Spirometry full details for md exam answer 15 marks
With graphs
Reading File
Finding Sources
Searching Images
spirometry lung volumes flow volume loop graph
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Searching Images
spirometry volume time curve FVC FEV1 obstructive restrictive pattern
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Searching Images
lung volumes diagram spirogram tidal volume IRV ERV residual volume FRC
Loading Image
Reading File
Finding Sources
I now have comprehensive data to write a full 15-mark MD exam answer on spirometry with graphs. Let me compile everything.
SPIROMETRY — Complete MD Examination Answer (15 Marks)
Definition
Spirometry is the measurement of the volume of air inhaled or exhaled as a function of time. It is performed using a pneumotachometer that measures flow rates and integrates them to obtain volume, making it the most commonly used, standardised pulmonary function test.
— Murray & Nadel's Textbook of Respiratory Medicine
Lung Volumes & Capacities (Static)
Before interpreting spirometry, understanding the subdivisions of lung volume is essential.
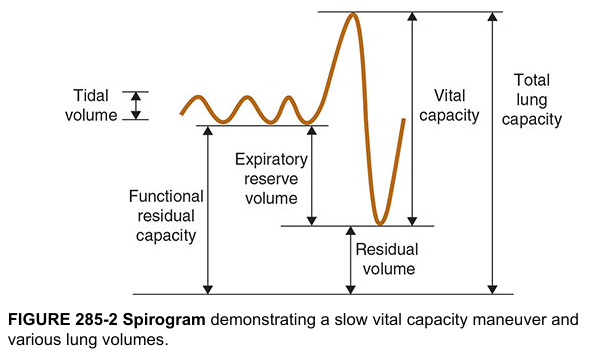
Four Primary Lung Volumes (non-overlapping):
| Volume | Definition | Normal Value |
|---|---|---|
| Tidal Volume (TV) | Volume inhaled/exhaled during each quiet respiratory cycle | ~500 mL |
| Inspiratory Reserve Volume (IRV) | Maximal extra volume inspired from end of tidal inspiration | ~3000 mL |
| Expiratory Reserve Volume (ERV) | Maximal volume exhaled from end of tidal expiration | ~1200 mL |
| Residual Volume (RV) | Volume remaining after maximal exhalation (cannot be measured by spirometry alone) | ~1200 mL |
Four Lung Capacities (each = sum of ≥2 volumes):
| Capacity | Components | Normal Value |
|---|---|---|
| Total Lung Capacity (TLC) | TV + IRV + ERV + RV | ~6000 mL |
| Vital Capacity (VC) | TV + IRV + ERV | ~4800 mL |
| Inspiratory Capacity (IC) | TV + IRV | ~3500 mL |
| Functional Residual Capacity (FRC) | ERV + RV | ~2400 mL |
Note: RV, FRC, and TLC cannot be measured by spirometry alone — they require nitrogen washout, helium dilution, or body plethysmography.
Spirometric Measurements (Dynamic Volumes)
Key Parameters
| Term | Definition |
|---|---|
| FVC (Forced Vital Capacity) | Total volume exhaled forcefully from full inspiration |
| FEV₁ | Volume exhaled in the first second of a forced expiration |
| FEV₁/FVC ratio | Proportion of FVC expelled in 1 second (≥0.70 normal) |
| FEF₂₅₋₇₅% | Average mid-expiratory flow between 25–75% of FVC; reflects small airway function |
| PEFR | Peak expiratory flow rate |
| FEV₆ | Volume exhaled in 6 seconds; approximates FVC |
| MVV | Maximal voluntary ventilation — maximal air moved in 1 minute (~FEV₁ × 40) |
The Volume–Time Curve (FVC Curve)
The subject:
- Inhales maximally to TLC
- Exhales as forcefully and rapidly as possible
Volume (y-axis) is plotted against Time (x-axis).
Graph: Normal vs. Obstructive Pattern
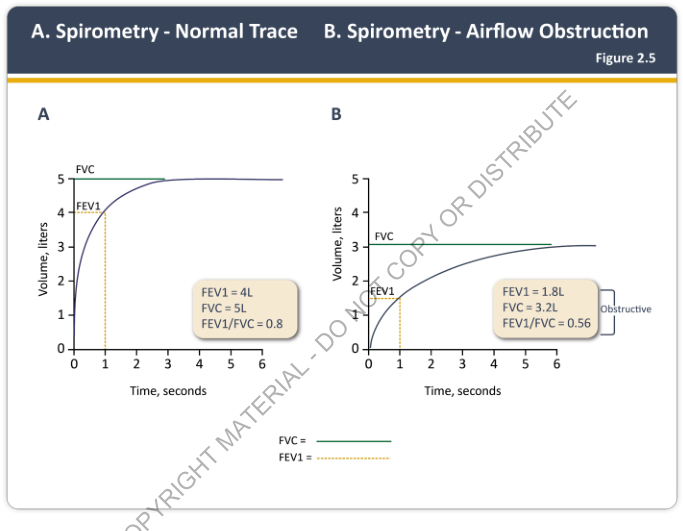
| Normal | Obstructive | |
|---|---|---|
| FEV₁ | 4 L | 1.8 L |
| FVC | 5 L | 3.2 L |
| FEV₁/FVC | 0.80 | 0.56 |
In obstruction, the curve rises slowly and plateaus late; FEV₁ is disproportionately reduced.
Spirogram Patterns — Normal, Obstructive, Restrictive
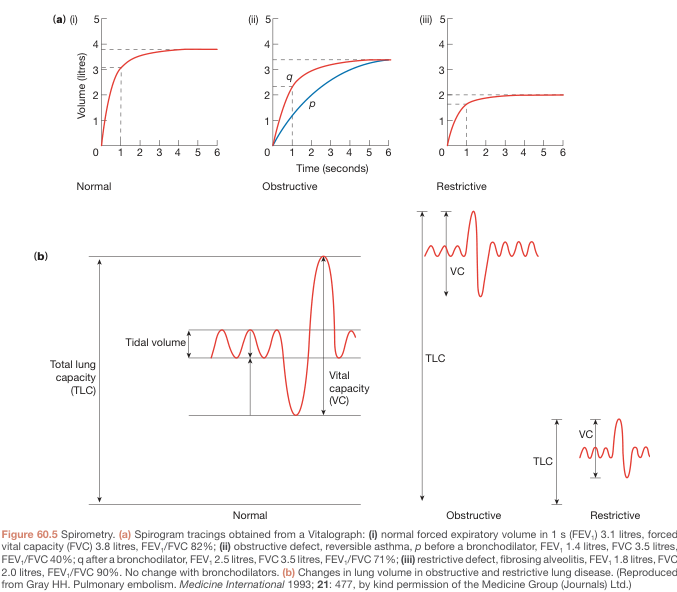
(a) Volume–Time Spirograms
(i) Normal: Rapid rise, plateau at ~3.8–4 L by 2 seconds. FEV₁/FVC ≈ 80%
(ii) Obstructive (e.g., asthma, COPD): Slow rise, plateau reached late. FEV₁ markedly reduced. FEV₁/FVC < 70%. Post-bronchodilator improvement shown by shift from curve p → q.
(iii) Restrictive (e.g., fibrosis, pleural effusion): Rapid rise but low plateau (~2 L). FEV₁ reduced, but FEV₁/FVC normal or elevated (both volumes proportionally reduced).
(b) Changes in Lung Volumes
| Normal | Obstructive | Restrictive | |
|---|---|---|---|
| VC | Normal | ↓ (air trapping) | ↓↓ |
| TLC | Normal | ↑ (hyperinflation) | ↓↓ |
| RV | Normal | ↑↑ | ↓ |
| FEV₁ | Normal | ↓↓ | ↓ |
| FEV₁/FVC | ≥0.70 | < 0.70 | Normal/↑ |
The Flow–Volume Loop
Most informative for upper airway obstruction and central airway lesions. Plots flow (y-axis) vs. volume (x-axis) during a maximal inspiratory and expiratory manoeuvre.
Shape characteristics:
- Expiratory limb (upper): Rises rapidly to peak flow (effort-dependent initial portion), then descends linearly and effort-independently to RV
- Inspiratory limb (lower): Semicircular, entirely effort-dependent
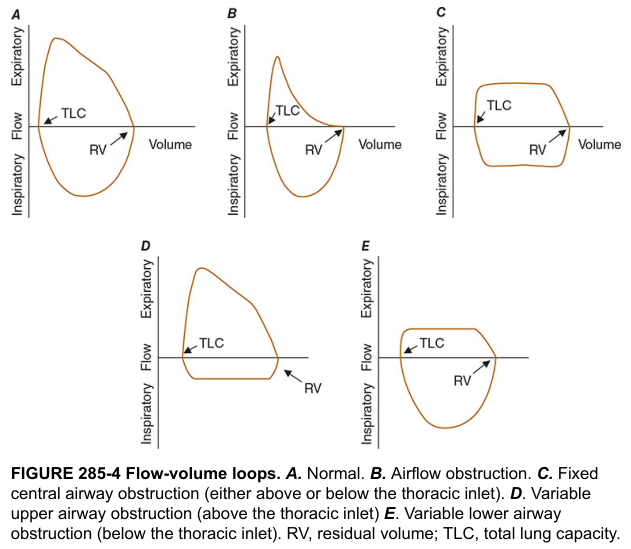
| Pattern | Shape | Cause |
|---|---|---|
| A — Normal | Broad rounded expiratory, symmetric inspiratory | — |
| B — Airflow obstruction | Scooped/concave expiratory limb (↓ flow at low volumes) | COPD, emphysema, asthma |
| C — Fixed central obstruction | Both expiratory and inspiratory limbs flattened ("box-shaped") | Tracheal stenosis, goitre |
| D — Variable extrathoracic (upper airway) | Inspiratory limb flattened only | Vocal cord paralysis, tracheomalacia above thoracic inlet |
| E — Variable intrathoracic | Expiratory limb flattened only | Tracheomalacia below thoracic inlet |
Interpretation Algorithm
Step 1: Check FEV₁/FVC ratio
- < 0.70 (or < LLN) → Obstructive pattern → proceed to Step 2
- ≥ 0.70 → Go to Step 3
Step 2: (Obstructive) — Check FVC
- FVC normal → Simple obstruction
- FVC also low → Obstruction + air trapping or mixed pattern
Step 3: (Non-obstructive) — Check FVC
- FVC reduced (< 80% predicted), normal ratio → Restrictive pattern (confirm with TLC)
- Both normal → Normal spirometry
Step 4: Severity (GOLD classification for obstruction, post-bronchodilator FEV₁%)
| GOLD Grade | FEV₁ % predicted | Severity |
|---|---|---|
| 1 | ≥ 80% | Mild |
| 2 | 50–79% | Moderate |
| 3 | 30–49% | Severe |
| 4 | < 30% | Very severe |
Bronchodilator Reversibility Testing
- Administer short-acting bronchodilator (salbutamol 400 µg)
- Repeat spirometry after 15–20 minutes
- Positive reversibility = FEV₁ increase ≥ 12% AND ≥ 200 mL from baseline
- Suggests asthma (vs. fixed obstruction in COPD)
- Requires: LABAs withheld ≥12 h, SABAs withheld ≥6 h before test
Indications for Spirometry
- Diagnostic — suspected asthma, COPD, pulmonary fibrosis, occupational lung disease
- Monitoring — disease progression (e.g., serial FVC in IPF predicts survival)
- Pre-operative assessment — especially lung resection surgery
- Disability/legal evaluation — quantifying impairment
- Occupational screening — hazardous environments
- Assessing treatment response — bronchodilators, steroids
Acceptability & Reproducibility Criteria (ATS/ERS)
- Minimum 3 acceptable manoeuvres
- Best 2 FVC values within 150 mL of each other
- Best 2 FEV₁ values within 150 mL
- No cough, glottis closure, or early termination
- Initial 25–30% of curve is effort-dependent; remainder is effort-independent
Conditions Causing Each Pattern
| Obstructive | Restrictive |
|---|---|
| Asthma | Pulmonary fibrosis (IPF) |
| COPD / Emphysema | Sarcoidosis |
| Bronchiectasis | Pleural effusion |
| Cystic fibrosis | Kyphoscoliosis |
| Obliterative bronchiolitis | Neuromuscular disease |
| Pneumonectomy |
FEF₂₅₋₇₅% (Forced Mid-Expiratory Flow)
- Reflects small airway (peripheral airway) function
- More sensitive for early obstructive disease than FEV₁
- Limitation: Wide 95% CI in normal populations → poor specificity; high false-positive and false-negative rates
- Less reproducible than FEV₁
Maximal Voluntary Ventilation (MVV)
- Maximal volume breathed in 1 minute by voluntary effort
- Normal ≈ FEV₁ × 40 L/min
- Decreased in: airway obstruction, neuromuscular disease, deconditioning, morbid obesity
- Correlates with subjective dyspnoea and exercise tolerance
- Useful in pre-operative evaluation (lung resection)
Diffusing Capacity (DLCO) — Adjunct to Spirometry
Although not a spirometric parameter, it complements spirometry:
- Normal/elevated in asthma (↑ perfusion upper zones, large lung volumes)
- Reduced in emphysema (destroyed alveoli)
- Reduced in pulmonary fibrosis
- Unexpectedly elevated DLCO → suspect undiagnosed asthma
Summary Table
| Parameter | Obstructive | Restrictive | Mixed |
|---|---|---|---|
| FEV₁ | ↓↓ | ↓ | ↓↓ |
| FVC | Normal or ↓ | ↓↓ | ↓↓ |
| FEV₁/FVC | ↓ (<0.70) | Normal/↑ | ↓ |
| TLC | ↑ (hyperinflation) | ↓ | Variable |
| RV | ↑↑ | ↓ | ↑ |
| DLCO | ↓ (emphysema) / N (asthma) | ↓ | ↓ |
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Harrison's Principles of Internal Medicine, 21e; Bailey & Love's Short Practice of Surgery, 28e; GOLD 2025 Report
Physiology behind it
Finding Sources
Finding Sources
Searching Images
equal pressure point expiratory flow limitation physiology diagram
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Give me crisp point wise answer to fetch more marks
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Give me crisp concise point for exam purpose with some physiology
Finding Sources
Searching Images
equal pressure point forced expiration physiology airway collapse spirometry
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
pressure volume curve lung compliance elastic recoil spirometry physiology
Loading Image
Loading Image
Finding Sources
I now have all the physiology content needed. Here is the crisp, exam-focused answer:
PHYSIOLOGY BEHIND SPIROMETRY — Exam Answer
1. WHAT SPIROMETRY ACTUALLY MEASURES
- Spirometry measures airflow generated by the mechanical interaction between:
- Respiratory muscles (force generators)
- Lung elastic recoil (stored energy)
- Airway resistance (opposition to flow)
- The instrument converts flow → integrates → volume over time
2. FORCES DRIVING EXPIRATION
Two components of alveolar pressure (Palv):
Palv = Pleural pressure (Ppl) + Lung elastic recoil pressure
- At rest (no flow): Ppl is negative (~−5 cmH₂O), elastic recoil positive; net Palv = 0
- On forced expiration: expiratory muscles contract → Ppl becomes positive → Palv rises → air is driven out
- The driving pressure for expiratory flow = elastic recoil of the lung (not Ppl alone)
3. THE KEY CONCEPT: EQUAL PRESSURE POINT (EPP) — ★ High-yield ★
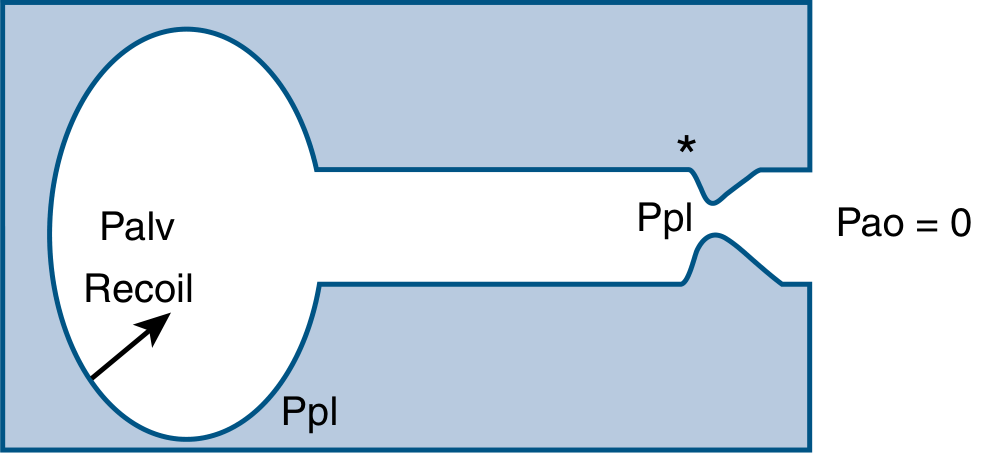
- As air flows from alveoli → mouth, airway pressure drops progressively due to frictional resistance
- At some point along the airway: intraluminal pressure = surrounding pleural pressure → this is the Equal Pressure Point (EPP)
- Downstream (mouthward) of EPP: Ppl exceeds intraluminal pressure → dynamic airway compression
- Result: Further increase in expiratory effort does NOT increase flow → flow becomes effort-independent
Key equation:
V̇max = Elastic recoil pressure (PL) ÷ Upstream resistance (Rus)
- Flow is determined only by lung recoil and upstream resistance, NOT by effort
- EPP moves upstream (toward alveoli) as effort increases → eventually fixed in lobar/segmental bronchi
4. EFFORT-DEPENDENT vs. EFFORT-INDEPENDENT PORTIONS
| Portion of FVC curve | Physiological basis |
|---|---|
| First 25–30% (peak flow region) | Effort-dependent — flow ↑ with greater muscle force; large airways open wide |
| Remaining 70–75% (descending limb) | Effort-independent — determined by EPP mechanics; reflects lung recoil + small airway resistance |
Clinical implication: FEV₁ incorporates both portions → reproducible and clinically meaningful. FEF₂₅₋₇₅% is from the effort-independent zone → sensitive for small airway disease.
5. PRESSURE–VOLUME (P-V) CURVE — Basis of Lung Mechanics
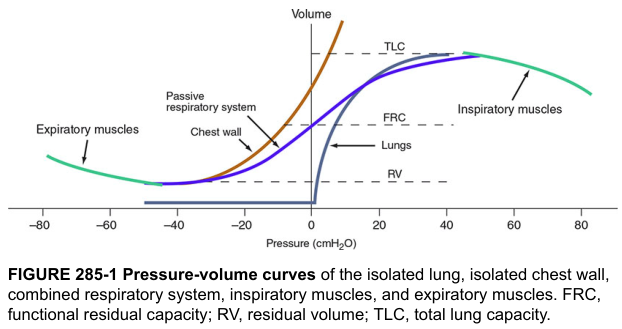
- Lungs alone: tend to collapse inward at all volumes (elastic recoil inward)
- Chest wall alone: tends to spring outward below ~70% TLC
- FRC = equilibrium point where lung recoil inward = chest wall recoil outward (no muscle activity needed)
- TLC = point where inspiratory muscle force is fully opposed by combined recoil of lungs + chest wall
- RV = point where either chest wall rigidity OR airway closure prevents further exhalation
6. WHY FEV₁/FVC IS THE KEY RATIO
| Physics | Clinical meaning |
|---|---|
| At high lung volumes → high elastic recoil → airways dilated → low resistance → fast flow | FEV₁ is high in normal lungs |
| As volume decreases during expiration → recoil falls → airways narrow → resistance ↑ → flow decelerates | Curve descends on flow-volume loop |
| In obstruction: airways narrow excessively (↑ resistance, ↓ recoil in emphysema) → EPP shifts upstream → more dynamic compression | FEV₁ disproportionately ↓ → FEV₁/FVC < 0.70 |
| In restriction: lung volume is small but airways and recoil are often normal → both FEV₁ and FVC ↓ proportionally | FEV₁/FVC normal or ↑ |
7. PHYSIOLOGY OF INDIVIDUAL PARAMETERS
FVC
- Determined by: TLC − RV
- Limited by: chest wall rigidity, airway closure, muscle weakness, lung stiffness
FEV₁
- Determined by: airway calibre + elastic recoil + effort (early phase)
- Most reproducible measure — standard deviation only ~200 mL in normal subjects
FEF₂₅₋₇₅%
- Reflects small airway (<2 mm) resistance
- Small airways contribute <20% of total airway resistance → disease here is "silent" until FEF₂₅₋₇₅% falls
PEFR (Peak Expiratory Flow Rate)
- Occurs within first 100–120 ms of forced expiration
- Entirely effort-dependent → useful for monitoring (asthma diary) but not diagnosis
MVV (Maximal Voluntary Ventilation)
- MVV ≈ FEV₁ × 40
- Reflects respiratory muscle endurance + coordination, not just airways
8. PHYSIOLOGY OF OBSTRUCTIVE vs. RESTRICTIVE DEFECTS
Obstructive (e.g., asthma, COPD, emphysema)
- ↑ Airway resistance → EPP shifts far upstream → severe dynamic compression
- In emphysema: ↓ elastic recoil → Vmax = PL/Rus → both PL↓ and Rus↑ → severe flow limitation
- Air trapping: small airways close prematurely → RV↑, FRC↑, TLC↑
- Hyperinflation: diaphragm flattens → mechanical disadvantage → ↑ work of breathing
Restrictive (e.g., fibrosis, pleural disease, kyphoscoliosis)
- ↓ Lung compliance (stiff lungs) → reduced TLC, VC, FRC
- Elastic recoil is increased in fibrosis → flow rates preserved or even ↑
- FEV₁/FVC normal or elevated (stiff lung recoils quickly → empties fast proportionally)
- Work of breathing ↑ due to stiff lung (high elastic work)
9. PHYSIOLOGY OF BRONCHODILATOR RESPONSE
- Bronchodilators (β₂ agonists) → ↑ intracellular cAMP → smooth muscle relaxation → ↑ airway calibre
- ↑ calibre → ↓ resistance → EPP moves downstream → ↓ dynamic compression → ↑ FEV₁ and FVC
- Positive response: FEV₁ ↑ ≥12% AND ≥200 mL → reversible obstruction (asthma > COPD)
10. WHY RV CANNOT BE MEASURED BY SPIROMETRY — Physiology
- After maximal exhalation, air remains in lungs (RV) due to:
- Airway closure — small airways collapse at low lung volumes (closure volume > RV in elderly/smokers)
- Chest wall rigidity — in young individuals, chest wall springs back and limits further exhalation
- Since spirometry measures air moving in or out, trapped RV cannot be detected
- Measured by: Helium dilution, Nitrogen washout, or Body plethysmography (most accurate)
QUICK PHYSIOLOGY SUMMARY TABLE
| Parameter | Main determinant | Physiological insight |
|---|---|---|
| FVC | TLC − RV | Limited by airway closure + chest wall |
| FEV₁ | Airway resistance + recoil | EPP location determines flow |
| FEV₁/FVC | Balance of recoil vs resistance | < 0.70 → obstruction |
| PEFR | Effort + large airway calibre | Effort-dependent, monitoring only |
| FEF₂₅₋₇₅% | Small airway resistance | First sign of peripheral airway disease |
| RV | Airway closure point | Cannot be measured by spirometry |
| FRC | Lung recoil = chest wall recoil | Equilibrium of opposing forces |
| TLC | Max inspiratory muscle force | Overcome by combined lung + chest wall recoil |
Sources: Fishman's Pulmonary Diseases & Disorders; Murray & Nadel's Textbook of Respiratory Medicine; Harrison's Principles of Internal Medicine, 21e
This is a shared conversation. Sign in to Orris to start your own chat.