Explain trratment and doms of erector spinae and quadram limboram
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple textbooks. Let me compile the full answer.
Erector Spinae and Quadratus Lumborum - Anatomy, DOMS, and Treatment
ERECTOR SPINAE
Anatomy
The erector spinae is the largest group of intrinsic back muscles. The muscles lie posterolaterally to the vertebral column, between the spinous processes medially and the angles of the ribs laterally. They are covered in the thoracic and lumbar regions by the thoracolumbar fascia.
The mass arises from a broad, thick common tendon attached to:
- The sacrum
- Spinous processes of the lumbar and lower thoracic vertebrae
- Iliac crest
In the upper lumbar region it splits into three vertical columns, each further subdivided regionally:
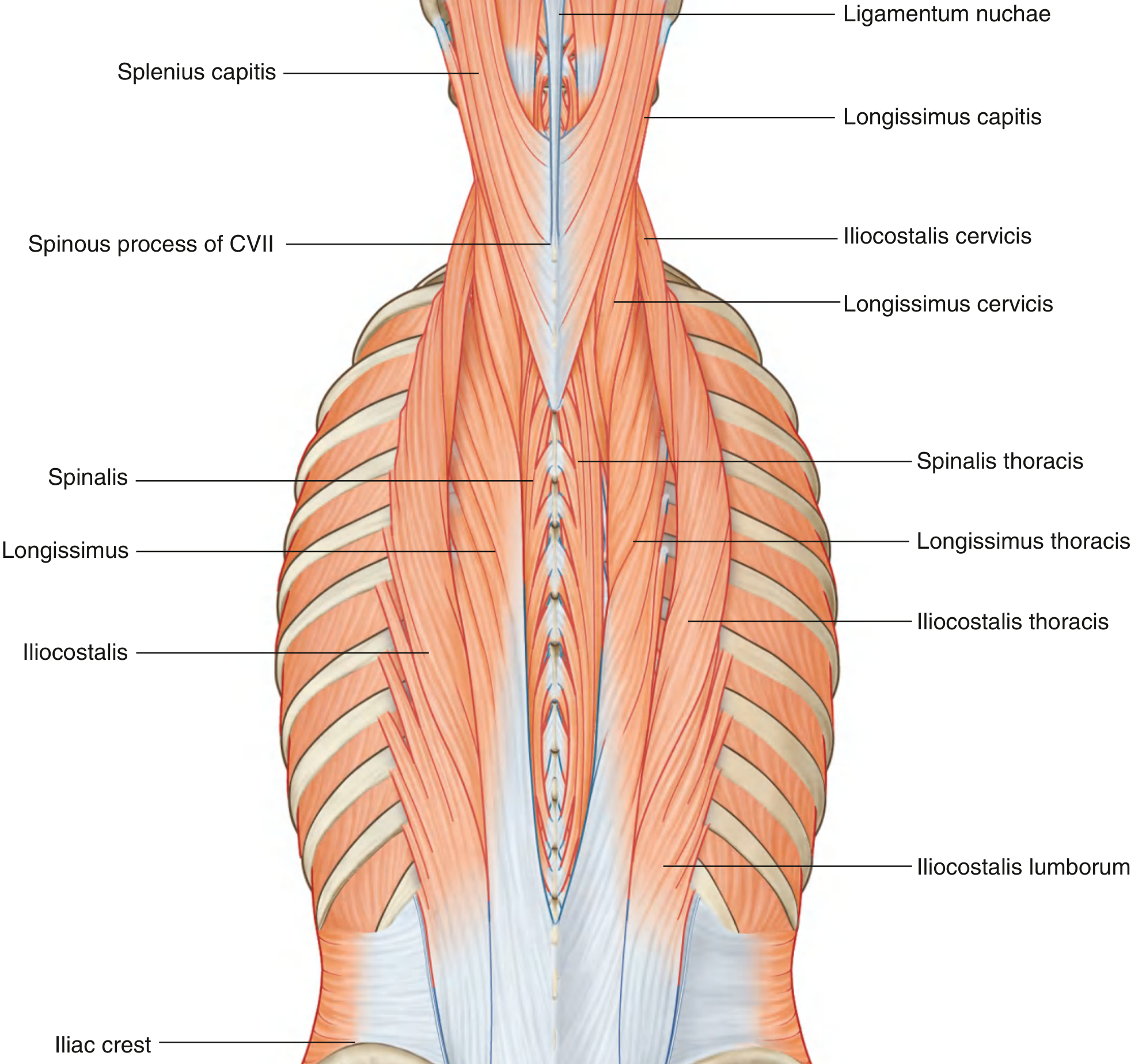
Fig. 2.50 Deep Group of Back Muscles - Erector Spinae Muscles (Gray's Anatomy for Students)
| Column | Muscle | Origin | Insertion |
|---|---|---|---|
| Iliocostalis | Iliocostalis lumborum | Sacrum, lumbar/lower 2 thoracic spinous processes, iliac crest | Angles of lower 6-7 ribs |
| Iliocostalis thoracis | Angles of lower 6 ribs | Angles of upper 6 ribs + TP of CVII | |
| Iliocostalis cervicis | Angles of ribs III-VI | Transverse processes (TP) of CIV-CVI | |
| Longissimus | Longissimus thoracis | Blends with iliocostalis; TPs of lumbar vertebrae | TPs of all thoracic vertebrae + lower 9-10 rib tubercles |
| Longissimus cervicis | TPs of upper 4-5 thoracic vertebrae | TPs of CIII-CVI | |
| Longissimus capitis | TPs upper T/lower C vertebrae | Posterior margin of mastoid process | |
| Spinalis | Spinalis thoracis | Spinous processes TX/TXI to LIII | Spinous processes TII-TVIII |
| Spinalis cervicis | Ligamentum nuchae, CVII spinous process | Spinous process of CIII (axis) |
Innervation: Posterior (dorsal) rami of spinal nerves at each level (segmental innervation throughout the entire column).
Function: Extension and lateral flexion of the vertebral column; maintenance of upright posture. The three columns together "erect the spine."
DOMS of Erector Spinae
Delayed-onset muscle soreness (DOMS) in the erector spinae typically presents as:
- Deep, aching stiffness along the thoracic and/or lumbar spine, typically beginning 12-24 hours after unaccustomed activity and peaking at 24-72 hours
- Common triggers: deadlifts, heavy squats, rowing, prolonged forward bending, carrying loads
- Reduced range of motion in spinal extension and lateral flexion
- Tenderness to palpation of the longitudinal muscle columns alongside the spine
- Pain is bilateral when the cause is axial loading; unilateral in asymmetric tasks
Trigger points in the erector spinae group (thoracic paraspinals) are frequently associated with both migraine and tension headaches, in addition to local and referred back pain.
Treatment of Erector Spinae DOMS / Myofascial Pain
Noninvasive (first-line):
- Rest and activity modification
- NSAIDs (e.g. ibuprofen, naproxen) - reduce prostaglandin-mediated pain
- Muscle relaxants (e.g. cyclobenzaprine)
- Spray and stretch - vapocoolant spray followed by passive stretching of the muscle
- Massage therapy
- Ischemic compression of trigger points
- Heat application (improves blood flow and reduces stiffness)
Invasive (for trigger points that fail noninvasive treatment):
The "universal technique" for trigger point injection (Roberts & Hedges' Clinical Procedures in Emergency Medicine):
- Position the patient recumbent (relaxes muscle, prevents syncope)
- Identify and mark the trigger point; clean skin with antiseptic
- Use a 22-gauge, 1.5-inch needle for superficial muscles; 21-gauge, 2-2.5-inch for deeper
- Grasp skin between thumb and index finger; insert needle 1-1.5 cm from the trigger point at a 30-degree angle
- Aspirate first (to exclude blood vessel entry), then inject a small amount
- Withdraw to skin, redirect, and reinject using a fast-in, fast-out technique to elicit a local twitch response - this is critical for effectiveness
- Paresthesia or severe cramping = withdraw immediately (nerve contact)
- After injection, put the muscle through a full active stretch
Injectate options:
- Local anesthetic (lidocaine 1%) is preferred - reduces post-injection soreness
- Sterile saline or dry needling are equally effective (nature of injectate does not change outcome)
- Steroids are NOT recommended for trigger points - no inflammatory basis for trigger point pain
- Botulinum toxin has been used
ESP (Erector Spinae Plane) Block - for regional anesthesia/analgesia:
The ESP block deposits local anesthetic deep to the erector spinae muscles, between the muscle and the transverse process. It was first described in 2016 for thoracic neuropathic pain and has become popular as an alternative to paravertebral blocks.
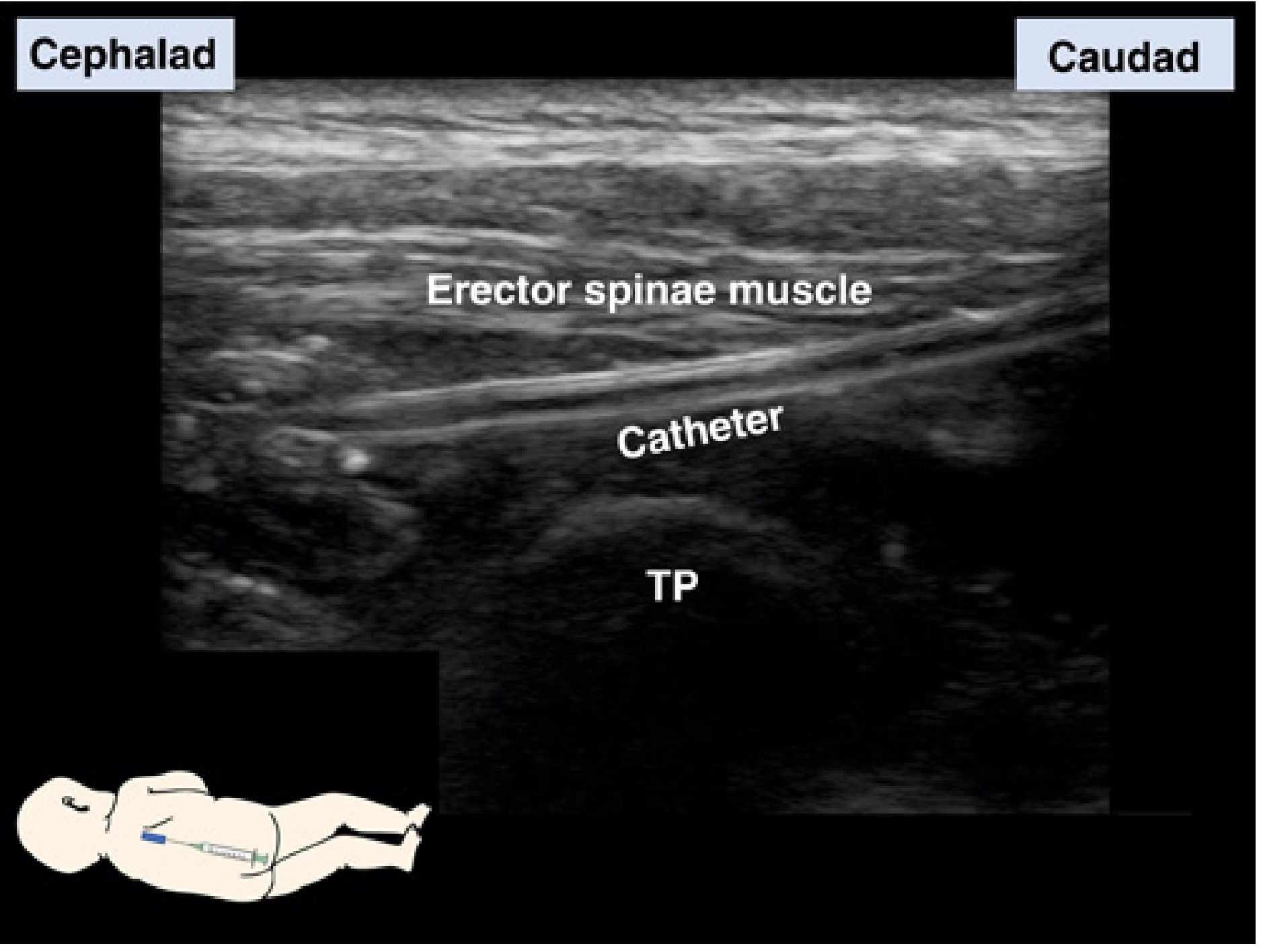
FIG. 74.30 Erector spinae plane (ESP) block - catheter in the interfascial plane deep to the erector spinae (Miller's Anesthesia)
ESP Block technique:
- Patient seated or lateral decubitus
- Linear/curvilinear ultrasound probe in parasagittal orientation
- Identify trapezius, rhomboid, and erector spinae muscles superficial to transverse processes
- Insert long block needle caudad-to-cephalad or cephalad-to-caudad, in-plane, until it contacts the transverse process
- Inject a large volume (30-50 mL) of local anesthetic - spread should be seen over several spinal levels
- Local anesthetic diffuses into the paravertebral space covering multiple dermatomes
Advantages: avoids risks of dural puncture, pneumothorax (though pneumothorax has been reported), bladder catheterization, and spinal hematoma. Can be used with anticoagulation.
- Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 1952
- Miller's Anesthesia, 10e
QUADRATUS LUMBORUM (QL)
Anatomy
The QL muscles fill the space between rib XII and the iliac crest on both sides of the vertebral column. They are overlapped medially by psoas major and bordered laterally by transversus abdominis.
| Detail | |
|---|---|
| Origin | Transverse process of LV vertebra, iliolumbar ligament, and iliac crest |
| Insertion | Transverse processes of LI-LIV vertebrae + inferior border of rib XII |
| Innervation | Anterior rami of T12 and L1-L4 spinal nerves |
| Functions | Depress and stabilize rib XII; lateral flexion of trunk; bilateral action extends lumbar spine; respiratory accessory - anchors rib XII for diaphragmatic pull |
The QL is considered a "hip hiker" (elevates the ipsilateral ilium) and a lateral flexor of the spine.
- Gray's Anatomy for Students, p. 431
DOMS of Quadratus Lumborum
-
Presents as unilateral or bilateral low back pain and stiffness, often extending to the iliac crest, lower abdomen, or groin
-
Triggered by: heavy lifting in lateral flexion, carrying loads on one side, prolonged sitting with lumbar asymmetry, or sudden trunk side-bending
-
Trigger points are extremely common in the QL and are found along the 12th rib, around the iliac crest, and along the lateral border of the muscle
-
Referred pain can go to the anterior abdominal wall; QL trigger points can also accentuate postoperative pain or painful lower-quadrant abdominal scars
-
Trigger points may be associated with distress on deep inspiration and 12th rib pain (because the QL stabilizes rib XII during breathing)
-
The QL and gluteus medius should be suspected in all patients presenting with low back pain
-
Roberts & Hedges' Clinical Procedures in Emergency Medicine
Treatment of Quadratus Lumborum DOMS / Myofascial Pain
Noninvasive (same as erector spinae - see above): NSAIDs, muscle relaxants, spray-and-stretch, massage, ischemic compression, and heat
Trigger point injection: Same universal technique as above. QL trigger points that fail conservative management should be injected. Because the QL is a deep muscle, a 21-gauge, 2-2.5-inch needle is required.
Quadratus Lumborum (QL) Block - regional anesthesia/analgesia for abdominal and lower-body surgery:
The QL block targets the thoracolumbar fascia (TLF) around the QL muscle. Local anesthetic in the TLF (which contains mechanoreceptors, nociceptors, and sympathetic fibers) diffuses into the paravertebral space producing visceral analgesia. Dermatomal spread: T8 to L1, routinely affecting the iliohypogastric and ilioinguinal nerves.
Guidance: Ultrasound only (no nerve to stimulate). A 50-100mm, 22-gauge short-bevel needle. Recommended dose: 0.5 mL/kg of 0.2% ropivacaine per side (max 3 mg/kg, max 20 mL).
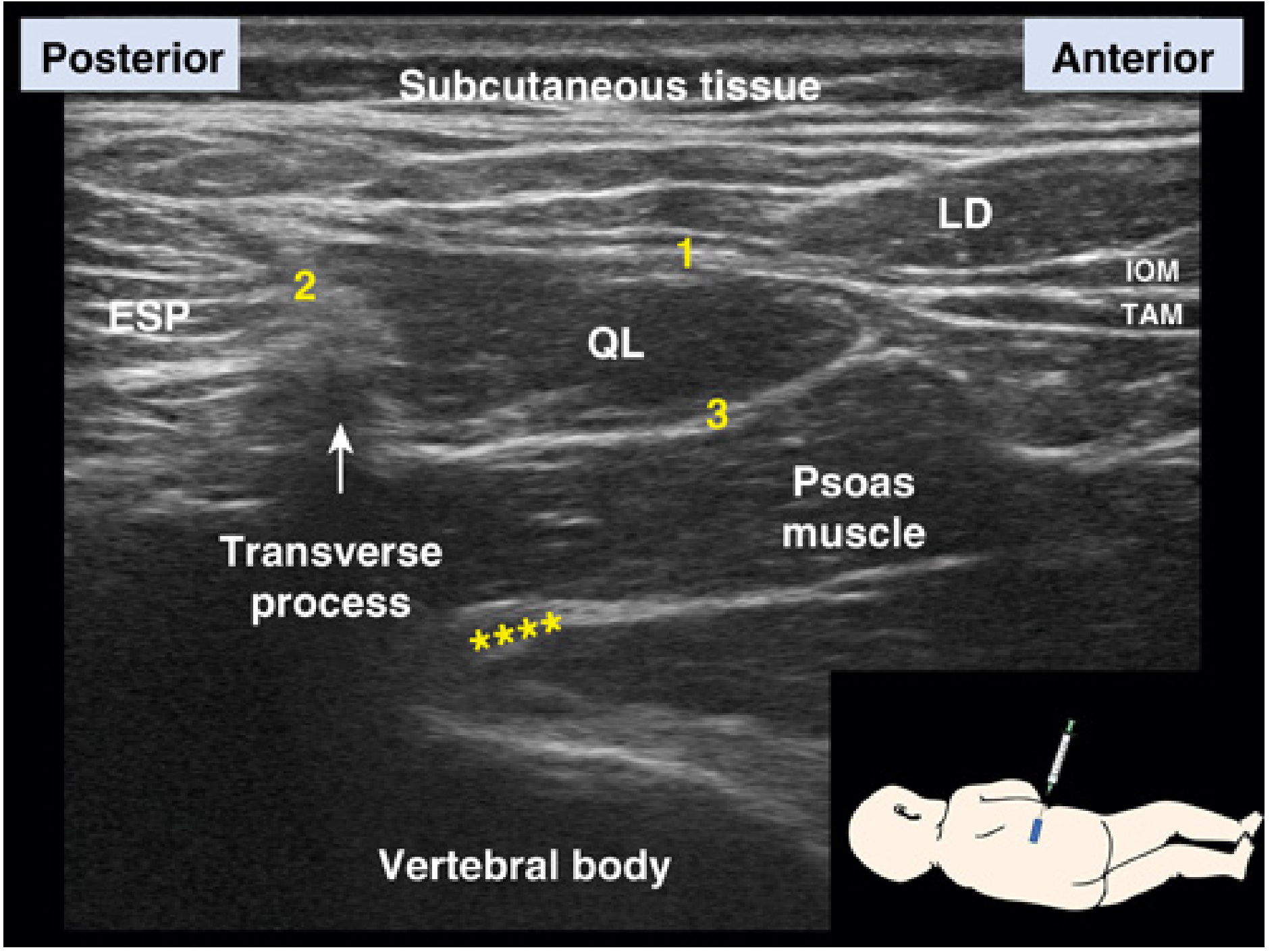
FIG. 74.37 Quadratus lumborum (QL) blocks - 1 = lateral (QL1), 2 = posterior (QL2), 3 = anterior/transmuscular (QL3). ESP = erector spinae, LD = latissimus dorsi (Miller's Anesthesia)
There are three QL block approaches:
| Approach | Also Called | Target | Volume | Patient Position |
|---|---|---|---|---|
| QL1 (Lateral) | Type 1 | Lateral aspect of QL, deep to TA posterior aponeurosis | 20-30 mL | Supine or lateral |
| QL2 (Posterior) | Type 2 | Posterior QL, between QL and erector spinae muscles (central thoracolumbar fascial plane) | 20-30 mL | Lateral decubitus |
| QL3 (Transmuscular/Anterior) | QL3, Anterior QL | Anterior QL, at the QL-psoas border | 20-30 mL | Lateral or prone |
For the QL3 block, the needle traverses the erector spinae muscle belly and then the QL muscle belly to reach the QL-psoas interface. The QL "shamrock sign" (QL and psoas as "leaves" and the transverse process as "stem") aids ultrasound identification.
- Miller's Anesthesia, 10e, p. 11096-11098
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1962
Summary Table
| Feature | Erector Spinae | Quadratus Lumborum |
|---|---|---|
| Location | Posterolateral to vertebral column | Between rib XII and iliac crest (posterior abdominal wall) |
| Innervation | Dorsal rami (all levels) | Anterior rami T12, L1-L4 |
| Key actions | Extend & laterally flex spine | Lateral flexion, rib XII stabilization, "hip hiking" |
| DOMS triggers | Deadlifts, squats, rowing | Lateral lifting, asymmetric postures |
| Referred pain | Local back/thoracic; paraspinal headaches | Low back, iliac crest, anterior abdomen, groin, 12th rib |
| Regional block | ESP block (large volume, T/P plane) | QL1/QL2/QL3 blocks (TLF targeting) |
This is a shared conversation. Sign in to Orris to start your own chat.