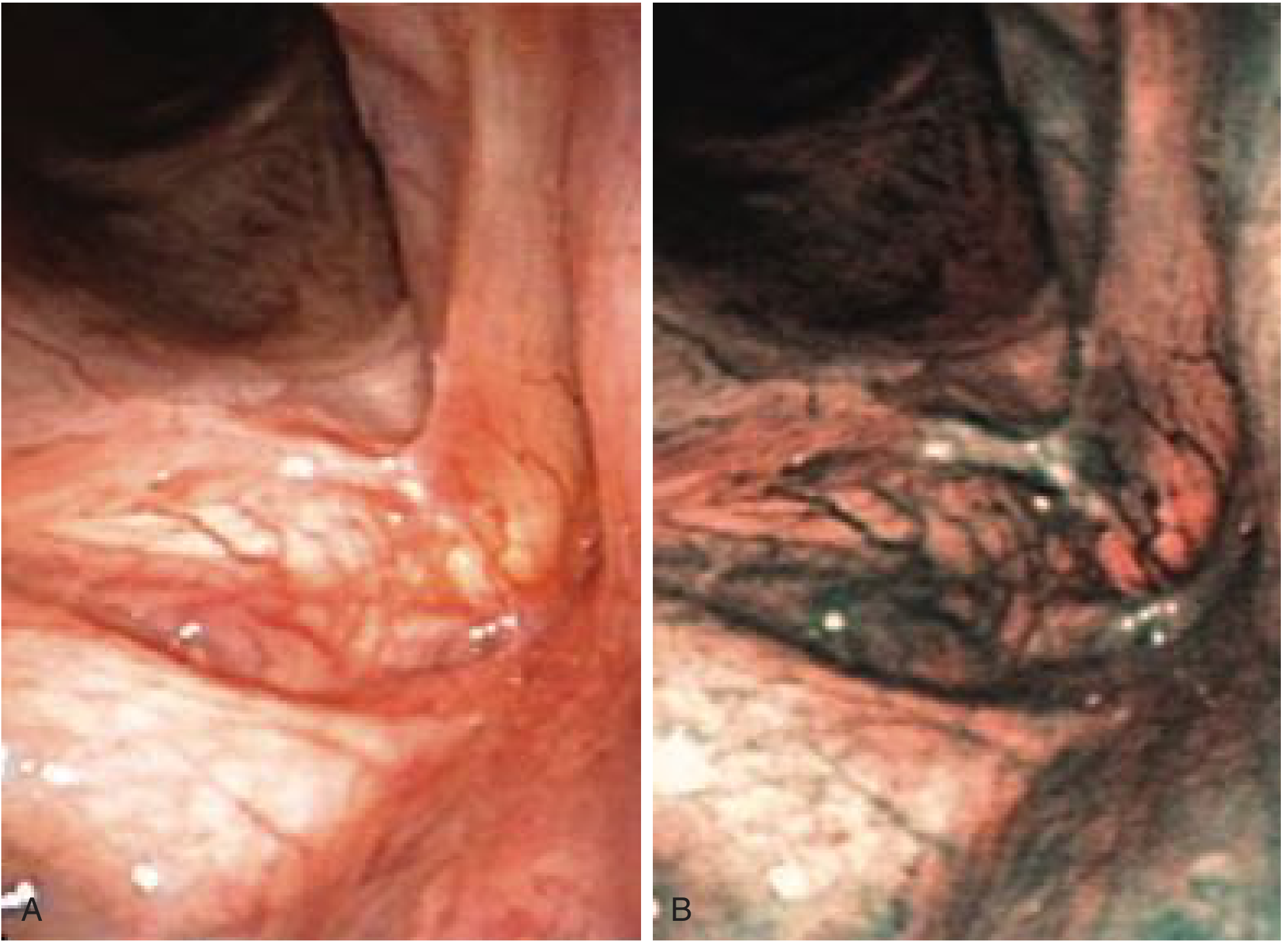
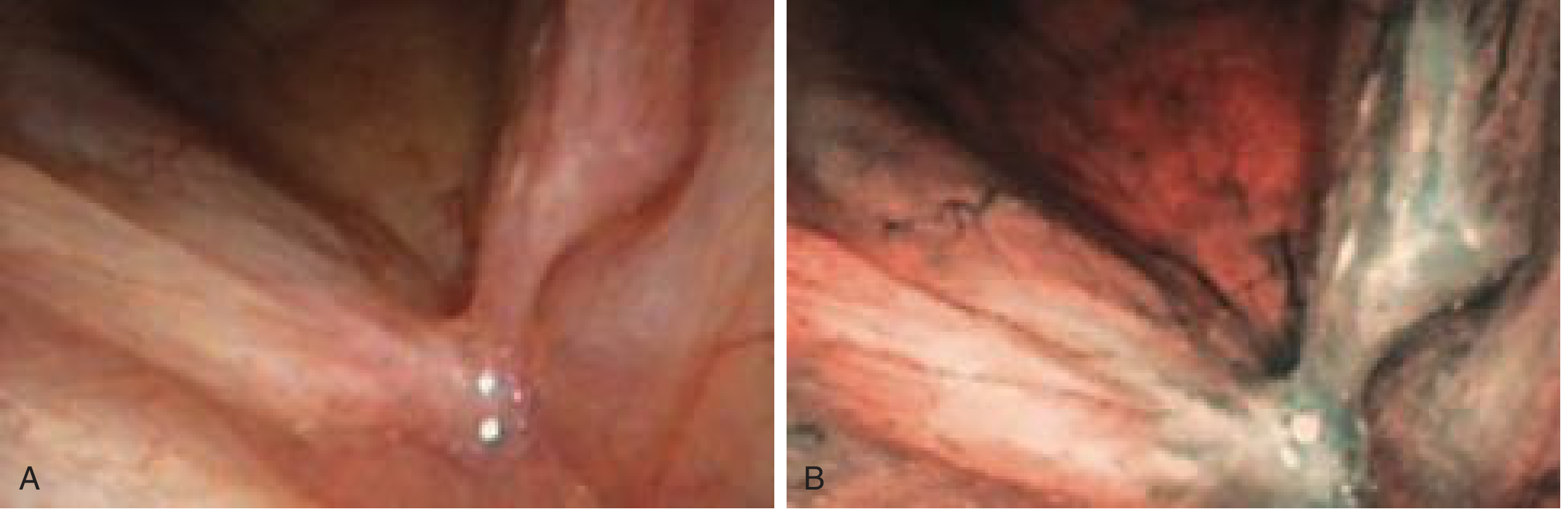
- Advanced imaging - NBI (Narrow-Band Imaging): Maps IPCL pattern; guides biopsy to highest-risk areas; distinguishes benign from malignant vascular patterns
- Microlaryngoscopy under GA - direct visualization + biopsy (gold standard for diagnosis)
- Biopsy / excision biopsy (histopathology) - mandatory; diagnosis and treatment often combined in one procedure
Additional
- Contact endoscopy - cellular architecture assessment in vivo
- Stroboscopy - assess mucosal wave (invasion of lamina propria reduces/abolishes wave)
- CT/MRI neck - only if invasive carcinoma suspected (cartilage involvement, nodal disease)
7. Treatment
Principles
Risk Factor Modification (All Patients)
- Smoking cessation - mandatory counselling; smoking is the dominant risk factor and continued smoking reduces treatment efficacy
- Anti-reflux measures for symptomatic LPR - lifestyle modification, PPI therapy
- Alcohol reduction
A. Surgical Excision (First-Line for Most Lesions)
| Method | Details |
|---|---|
| Cold steel (cup forceps/microscissors) | Precise microflap technique; no thermal artifact on specimen; preferred for accurate histological assessment |
| CO₂ laser excision (TLM) | Excellent haemostasis; precise; most widely used laser; risk of thermal artifact on margins |
| KTP/Thulium laser (angiolytic) | Fibre-based; AULS possible; preserves layered microstructure; angiolytic ablation promotes normal re-epithelialization |
- Specimens must be mounted, orientated, and presented on an anatomical template to the pathologist for accurate margin assessment
- Vocal cord stripping is NOT recommended - high risk of permanent voice damage (destroys superficial lamina propria)
- Ablation without excision (laser vaporization) is discouraged - no specimen available for diagnosis and higher risk of voice damage
- Excision in the subepithelial plane (preserve SLP/Reinke's space whenever possible)
- Type I (subepithelial): Superficial dysplasia
- Type II (subligamental): Extends to vocal ligament
- Type III (transmuscular): Extends to vocalis muscle (for high-grade dysplasia approaching Tis/T1)
B. Awake Unsedated Laryngeal Surgery (AULS) - Modern Paradigm
- KTP or Thulium laser via flexible laryngoscope, office-based, no GA required
- Angiolytic laser energy absorbed by microcirculation → lesion ablation with maximal preservation of layered microstructure
- Allows small biopsies + ablation in same sitting
- Angiolytic epithelial ablation promotes re-epithelialization of laryngeal mucosa toward normal
- Avoids: repeated GA, permanent voice impairment from multiple biopsies, cumulative mucosal scarring
"A paradigm shift from the traditional 'wait and see' approach, where periodic microlaryngoscopies under GA with biopsies cumulatively destroy the voice in managing benign disease." - Scott-Brown's HNS, p. 1160
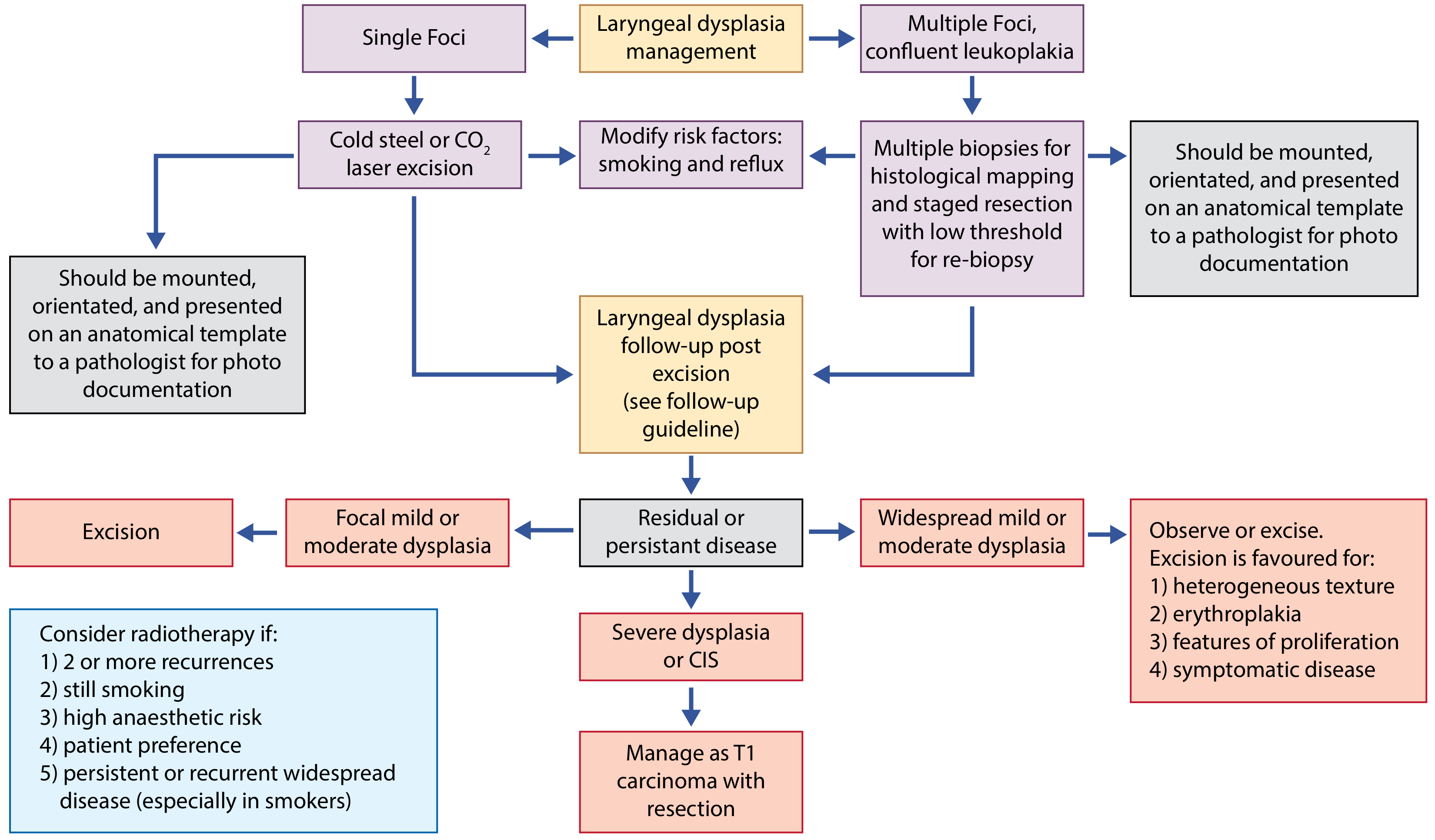
C. Management Algorithm (BAO-HNS / Cosway & Paleri)
- Single focus → Cold steel or CO₂ laser excision
- Multiple foci or confluent leukoplakia → Multiple biopsies for mapping → Staged resection
- All excised specimens → Mounted, orientated on anatomical template → Pathologist
- Focal mild/moderate dysplasia → Re-excision
- Widespread mild/moderate dysplasia → Observe OR excise (excision favoured if: heterogeneous texture, erythroplakia, proliferative features, symptomatic)
- Severe dysplasia/CIS → Manage as T1 laryngeal carcinoma with surgical resection (cordectomy type II/III) ± RT
D. Radiotherapy
- Two or more recurrences after excision
- Still smoking (continued risk)
- High anaesthetic risk (cannot safely undergo GA)
- Patient preference
- Persistent or recurrent widespread disease (especially in smokers)
- Severe dysplasia/CIS where surgical resection not feasible
Note: RT should be offered "only in rare circumstances for patients where there is very high risk/suspicion of conversion to malignancy and surgical resection is not possible." - Scott-Brown's HNS
8. Follow-Up (Cosway & Paleri Protocol)
- 3-monthly flexible laryngoscopy × 1 year
- 6-monthly × 2 years
- Annual thereafter × 5 years minimum
- More frequent review (every 6-8 weeks initially)
- Lower threshold for re-biopsy
- Long-term surveillance
- Recurrence and progression to cancer
- Voice outcomes (patient-reported voice questionnaire, e.g. VHI)
9. Summary Table: Malignant Transformation Risk and Management
| Histology | Transformation Risk | Management |
|---|---|---|
| Hyperplasia/keratosis, no dysplasia | 3.8% | Risk factor modification; surveillance |
| Low-grade dysplasia | ~10% | Excision; risk factor modification |
| High-grade dysplasia | ~18% | Excision (cordectomy if needed); MDT |
| CIS (Tis) | High; ~20-30% progress | TLM cordectomy or RT |
| Invasive carcinoma | N/A | Treat as T1/T2 laryngeal SCC |
Key exam point: "A binary grading system for laryngeal dysplasia is currently espoused. Management of laryngeal precancer is driven by consensus as high-level evidence is lacking." - Scott-Brown's HNS Key Points
Leukoplakia, erythroplakia, keratosis of larynx
laryngeal leukoplakia keratosis erythroplakia malignant transformation treatment
laryngeal leukoplakia erythroplakia keratosis classification pathology treatment 2024 2025
Leukoplakia, Erythroplakia and Keratosis of the Larynx
1. Definitions
Leukoplakia
- Etymology: Greek - "leuko" (white) + "plakia" (plaque)
- WHO 1978 definition: "A white patch or plaque that cannot be characterised clinically or pathologically as any other disease"
- A purely descriptive/clinical term - it says nothing about the underlying histology
- Implies the white patch cannot be wiped off (distinguishing it from candidiasis, which can be scraped away)
- Represents a broad spectrum from benign hyperkeratosis to frank carcinoma
Erythroplakia
- Etymology: Greek - "erythro" (red) + "plakia" (plaque)
- A red, velvety patch on the laryngeal mucosa
- Much less common than leukoplakia but carries significantly higher risk of severe dysplasia/CIS
- Red appearance results from increased vascularity, mucosal thinning, and subepithelial haemorrhage
- Often seen alongside leukoplakia as erythroleukoplakia (speckled lesion) - the highest risk clinical presentation
Keratosis (Laryngeal Hyperkeratosis)
- A histological and clinical term referring to abnormal keratin production by the normally non-keratinizing squamous epithelium of the vocal cords
- "An inflammatory disease of the epithelium of the vocal cords due to chronic hyperplasia and hyperkeratosis of the laryngeal mucosa" - Scott-Brown's HNS, p. 999
- Terminology is interchangeable with leukoplakia in many clinical contexts - the white appearance of leukoplakia is caused by keratosis
- Key point: Keratosis ≠ dysplasia; the two can exist together or separately; the degree of keratinization does not predict the degree of dysplasia
The relationship: Keratosis is what causes the white appearance of leukoplakia. A leukoplakic lesion is white because the epithelium is keratinizing. However, keratosis can exist without dysplasia (benign hyperkeratosis) or alongside any grade of dysplasia up to CIS.
2. Normal Laryngeal Epithelium
| Location | Normal Epithelium |
|---|---|
| True vocal cords (free edge) | Stratified squamous, non-keratinizing |
| Supraglottis / epiglottis | Pseudostratified ciliated columnar (respiratory) |
| Subglottis | Ciliated columnar transitioning to squamous |
| Trachea | Pseudostratified ciliated columnar |
3. Macroscopic Appearances and Clinical Morphology

| Type | Appearance | Surface | Risk Level |
|---|---|---|---|
| Thin/smooth leukoplakia | Flat white film | Smooth, regular | Low |
| Thick/rough leukoplakia | Raised white plaque | Irregular, rough, granular | Intermediate |
| Confluent leukoplakia | Widespread white covering | May cross AC | Intermediate-high |
| Erythroplakia | Red, velvety | Smooth to granular | High |
| Erythroleukoplakia (speckled) | Mixed red and white | Heterogeneous | Highest |
| Verrucous/exophytic | Warty white proliferation | Papillomatous | Suspicious for verrucous Ca |
| Proliferative/infiltrative | Nodular mass | Irregular | Carcinoma until proven otherwise |
Key exam point (Scott-Brown's): "Clinically abnormal areas in the larynx do not always exhibit histopathological evidence of LD, and LD can be detected under the microscope in clinically normal appearing epithelium." - Scott-Brown's HNS, p. 284
4. Histological Spectrum
| Histology | What it means | Malignant transformation risk (3 years) |
|---|---|---|
| Squamous hyperplasia (simple keratosis) | Thickened squamous epithelium, normal maturation, NO dysplastic features | ~3.8% |
| Hyperkeratosis | Excess surface keratin (orthokeratosis or parakeratosis), ordered cellular maturation | ~3.8% |
| Parakeratosis | Retained nuclear remnants in surface keratin layer (nucleated keratinocytes at surface) | Low-moderate |
| Low-grade dysplasia (WHO 2017 Low-SIL) | Architectural/cytological atypia in lower half of epithelium | ~10% |
| High-grade dysplasia (WHO 2017 High-SIL) | Atypia extending to upper half or full thickness | ~18% |
| Carcinoma in situ (CIS/Tis) | Full-thickness atypia, intact basement membrane | High; imminent invasion |
| Invasive SCC | Basement membrane breached | Malignancy |
Histological subtypes of keratosis:
- Orthokeratosis - surface keratin layer composed of anucleate squames (cells without nuclei); more organized
- Parakeratosis - surface keratin layer retains nuclei; often indicates a more reactive/dysplastic process
- In contact endoscopy: keratosis appears as amorphous or laminar structure where individual cells cannot be identified (their nuclei have been lost or are obscured by keratin)
5. Keratosis as Seen by Contact Endoscopy
- Keratosis appears as areas of amorphous (no structure) or laminar (layered) pattern at ×60 or ×150
- Individual cells cannot be distinguished in these areas because nuclei are absent (hyperkeratosis) or obscured
- In the same lesion or same patient, keratosis and dysplasia can coexist
- Vessels in leukoplakic lesions may pass below the keratotic area (normal pattern) or may surround the leukoplastic lesion (more concerning)
- Keratosis is also found in chronic inflammation, papillomas, and tumours
6. Why Erythroplakia is Higher Risk
- Leukoplakia is white because keratin is thick and obscures the underlying mucosa - the cell surface maturation may actually be relatively preserved (hyperkeratosis)
- Erythroplakia is red because the epithelium is thin (atrophic) and highly dysplastic/undifferentiated; without keratin protection, abnormal vascularity shows through
- Atrophic dysplastic epithelium lacks the surface keratin layer → undifferentiated cells predominate, more aggressive dysplastic/CIS features
- NBI confirms this: erythroplakia shows type III/IV IPCL changes (dilated, tortuous, abnormal angiogenesis) more consistently than thick leukoplakia
In practical terms: a thin, red patch on the vocal cord is more worrying than a thick white plaque.
7. The Keratosis-Dysplasia Relationship
| Feature | Keratosis | Dysplasia |
|---|---|---|
| Definition | Abnormal keratin production | Abnormal cellular/architectural maturation |
| Can exist alone? | Yes (benign hyperkeratosis without dysplasia) | Yes (dysplasia without surface keratosis - e.g. erythroplakia) |
| Can coexist? | Yes - commonly | Yes - commonly |
| Correlated? | NOT correlated - the amount of keratosis does NOT predict the grade of dysplasia | - |
| Clinical implication | A thick, obviously keratotic leukoplakia may be benign; a thin patch may be CIS | Always biopsy; clinical appearance is unreliable |
8. Differential Diagnosis of White Laryngeal Lesions
| Condition | Key differentiator |
|---|---|
| Candidiasis | Can be wiped off; immunocompromised; responds to antifungals; culture positive |
| Mucus | Transient; clears with swallowing/coughing |
| Vocal cord polyp/nodule | Bilateral (nodules), unilateral (polyp); glassy/translucent; stroboscopy shows normal mucosal wave at base |
| Reinke's oedema | Bilateral, fusiform, gelatinous appearance; smokers |
| RRP (Recurrent Respiratory Papillomatosis) | Multiple exophytic frond-like lesions; HPV-positive |
| Verrucous carcinoma | Exophytic, warty; locally aggressive SCC variant; slow growing; needs complete excision |
| Early invasive SCC | Proliferative or infiltrative; vocal cord fixity; NBI shows severe IPCL changes |
| Granuloma | Posterior glottis/arytenoid contact area; intubation/reflux history |
9. Stroboscopy in Leukoplakia Assessment
- Normal mucosal wave preserved = surface lesion only, SLP (superficial lamina propria) uninvolved → reassuring
- Reduced/absent mucosal wave = invasion of SLP or deeper structures → raises suspicion of invasive carcinoma despite apparently superficial appearance
- Vocal cord fixity = deep muscular/cartilage invasion or cricoarytenoid joint involvement → T3/T4 features
10. Investigations Summary
- Flexible nasolaryngoscopy (clinic) - first line; document with video recording and photography; NBI mode
- NBI evaluation - IPCL pattern assessment; grade I-II (benign) vs III-IV (suspicious/malignant)
- Stroboscopy - mucosal wave assessment
- CT neck and chest - only if invasive malignancy is suspected (vocal cord fixity, subglottic extension, nodal disease); LDCT chest for smoking-related second primaries
- Microlaryngoscopy under GA + biopsy - mandatory for histological diagnosis; excision biopsy preferred (therapeutic and diagnostic simultaneously); specimen must be mounted and orientated on anatomical template
11. Practical Management Points
- All white/red lesions of the larynx = biopsy until proven otherwise
- Leukoplakia that cannot be assigned a definitive benign diagnosis clinically requires histological assessment
- The aim at microlaryngoscopy is excision rather than punch biopsy alone - this serves as diagnosis and treatment
- Vocal cord stripping is absolutely contraindicated - destroys SLP irreversibly
- Risk factor modification (smoking cessation, anti-reflux) is part of treatment for all patients
- Even after histologically benign keratosis/hyperplasia, long-term surveillance is mandatory because the 3.8% 3-year transformation rate is not negligible and continued smoking perpetuates new lesion development