GIVE ME A PATIENT SCENARIO AND SOLVE RTHE CASE
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have excellent source material from Harrison's and Braunwald's to construct and solve a comprehensive STEMI case. Let me build this out fully.
🫀 Clinical Case: "The Man Who Walked in From the Parking Lot"
🟥 PATIENT PRESENTATION
Patient: Mr. Ahmad K., 58-year-old male
Setting: Emergency Department, 10:15 AM
Chief Complaint
"Crushing chest pain for the last 90 minutes — it started while I was driving here."
History of Present Illness (HPI)
Mr. Ahmad, a 58-year-old male with a known history of hypertension, type 2 diabetes, and heavy smoking (30 pack-years), presents to the ED with sudden-onset severe substernal chest pain rated 9/10, described as heavy and crushing, radiating to his left arm and jaw. Associated with diaphoresis, nausea, and mild dyspnea.
- Onset: 90 minutes ago while driving
- No positional change with pain; no pleuritic component
- No prior episodes like this
- Last took metformin and amlodipine this morning
Past Medical History
| Condition | Detail |
|---|---|
| Hypertension | On amlodipine 5 mg OD |
| Type 2 Diabetes | On metformin 1000 mg BD |
| Dyslipidemia | Not on statin (non-compliant) |
| Smoking | 30 pack-years, still active |
Family history: Father died of MI at age 62.
Physical Examination
| Finding | Value |
|---|---|
| BP | 148/94 mmHg |
| HR | 98 bpm, regular |
| RR | 20/min |
| SpO₂ | 95% on room air |
| Temp | 37.1°C |
| General | Diaphoretic, anxious, clutching chest |
| Cardiovascular | S1, S2 present; no S3/S4; no murmurs |
| Lungs | Mild bibasal crackles |
| JVP | Mildly elevated (~8 cm) |
| Abdomen | Soft, non-tender |
| Extremities | No peripheral edema |
🟨 INVESTIGATIONS
12-Lead ECG (done within 5 minutes of arrival)
ST-segment elevation of 3–4 mm in leads II, III, aVF Reciprocal ST depression in leads I and aVL Sinus rhythm at 98 bpm
Labs (Initial)
| Test | Result | Reference |
|---|---|---|
| hs-Troponin I (T=0) | 2.8 ng/L | < 0.04 ng/L |
| hs-Troponin I (T=1h) | 18.6 ng/L | < 0.04 ng/L (rising = active MI) |
| CK-MB | 32 U/L | < 25 U/L |
| CBC | WBC 11.2, Hgb 13.8, Plt 245 | Normal |
| BMP | Na 138, K 4.1, Cr 1.1, Glucose 214 | Glucose elevated |
| Lipids | LDL 4.8 mmol/L, HDL 0.8 mmol/L | LDL markedly elevated |
| BNP | 490 pg/mL | < 100 pg/mL |
Chest X-Ray
Mild pulmonary vascular congestion; no pneumothorax; cardiothoracic ratio borderline
🟩 DIAGNOSIS
Acute Inferior STEMI (ST-Elevation Myocardial Infarction) Likely culprit vessel: Right Coronary Artery (RCA)
Reasoning
| Feature | Supports STEMI |
|---|---|
| ST elevation in II, III, aVF | Inferior territory → RCA distribution |
| Reciprocal ST depression in I, aVL | Classic reciprocal changes confirming true elevation |
| Troponin rising serially | Myonecrosis confirmed |
| Crushing chest pain + diaphoresis | Classic ischemic presentation |
| Multiple risk factors (HTN, DM, smoking, dyslipidaemia) | High pre-test probability |
| Elevated BNP + crackles | Early LV dysfunction from infarction |
ECG Criteria Used (Universal Definition of MI):
New ST-elevation at the J-point in ≥2 contiguous leads: ≥0.1 mV in all leads except V2–V3, where ≥0.2 mV is required in men ≥40 years. — Harrison's Principles of Internal Medicine, 22e, Table 286-2
🟦 MANAGEMENT
⚡ IMMEDIATE (First 10 minutes — "Time is Muscle")
| Drug | Dose | Rationale |
|---|---|---|
| Aspirin | 300 mg PO (chewed) | Antiplatelet — Class I |
| Ticagrelor | 180 mg PO loading | P2Y12 inhibitor — dual antiplatelet therapy |
| Heparin (UFH) | 60 units/kg IV bolus | Anticoagulation for PCI |
| Oxygen | 2–4 L/min via nasal cannula | SpO₂ 95% → target ≥95% |
| GTN (Nitroglycerin) | 0.4 mg SL, can repeat | Pain relief, venodilation (hold if BP drops or RV infarct suspected) |
| Morphine | 2–4 mg IV PRN | For severe pain unrelieved by GTN |
⚠️ Important: Avoid NSAIDs and glucocorticoids — they impair infarct healing, increase risk of myocardial rupture, and raise coronary vascular resistance. — Harrison's, 22e
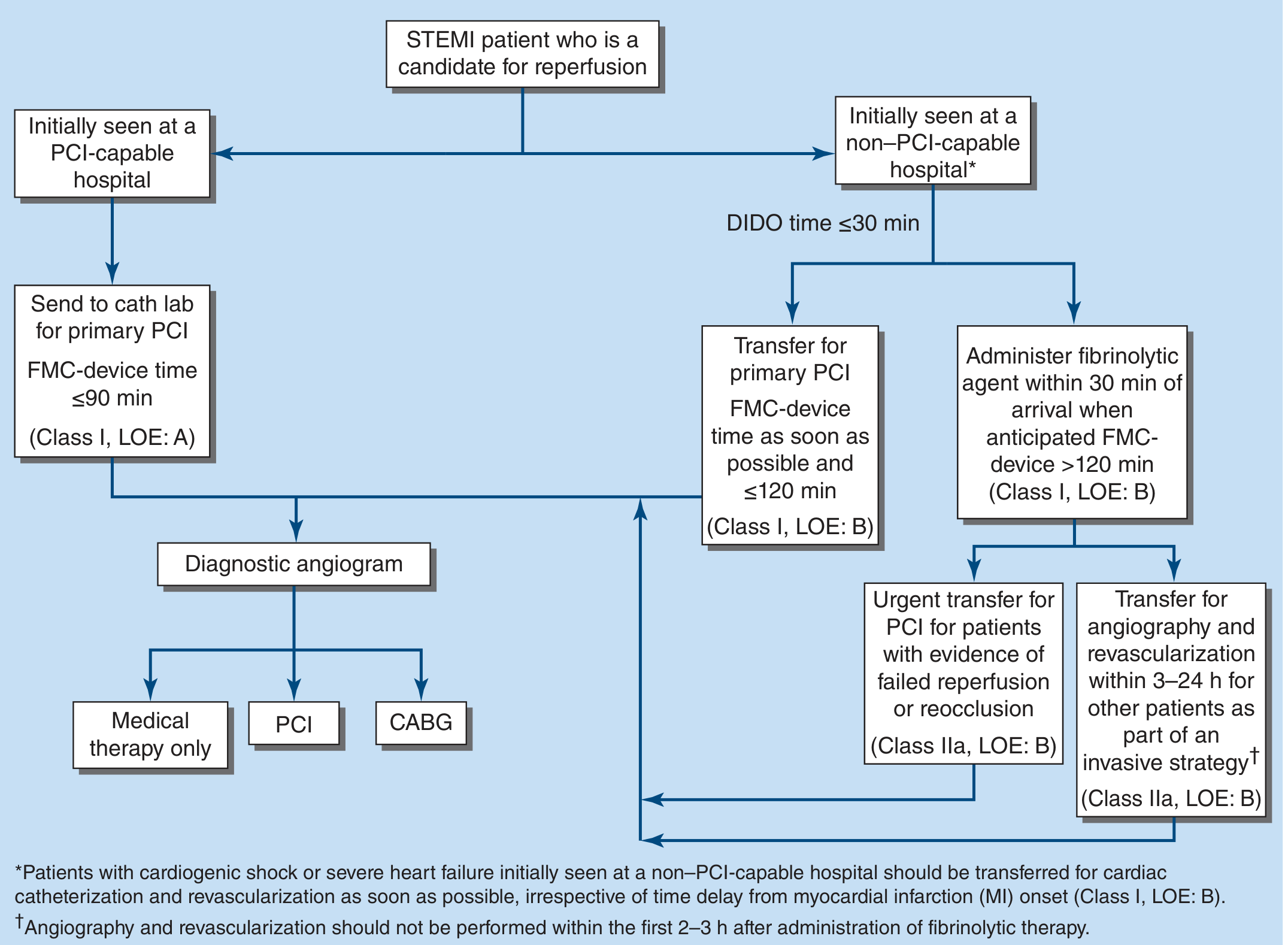
🏥 REPERFUSION STRATEGY
This patient is at a PCI-capable hospital. The goal is:
Primary PCI within 90 minutes of first medical contact (FMC-device time ≤90 min) — Class I, Level of Evidence A — Harrison's Principles of Internal Medicine, 22e, Figure 286-5
Decision:
- Activate Cath Lab immediately
- Target door-to-balloon time: < 90 minutes
- Expected procedure: Coronary angiography → stenting of the occluded RCA
If this were a non-PCI-capable hospital with anticipated FMC-device time >120 min → administer fibrinolytic agent within 30 min of arrival (e.g., tenecteplase), then transfer for angiography within 3–24 hours.
💊 POST-PCI / INPATIENT MANAGEMENT
| Drug Class | Agent | Rationale |
|---|---|---|
| Dual antiplatelet | Aspirin 75–100 mg + Ticagrelor 90 mg BD | Prevent stent thrombosis; continue for ≥12 months |
| Beta-blocker | Metoprolol succinate 25–50 mg OD | Reduces reinfarction risk, limits infarct size, prevents VF |
| ACE inhibitor | Ramipril 2.5 mg OD (titrate up) | Reduces LV remodeling — start within 24h if no hypotension |
| High-intensity statin | Atorvastatin 80 mg OD | Plaque stabilization, LDL reduction — start immediately |
| Anticoagulation | Continue IV heparin for 48h post-PCI | Then discontinue (PCI done) |
| Insulin sliding scale | Correct glucose (currently 214) | Tight glycaemic control post-MI improves outcomes |
Beta-blocker indication criteria: HR >60, SBP >100 mmHg, PR interval <0.24s, no signs of acute HF, no active bronchospasm. — Harrison's, 22e
⚠️ Special caution for inferior STEMI:
- Monitor for right ventricular (RV) infarction (common with RCA occlusion) — obtain right-sided ECG leads (V4R). If present: avoid nitrates (preload-dependent), aggressive IV fluids.
- Watch for bradycardia/heart block (AV node supplied by RCA) — atropine 0.5 mg IV if symptomatic.
📋 MONITORING & FOLLOW-UP
| Parameter | Action |
|---|---|
| Continuous ECG monitoring | 24–48h in CCU for arrhythmias |
| Serial troponins | Confirm peak and trend |
| Echocardiogram | Assess LV function, wall motion abnormalities, EF |
| Repeat ECG post-PCI | Confirm ST resolution (>50% = successful reperfusion) |
| BNP trending | Monitor for decompensating HF |
🔄 DISCHARGE PLANNING
- Medications: DAPT (aspirin + ticagrelor), beta-blocker, ACEi, high-dose statin, metformin (resume after 48h)
- Lifestyle: Smoking cessation (mandatory — refer to cessation program), diabetic diet, cardiac rehabilitation
- Education: Recognize symptoms of recurrent MI, medication adherence
- Follow-up: Cardiology in 4–6 weeks; repeat echocardiogram at 6 weeks to reassess EF
📊 SUMMARY CARD
| Diagnosis | Acute Inferior STEMI (RCA occlusion) |
| Confirm with | ECG (ST↑ in II, III, aVF) + serial troponins |
| Key time target | Door-to-balloon ≤ 90 min |
| Reperfusion | Primary PCI (stenting) |
| Adjunct therapy | DAPT + heparin + beta-blocker + ACEi + statin |
| Key complications to watch | RV infarct, AV block, cardiogenic shock, VF |
| Pitfalls | Don't give nitrates if RV infarct; avoid NSAIDs; check for bradycardia before beta-blockers |
Sources: Harrison's Principles of Internal Medicine, 22e (2025), Table 286-2 & Figure 286-5; Braunwald's Heart Disease, 11e
GIVE ME SOME LATEST GUIDELINES RELATED
Checking Date & Time
Searching PubMed
"myocardial infarction" AND "guideline"
Searching the Web
AHA ACC ESC STEMI guidelines 2024 2025 latest updates
Reading Article
PMID: 40014670
Reading Article
PMID: 40100174
Searching the Web
2025 ACC AHA ACS guideline key changes STEMI NSTEMI dual antiplatelet intravascular imaging radial access
Searching the Web
2025 ACS guideline complete revascularization DAPT duration ticagrelor prasugrel P2Y12 new recommendations site:acc.org OR site:ahajournals.org OR site:clevelandclinic.org
Searching PubMed
"STEMI" AND "complete revascularization" AND "PCI"
I now have everything needed to present a comprehensive, well-cited guideline update. Let me compile it.
📋 Latest Guidelines: Acute Coronary Syndromes (STEMI/NSTEMI)
🏆 Master Reference: 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline
Published: February 27, 2025 | Circulation & JACC Authors: Rao SV, O'Donoghue ML, Ruel M, et al. PMID: 40014670 | DOI: 10.1161/CIR.0000000000001309
This is the most comprehensive update in over a decade, replacing the 2013 STEMI, 2014 NSTEMI, and 2015 PCI guidelines all at once.
🔑 Key Changes & New Recommendations
1. 🩻 Intravascular Imaging to Guide PCI — UPGRADED to Class I
| Old (2021 Revascularization Guideline) | New (2025 ACS Guideline) |
|---|---|
| Class IIa (moderate recommendation) | Class I (strong recommendation) |
What this means for your case: When Mr. Ahmad's RCA was stented, the interventionist is now strongly recommended to use IVUS (intravascular ultrasound) or OCT (optical coherence tomography) to optimize stent placement — ensuring full expansion, correct sizing, and no edge dissection. This reduces stent thrombosis and restenosis.
2. 🖐️ Radial Access Over Femoral — Class I
Recommendation: Transradial (wrist) approach is preferred over transfemoral (groin) for PCI in ACS.
Why: Reduces access-site bleeding, vascular complications, and mortality compared to the femoral approach. This was previously a less definitive recommendation but is now Class I based on accumulating trial data.
3. 🫀 Complete Revascularization — Now Recommended
Recommendation: In STEMI or NSTE-ACS patients with multivessel disease, a complete revascularization strategy is recommended (not just culprit-vessel-only PCI).
This is supported by two landmark trials:
- FULL REVASC / FFR-REACT RCT (NEJM, 2024) — FFR-guided complete revascularization vs. culprit-only in MI: complete strategy reduced major adverse cardiovascular events. [PMID 38587995]
- Network Meta-Analysis, JACC 2025 — Confirmed complete revascularization reduces death and reinfarction in STEMI with multivessel disease. [PMID 39779054]
Timing: Complete revascularization can be staged (within the same hospitalization or shortly after) rather than done all at once.
4. 💊 Dual Antiplatelet Therapy (DAPT) — New Strategies
| Strategy | Recommendation | Class |
|---|---|---|
| Default DAPT | Aspirin + oral P2Y12 inhibitor for ≥12 months | Class I |
| Bleeding risk reduction | 1 month DAPT → ticagrelor monotherapy (drop aspirin) | Class I (NEW) |
| P2Y12 of choice | Ticagrelor or prasugrel preferred over clopidogrel in ACS | Class I |
| Clopidogrel | Only if ticagrelor/prasugrel not tolerated or contraindicated | Class IIa |
Key new Class I: After 1 month of DAPT, dropping aspirin and continuing ticagrelor alone significantly reduces bleeding risk without increasing ischemic events — based on the TWILIGHT and TICO trials.
5. 🩸 High-Sensitivity Troponin Algorithms
Recommendation: Use validated 0h/1h or 0h/2h high-sensitivity troponin (hs-cTn) algorithms for early rule-in/rule-out of MI.
- 0/1h algorithm: Allows rapid discharge or rule-in within 1 hour
- Significantly reduces unnecessary hospital admissions
- Applies directly to Mr. Ahmad's case — his hs-Troponin I rising from 2.8 → 18.6 ng/L over 1 hour is a clear rapid-rule-in pattern
6. 🏥 Cardiogenic Shock — 2025 ACC Expert Consensus
PMID: 40100174 | JACC, April 2025
| Updated Recommendation | Detail |
|---|---|
| Avoid routine IABP | Intra-aortic balloon pump not recommended routinely in cardiogenic shock post-MI |
| MCS devices | Impella or ECMO may be considered for refractory cardiogenic shock (Class IIa) |
| Early invasive strategy | Coronary angiography within 2 hours for cardiogenic shock regardless of hospital type |
| Temperature management | Targeted temperature management no longer routinely recommended post-cardiac arrest |
7. 🧠 Secondary Prevention — Reinforced
| Drug | Recommendation | Class |
|---|---|---|
| High-intensity statin (atorvastatin 40–80 mg) | All post-ACS patients regardless of baseline LDL | Class I |
| ACE inhibitor / ARB | All ACS patients, especially EF < 40% | Class I |
| Beta-blocker | Patients with reduced EF (EF < 40%) or ongoing ischemia | Class I |
| Ezetimibe (add-on) | If LDL not at goal on statin alone | Class I |
| PCSK9 inhibitor | If LDL still not at goal despite statin + ezetimibe | Class I |
| Empagliflozin / Dapagliflozin (SGLT2i) | Post-MI with HFrEF — reduces hospitalisation/death | Class I (NEW) |
| GLP-1 agonists | In post-ACS diabetic patients — cardiovascular benefit | Class IIa |
Note for Mr. Ahmad (diabetic patient): The upgrade of SGLT2 inhibitors to Class I is directly relevant — initiate empagliflozin or dapagliflozin before discharge given his diabetes and mildly elevated BNP suggesting early HF.
8. ⏱️ Door-to-Balloon Time Targets — Unchanged but Reinforced
| Scenario | Target |
|---|---|
| PCI-capable hospital | FMC-to-device ≤ 90 min (Class I, LOE: A) |
| Non-PCI hospital, transfer possible | FMC-to-device ≤ 120 min |
| Non-PCI hospital, transfer >120 min | Fibrinolysis within 30 min of arrival |
| Post-fibrinolysis | Angiography at 2–24 hours (intent for PCI) |
📰 Also Relevant: 2024 ESC Chronic Coronary Syndrome Guidelines
For Mr. Ahmad's long-term follow-up, the 2024 ESC Chronic Coronary Syndromes Guideline updated:
- Risk stratification using risk-factor-weighted pre-test probability models
- Emphasis on lifestyle modification + cardiac rehab as Class I
- Non-obstructive coronary disease (MINOCA) now given specific management pathways
🗂️ Quick Reference Card — What Changed for Your STEMI Patient
| Domain | Old Practice | 2025 Update |
|---|---|---|
| PCI guidance | Angiography alone | Intravascular imaging (IVUS/OCT) — Class I |
| Access site | Femoral or radial | Radial preferred — Class I |
| Multivessel disease | Culprit-only often | Complete revascularization — recommended |
| DAPT reduction | Aspirin backbone | 1 month DAPT → ticagrelor monotherapy — Class I |
| Diabetes post-MI | Metformin only | Add SGLT2i — Class I |
| Troponin testing | Serial at 0/3/6h | hs-Troponin 0h/1h algorithm |
| Cardiogenic shock | Routine IABP | IABP not routine; MCS devices selectively |
📚 Source Papers
| Guideline | PMID | Journal | Year |
|---|---|---|---|
| 2025 ACC/AHA/ACEP/NAEMSP/SCAI ACS Guideline | 40014670 | Circulation | 2025 |
| 2025 ACC Expert Consensus — Cardiogenic Shock | 40100174 | JACC | 2025 |
| Complete vs Culprit-Only PCI Meta-Analysis | 39779054 | JACC | 2025 |
| FFR-Guided Complete Revascularization RCT (NEJM) | 38587995 | NEJM | 2024 |
COMPARE ANY TWO TEXT BOOKS SIDE BY SIDE
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.