Appendix
Reading File
Finding Sources
Searching the Web
appendix anatomy physiology appendicitis overview
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the appendix (vermiform appendix) drawn from authoritative medical textbooks:
Vermiform Appendix
Anatomy
The vermiform appendix is a narrow, blind-ended tube that projects from the posteromedial wall of the cecum, just below the ileocecal valve. It develops embryologically as part of the midgut, forming as a bud from the midgut loop between the 8th and 12th weeks of gestation.
Key measurements:
- Average length: 9-10 cm (range: 5-35 cm)
- Average diameter: ~6 mm
Position: The appendix assumes a highly variable position. Unlike the rest of the colon - where the longitudinal muscle forms teniae coli - the appendix has a continuous circumferential longitudinal muscle layer and no teniae. Surgically, this is useful: following the teniae of the cecum leads directly to the appendiceal base.
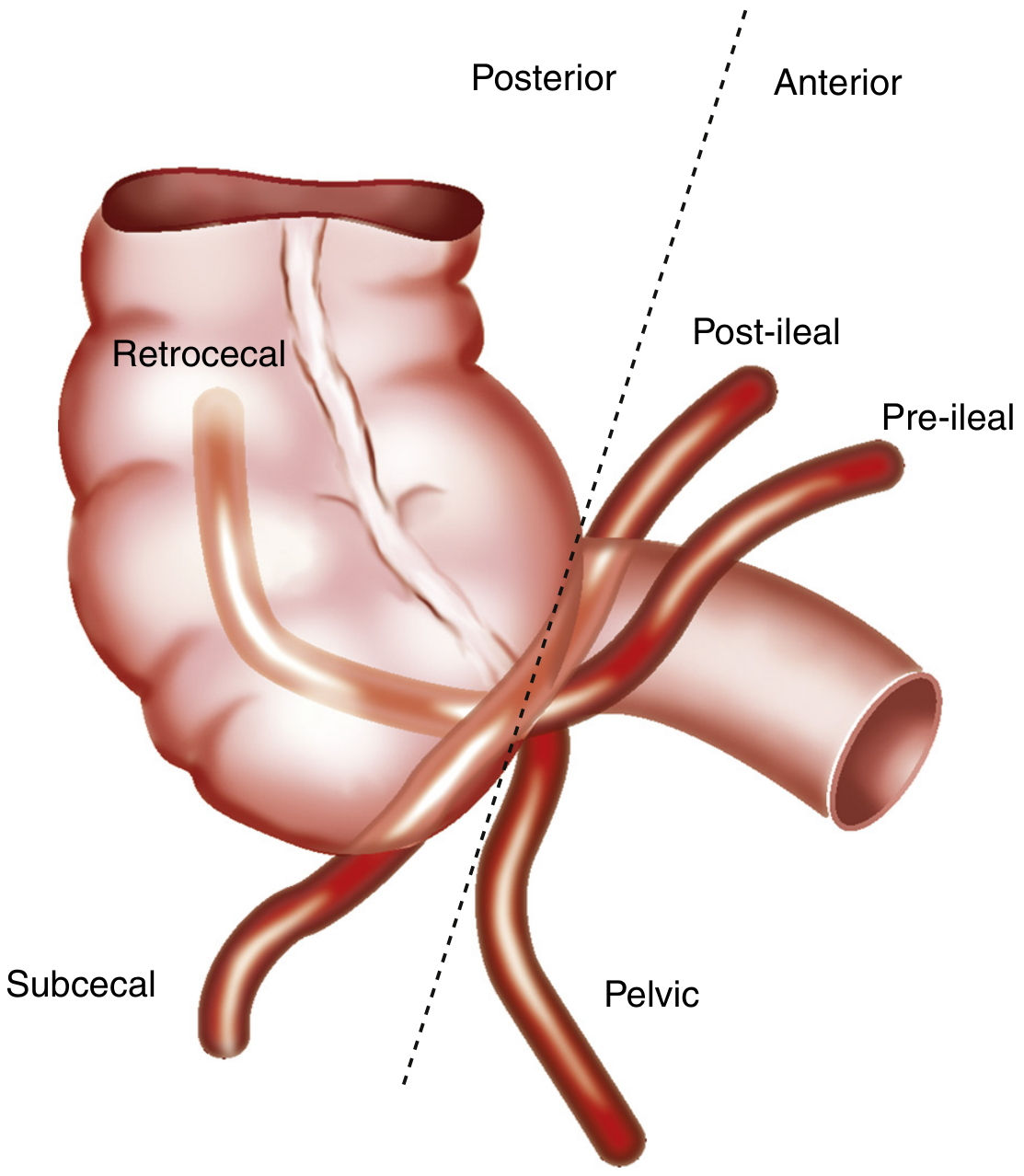
Five positions of the appendix. Retrocecal is most common (~65%), followed by pelvic/subcecal (~31%). - Sleisenger and Fordtran's GI and Liver Disease, Fig. 120.1
| Position | Frequency |
|---|---|
| Retrocecal (ascending) | ~65% |
| Subcecal / pelvic (descending) | ~31% |
| Transverse retrocecal | ~2% |
| Pre-ileal (paracecal) | ~1% |
| Post-ileal (retroileal) | ~0.5% |
McBurney's point: The classic surface landmark is located at the junction of the lateral and middle thirds of a line from the right anterior superior iliac spine to the umbilicus. However, the appendix is within 5 cm of this point in less than 50% of cases, explaining why tenderness at McBurney's point is not universal in appendicitis.
Blood Supply, Venous Drainage & Lymphatics
- Arterial supply: The appendicular artery - a branch of the ileocolic artery (the last branch of the superior mesenteric artery) - runs within the mesoappendix to supply the appendix.
- Venous drainage: Via the appendicular vein → ileocolic vein → superior mesenteric vein → portal vein.
- Lymphatics: Drain to the ileocolic lymph nodes, shared with the terminal ileum and ascending colon.
- Peritoneum: The appendix is an intraperitoneal structure with its own mesentery (mesoappendix).
Histology
Microscopically, the appendix resembles the large intestine but with several distinguishing features:
- Crypts (intestinal glands) are present but shallow and irregular (unlike the deep, packed crypts of the cecum).
- The most distinctive feature is a massive collection of lymphoid follicles (aggregated lymphoid nodules) extending from the lamina propria through the muscularis mucosae into the submucosa.
- This dense lymphoid tissue makes the appendix an important component of the gut-associated immune system - sometimes described as a "safe house" for symbiotic gut microbiota.
Function
Once considered a vestigial organ, current understanding recognizes two roles:
- Immune function: The appendix is rich in lymphoid tissue (GALT - gut-associated lymphoid tissue) and likely plays a role in mucosal immunity, particularly in early life.
- Microbiome reservoir: It has been proposed to serve as a reservoir for beneficial gut bacteria, potentially aiding recolonization after gastrointestinal illness.
Acute Appendicitis
Appendicitis is the most common abdominal surgical emergency. Inflammation is classified as:
| Stage | Gross / Microscopic Features |
|---|---|
| Acute (suppurative) | Serosal injection and edema; neutrophilic infiltrate involving the muscularis propria circumferentially; mucosal ulceration and microabscesses |
| Gangrenous | Transmural inflammation; focal mural necrosis; greenish/black discoloration; prominent vascular thrombosis |
| Perforated | Breakdown of the necrotic wall; spillage of contents; adjacent abscess formation or generalized peritonitis |
Note: Mucosal inflammation alone ("catarrhal" inflammation) is not sufficient for microscopic diagnosis of appendicitis - inflammation must extend to the muscularis propria.
Pathogenesis (two main hypotheses):
-
Obstruction hypothesis: A fecalith or lymphoid hyperplasia obstructs the lumen → raised intraluminal pressure → venous hypertension → ischemia → bacterial invasion and necrosis. However, fecaliths are found in only 3.6-27% of cases, and elevated intraluminal pressure is present in only a minority.
-
Mucosal ulceration hypothesis: Bacterial or viral enteric infection (CMV has been implicated) causes primary mucosal ulceration → bacterial invasion by normal colonic flora. Mucosal ulceration is found in up to 75% of appendicitis cases and is a more consistent finding than fecaliths.
Appendiceal Tumors
- Neuroendocrine tumors (NETs) are the most common appendiceal neoplasm (60-80% of appendiceal tumors), and are found incidentally in ~1-1.5% of appendectomy specimens.
- Lymph node metastasis rates correlate with tumor size: 15% for <1 cm, 47% for 1-2 cm, 86% for >2 cm.
- Management is guided by size: small NETs (<1 cm) can be treated with simple appendectomy; larger or high-risk tumors require right hemicolectomy with lymphadenectomy.
Sources:
- Color Atlas of Human Anatomy Vol. 2, Internal Organs, pp. 338-342
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, pp. 2436-2438
- Sabiston Textbook of Surgery, p. 1613
This is a shared conversation. Sign in to Orris to start your own chat.