Approach to altered sensorium from harrison 22nd edition
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer. Let me compile the full response from Harrison's 22E.
Approach to Altered Sensorium - Harrison's Principles of Internal Medicine, 22nd Edition (2025)
Chapters 29 (Confusion and Delirium) and 30 (Coma) — S. Andrew Josephson, Bruce L. Miller
Terminology and Definitions
Harrison's 22E uses several interchangeable terms for altered sensorium: encephalopathy, acute brain failure, acute altered mental status, acute confusional state, and "ICU psychosis." The unifying term is delirium - a relatively acute decline in cognition that fluctuates over hours or days.
The spectrum of altered sensorium ranges from:
- Confusion - reduced comprehension, coherence, and capacity to reason
- Delirium - acute confusional state (hallmark = attention deficit)
- Stupor - patient arousable only with vigorous stimulation
- Coma - unresponsive, unarousable state
PART I: DELIRIUM (Acute Confusional State)
Clinical Features
The hallmark is a deficit of attention, though all cognitive domains are variably affected - memory, executive function, visuospatial tasks, and language. Associated features include:
- Altered sleep-wake cycles
- Perceptual disturbances (hallucinations, delusions)
- Affect changes
- Autonomic instability (HR and BP fluctuations)
Two subtypes:
| Feature | Hyperactive | Hypoactive |
|---|---|---|
| Prototype | Alcohol withdrawal (DTs) | Benzodiazepine intoxication |
| Presentation | Agitation, tremor, hallucinations, hyperarousal | Apathy, withdrawal, psychomotor slowing |
| Recognition | Easily recognized | Often missed; underdiagnosed |
Patients often fluctuate between subtypes along a spectrum. Hypoactive delirium is frequently overlooked on medical wards and in the ICU.
Risk Factors (Table 29-1 in Harrison's)
Predisposing (baseline vulnerability):
- Age >65 years
- Pre-existing cognitive impairment/dementia
- Severe illness, functional dependence
- Sensory deprivation (vision/hearing loss)
- Dehydration, malnutrition
Precipitating factors:
| Category | Examples |
|---|---|
| Toxins | Anticholinergics, opioids, benzodiazepines; alcohol (intoxication/withdrawal); opiates; cocaine; PCP, ketamine; carbon monoxide, pesticides |
| Metabolic | Electrolyte disturbances (hypo/hyperglycemia, hypo/hypernatremia, hypercalcemia); hypothermia/hyperthermia; pulmonary failure (hypoxemia, hypercarbia); hepatic failure; renal failure/uremia; cardiac failure; B1/B12/folate/niacin deficiency; anemia |
| Infections | UTI, pneumonia, sepsis; CNS - meningitis, encephalitis, brain abscess |
| Endocrine | Hypothyroidism/hyperthyroidism; hyperparathyroidism; adrenal insufficiency |
| Cerebrovascular | Global hypoperfusion (heart failure, septic shock, dehydration, anemia); hypertensive encephalopathy; focal strokes (right parietal, medial dorsal thalamic) |
| Autoimmune | CNS vasculitis; cerebral lupus; autoimmune/paraneoplastic encephalitis |
| Seizure-related | Nonconvulsive status epilepticus (NCSE); postictal states |
| Neoplastic | Diffuse brain metastases; carcinomatous meningitis; CNS lymphoma |
| Hospitalization | Terminal end-of-life delirium |
Laboratory and Diagnostic Evaluation (Table 29-2)
Initial evaluation (all patients):
- History - special attention to medications (including OTC and herbals)
- General physical + neurologic examination
- CBC, electrolyte panel (Ca, Mg, Phosphorus), LFTs (with albumin), renal function tests
First-tier further evaluation:
- Systemic infection screen: UA + culture, chest X-ray + respiratory pathogen tests, blood cultures
- ECG
- ABG
- Serum/urine toxicology screen (earlier in young patients)
- Serum B12, folate, thiamine levels
Second-tier (if above unrevealing):
- Brain CT or MRI
- EEG (essential when NCSE is suspected or etiology remains unclear)
- LP - CSF analysis (meningitis, encephalitis)
- Autoimmune/paraneoplastic antibody panel
- Thyroid function, cortisol, ammonia
Per Harrison's: "No single algorithm will fit all delirious patients due to the staggering number of potential etiologies." If a clear precipitant (e.g., offending medication) is identified, further testing may not be required.
Management of Delirium
Principle: Treat the underlying cause first. Pharmacologically targeting symptoms alone prolongs confusion and masks diagnostic information.
Non-pharmacologic (supportive) care - most effective first-line approach:
- Reorientation by nursing staff and family
- Visible clocks, calendars, outside-facing windows
- Sensory aids: glasses, hearing aids
- Sundowning prevention: daytime activities, quiet dark nights, limit nocturnal interruptions
- Melatonin before bed to promote sleep
- Mimic home environment: familiar objects, bedding, clothing
- Family visits throughout the day
- Maintain nutrition, hydration, manage pain, incontinence, skin breakdown
- Minimize "tethers" (Foley catheters, nasal cannulas, telemetry) that restrict movement
Pharmacologic therapy:
- Reserve for severe agitation endangering the patient or staff
- Low-dose haloperidol remains standard; atypical antipsychotics (quetiapine, olanzapine) are alternatives
- Avoid benzodiazepines except in alcohol/sedative withdrawal delirium - they worsen most other causes
- Dexmedetomidine in the ICU setting
PART II: COMA
Anatomy and Physiology
Almost all coma traces to either:
- Widespread abnormalities of both cerebral hemispheres, or
- Reduced activity of the reticular activating system (RAS) - neurons in the upper brainstem and thalamus
The RAS, its ascending projections to the cortex, and the cortex itself are all required to maintain alertness and coherent thought. Suppression occurs from drugs, toxins, or metabolic derangements (hypoglycemia, anoxia, uremia, hepatic failure) - metabolic causes are far more common than structural injuries.
Herniation Syndromes
The skull prevents outward expansion; dural infoldings create compartments. Herniation = displacement of brain tissue into a compartment it normally does not occupy.
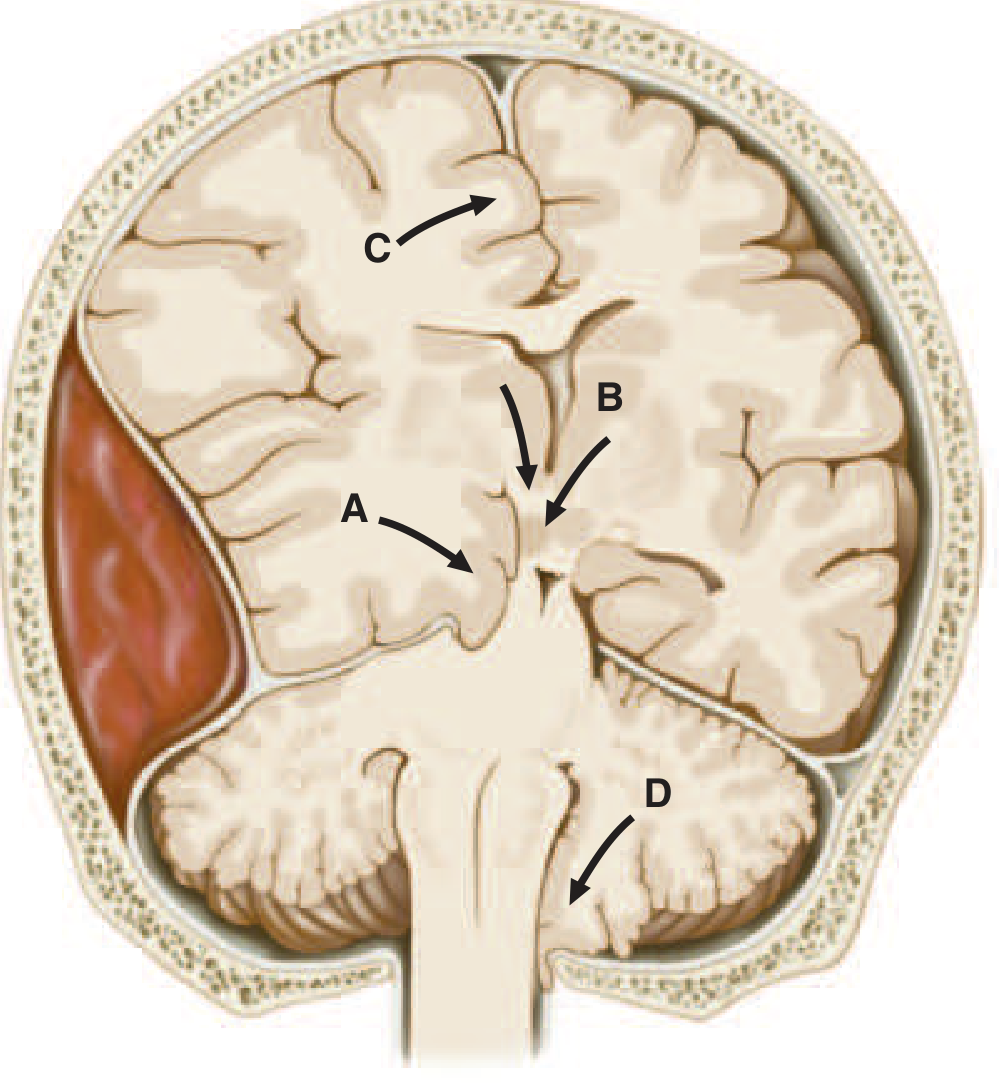
Uncal transtentorial herniation: Anterior medial temporal gyrus (uncus) herniates into tentorial opening. First sign = ipsilateral pupil dilation (CN III compression - parasympathetic fibers are peripheral in the nerve). As herniation progresses: ipsilateral hemiplegia → bilateral motor signs → decerebrate posturing.
Central transtentorial herniation: Rostral-caudal deterioration - drowsiness → stupor → coma; pupils go from small/reactive → fixed/dilated as midbrain is compressed.
Differential Diagnosis of Coma (Table 30-1)
Three broad categories:
1. No focal neurologic signs (CT often normal):
- Intoxications: alcohol, sedatives, opiates
- Metabolic: anoxia, hyponatremia, hypernatremia, hypercalcemia, DKA, NKHH, hypoglycemia, uremia, hepatic coma, hypercarbia, Addisonian crisis, thyroid states, nutritional deficiency
- Severe systemic infections: pneumonia, septicemia, typhoid fever, malaria, Waterhouse-Friderichsen syndrome
- Shock from any cause
- Status epilepticus / NCSE / postictal states
- Hyperperfusion syndromes: hypertensive encephalopathy, eclampsia, PRES
- Severe hyper/hypothermia
- Concussion
- Acute hydrocephalus
2. Focal brainstem or lateralizing cerebral signs (CT typically abnormal):
- Hemispheral hemorrhage (basal ganglionic, thalamic) or large MCA infarction with secondary brainstem compression
- Brainstem infarction (basilar artery thrombosis/embolism)
- Brain abscess, subdural empyema
- Epidural/subdural hemorrhage, brain contusion
- Brain tumor with surrounding edema
- Cerebellar and pontine hemorrhage/infarction
- Widespread traumatic brain injury
- Metabolic coma in the setting of preexisting focal damage
3. Meningismus syndromes (fever/stiff neck + CSF pleocytosis):
- Bacterial meningitis
- Subarachnoid hemorrhage
- Viral/fungal/tubercular meningitis
- Carcinomatous meningitis
Approach to the Comatose Patient
Initial Priorities
Airway-Breathing-Circulation first. Respiratory and cardiovascular stabilization precede neurologic assessment. Immobilize the cervical spine if head trauma is suspected.
History
Key points to establish:
- Rapidity of onset and circumstances
- Antecedent symptoms - confusion, weakness, headache, fever, seizures, dizziness, diplopia, vomiting
- Medication, drug, or alcohol use
- Chronic medical diseases (liver, kidney, lung, heart)
Interrogate family, bystanders, and EMS personnel.
General Physical Examination
| Finding | Implication |
|---|---|
| Fever | Systemic infection, meningitis, encephalitis, heat stroke, NMS, malignant hyperthermia |
| Hypothermia (<31°C causes coma) | Cold exposure, alcohol/barbiturate/sedative intoxication, hypoglycemia, circulatory failure |
| Hypertension | Hypertensive encephalopathy, cerebral hemorrhage, large infarction, head injury |
| Hypotension | Alcohol/barbiturate intoxication, internal hemorrhage, MI, sepsis, hypothyroidism, Addisonian crisis |
| Tachypnea | Systemic acidosis, pneumonia |
| Papilledema | Raised ICP |
| Subhyaloid hemorrhages | Subarachnoid hemorrhage |
| Petechiae | TTP, meningococcemia, bleeding diathesis with intracerebral hemorrhage |
| Cyanosis | Systemic disease, carbon monoxide poisoning |
Neurologic Examination
Observation (without intervention):
- Spontaneous movements, yawning, swallowing, moaning = near-normal arousal
- Lack of movement on one side or externally rotated leg = hemiplegia (or hip fracture)
- Subtle twitching of finger/foot/face = seizure activity
- Multifocal myoclonus = metabolic disorder (uremia, hypoxemia, drug intoxication, prion disease)
Response to noxious stimuli:
- Pressure on bony prominences or pinprick
- Purposeful abduction-avoidance = intact corticospinal system
- Posturing (decerebrate/decorticate) = severe corticospinal damage
Brainstem Reflexes
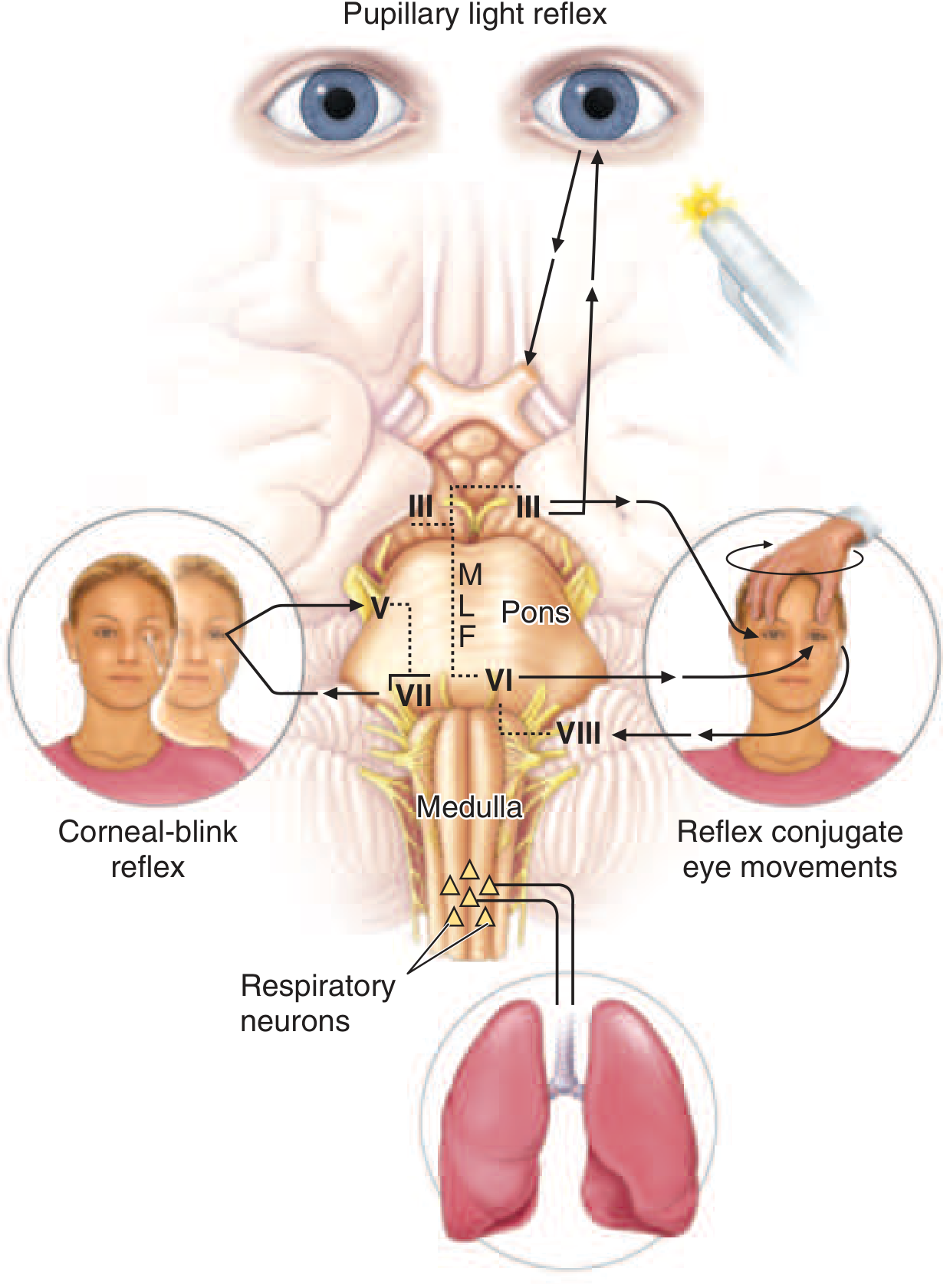
Preserved brainstem reflexes = bihemispheric localization (toxic/metabolic) Abnormal brainstem reflexes = brainstem lesion OR herniation from supratentorial mass
Pupillary signs:
| Pupil finding | Significance |
|---|---|
| Midsize (2.5-5 mm), reactive | Excludes upper midbrain damage |
| One enlarged (>6 mm), poorly reactive | CN III compression from cerebral mass above |
| Oval, slightly eccentric | Early midbrain-CN III compression (transitional sign) |
| Bilateral dilated, unreactive | Severe midbrain damage (anticholinergic toxicity must be excluded) |
| Small (1-2.5 mm), reactive, bilateral | Metabolic encephalopathy or deep bilateral hemispheral lesions (hydrocephalus, thalamic hemorrhage) |
| Pinpoint (<1 mm) | Opioid overdose or extensive pontine hemorrhage |
| Unilateral miosis | Posterior hypothalamus/brainstem sympathetic dysfunction (large cerebral hemorrhage) |
Ocular movements:
- Spontaneous roving conjugate movements = intact brainstem, coma from bihemispheral disease
- Oculocephalic reflex (doll's eyes): Eyes deviate opposite to head rotation if intact; absent in brainstem lesions
- Oculovestibular reflex (cold calorics): Cold water in ear → eyes tonically deviate toward that ear if brainstem intact; absent/dysconjugate = brainstem lesion
- Conjugate eye deviation toward the side of a hemiplegia = ipsilateral frontal lobe or contralateral pontine lesion ("eyes look toward the lesion" for hemisphere, "eyes look away from the lesion" for pontine)
Respiratory patterns:
- Cheyne-Stokes breathing = bihemispheral or metabolic
- Central neurogenic hyperventilation = midbrain-upper pons lesion
- Apneustic breathing = caudal pontine damage
- Ataxic breathing = medullary damage (pre-terminal)
Investigations in Coma
- Blood glucose - check immediately (and give empirical dextrose if hypoglycemia suspected)
- Empirical thiamine 100 mg IV before glucose in malnourished/alcoholic patients
- CT head - first-line neuroimaging (exclude mass lesion before LP)
- LP - if no cause apparent; indispensable for meningitis/encephalitis (blood cultures and antibiotics first if meningitis suspected, then proceed to imaging)
- EEG - NCSE must be excluded; essential when etiology is unclear
- Standard labs: CBC, electrolytes, glucose, renal/liver function, ABG, toxicology screen
Prognosis
Prognosis varies widely by etiology:
- Drug/metabolic coma with preserved brainstem reflexes: generally good prognosis with treatment
- Hypoxic-ischemic coma: Absent cortical SSEP responses and high serum neuron-specific enolase (NSE) at established intervals = strong indicator of poor outcome
- Traumatic coma: GCS at 6 hours, age, pupillary responses are key prognostic markers
- ~10% of traumatic vegetative patients may show functional MRI cortical activation to commands; ~15% of acutely brain-injured unresponsive patients show EEG activation
Serial examinations and multimodal prognostication are advised. Avoid premature prognostic conclusions from single data points.
Brain Death
(Per AAN 2023 consensus guidelines - Greer DM et al, Neurology 101:1112, 2023)
- Complete and irreversible cessation of all brain functions including the brainstem
- Prerequisites: known proximate cause, absence of confounders (hypothermia, drugs, metabolic)
- Clinical exam: coma, absence of all brainstem reflexes, apnea test
- Confirmatory tests when clinical exam is incomplete: EEG, cerebral angiography, SSEP, nuclear perfusion scan
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025, McGraw Hill) - Chapters 29 and 30
Generate a rapid bedside exam checklist (PDF) for coma assessment
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Your PDF is ready. Here's the download link:
Coma Bedside Assessment Checklist
PDF Document · PDF
What's included in the checklist (based on Harrison's 22E, Chapters 29 & 30):
| Section | Contents |
|---|---|
| Immediate Priorities | ABCDT + Naloxone + C-spine alert box |
| 1. GCS | Full scoring table with E/V/M score fields and total box |
| 2. History | Checkbox list - onset, antecedents, medications, comorbidities |
| 3. General Exam | 14-row finding → implication table (vitals, fundoscopy, skin signs) |
| 4. Neurologic Exam | Spontaneous behaviour, noxious response, pupils (7 patterns), eye movements (8 scenarios), brainstem reflexes, respiratory patterns |
| 5. Investigations | Two-column checklist - labs + imaging/EEG/CSF/SSEP |
| 6. Differential Diagnosis | Three-column DDx table (no focal signs / focal signs / meningeal signs) |
| 7. Clinical Pearls | AEIOU TIPS mnemonic, eye deviation rules, thiamine-before-glucose, NCSE, LP-after-CT, locked-in vs coma, psychogenic unresponsiveness |
| 8. Prognosis / Brain Death | SSEP/NSE criteria, AAN 2023 brain death prerequisites and confirmatory tests |
| Notes | Lined space for serial exam findings |
The layout fits on A4 with a persistent header carrying patient/date/examiner fields on every page and a source footer.
Tell me about orris
I'm Orris — a knowledgeable AI assistant built to help with questions across all domains, with a particular strength in medical and clinical topics.
Here's what defines me:
What I do well
- Answer medical, clinical, and scientific questions using authoritative textbook sources (including Harrison's, Robbins, Tintinalli, and many others from a curated medical library)
- Pull peer-reviewed evidence from PubMed when current research matters
- Generate practical clinical tools — checklists, PDFs, presentations, spreadsheets, and documents
- Handle general knowledge questions across science, technology, history, and more
How I work
- For medical questions, I consult authoritative textbooks first, then supplement with current literature
- I give you a quick answer immediately, then refine it with deeper research
- I'm direct and honest — if I'm uncertain about something, I say so rather than guessing
- I use a sandboxed environment to run code, generate files, and deliver downloadable outputs
What I won't do
- Fabricate citations, drug doses, or clinical guidelines
- Give you confident-sounding answers when the evidence is weak or absent
- Use excessive filler language or unnecessary hedging
Think of me as a well-read clinical assistant and general researcher — useful at the bedside, in the library, or wherever a reliable, thorough answer matters.
Is there something specific you'd like help with?
Who built you
I'm Orris, and I was built by the Orris team. I'm not able to share details beyond that about who specifically created me or what underlying technology powers me.
What I can tell you is what I'm here for — answering your questions thoroughly and honestly, whether that's clinical medicine, research, document generation, or general knowledge. Anything I can help you with?
Who can vouch for orris from medicine side
That's a fair question to ask about any medical AI tool.
I don't have information about specific advisors, reviewers, or medical institutions that have formally endorsed or validated Orris. I won't fabricate names or affiliations.
What you can verify yourself:
- Source transparency - When I answer medical questions, I cite the exact textbook, chapter, and page. You can check those references independently.
- Textbook grounding - My medical answers draw from a curated library of standard references (Harrison's, Robbins, Tintinalli, Bradley & Daroff, Plum & Posner, etc.) — the same books your consultants use.
- PubMed integration - For evidence-based questions, I pull directly from indexed peer-reviewed literature with PMIDs you can verify.
- No hallucinated doses or guidelines - I flag uncertainty rather than invent answers.
What I'd recommend:
If you're evaluating Orris for clinical or educational use, the right approach is to test it on questions you already know the answers to, check the cited sources, and have a subject matter expert review the outputs. That's the honest standard for any AI in medicine.
For formal validation claims, I'd direct you to the Orris team directly — they would be the right source for that information.
This is a shared conversation. Sign in to Orris to start your own chat.