H pylori treatment
Reading File
Searching PubMed
Helicobacter pylori treatment eradication
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is the full evidence-based answer:
Helicobacter pylori Treatment
Goals of Therapy
The aim is complete bacterial eradication, defined as a negative test ≥4 weeks after finishing all antibiotics. Successful eradication reduces peptic ulcer recurrence from 50-90% down to <5%, and meaningfully lowers gastric cancer risk. - Goldman-Cecil Medicine, p. 1449
First-Line Regimens
Selection depends on local clarithromycin resistance rates:
If clarithromycin resistance <15% (e.g., Northern Europe, North America)
PPI Triple Therapy - 14 days (preferred over 7-day courses)
| Drug | Dose |
|---|---|
| PPI (e.g., omeprazole) | 40 mg twice daily |
| Clarithromycin | 500 mg twice daily |
| Amoxicillin | 1 g twice daily |
| Or Metronidazole (if penicillin allergy) | 500 mg twice daily |
- Double-dose PPI improves eradication rates by ~10% - Goldman-Cecil Medicine, p. 1449
If clarithromycin resistance >15% (or resistance rates unknown)
Bismuth-Based Quadruple Therapy - 14 days (achieves ~85-90% eradication)
| Drug | Dose |
|---|---|
| PPI | 20-40 mg twice daily |
| Bismuth subsalicylate | 525 mg four times daily |
| Metronidazole | 250-500 mg four times daily |
| Tetracycline | 500 mg four times daily |
Non-Bismuth Quadruple (Concomitant) Therapy - 14 days (alternative when bismuth unavailable)
| Drug | Dose |
|---|---|
| PPI | 40 mg twice daily |
| Clarithromycin | 500 mg twice daily |
| Amoxicillin | 1 g twice daily |
| Metronidazole | 500 mg twice daily |
All four drugs are given simultaneously throughout the full 14-day course. This is the most effective non-bismuth quadruple regimen. - Goldman-Cecil Medicine, p. 1449
Treatment Flowchart
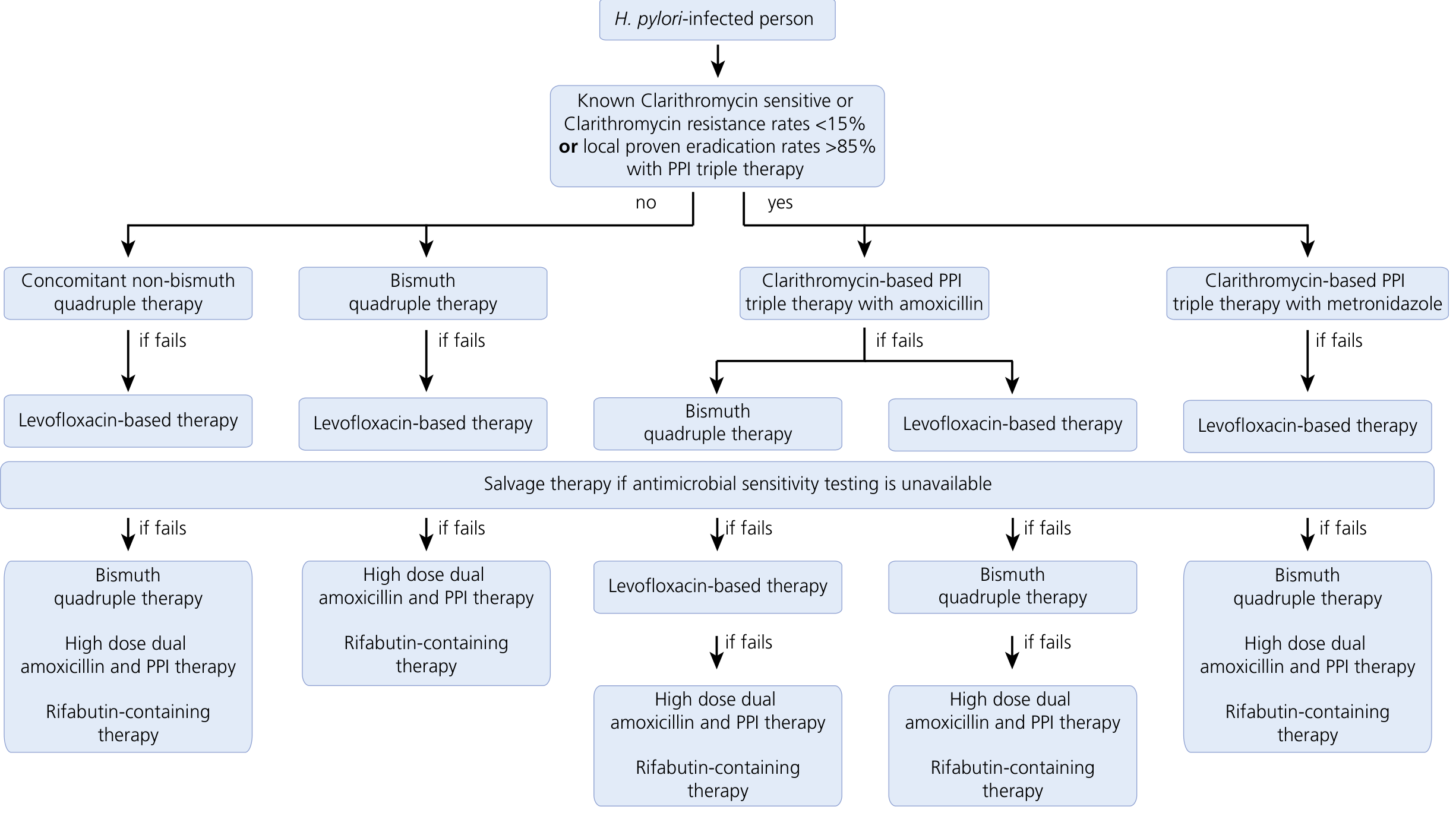
Figure: Therapeutic recommendations for H. pylori eradication based on local resistance patterns - Yamada's Textbook of Gastroenterology, 7th ed.
Second-Line Therapy (After First-Line Failure)
Failure is usually due to resistance to clarithromycin and/or metronidazole - avoid re-using those agents.
- Bismuth quadruple therapy (if not used first-line) - eradicates in ~80% of first-line failures
- Levofloxacin-based triple therapy - PPI + levofloxacin 500 mg once daily + amoxicillin 1 g twice daily for 14 days
Salvage (Third-Line) Therapy
For patients who fail two prior regimens, especially when susceptibility testing is unavailable:
- High-dose dual therapy - high-dose amoxicillin (1 g three to four times daily) + high-dose PPI
- Rifabutin-based triple therapy - PPI + rifabutin 150 mg twice daily + amoxicillin 1 g twice daily (FDA-approved as Talicia: omeprazole + rifabutin + amoxicillin)
At this point, susceptibility-guided therapy via culture or molecular testing is strongly preferred if available. - Yamada's Textbook of Gastroenterology, 7th ed., p. 1089
Key Drug Resistance Notes
| Antibiotic | Resistance Rate |
|---|---|
| Metronidazole | 20-80% worldwide |
| Clarithromycin | 10-50% (rising due to macrolide use for respiratory infections) |
| Levofloxacin | 10-50% in many regions (was rare a decade ago) |
| Amoxicillin | Rare - not clinically significant |
| Tetracycline | Rare - not clinically significant |
Goldman-Cecil Medicine, p. 1449
Confirming Eradication
Always test after treatment in patients with documented PUD or persistent/recurrent symptoms:
- Urea breath test (UBT) - 95% sensitivity and specificity; preferred for post-treatment confirmation
- Stool antigen test - equally acceptable
- Timing: test at least 4-6 weeks after completing all antibiotics AND after stopping PPIs for at least 2 weeks (PPIs cause false-negatives)
- Symptom to Diagnosis, 4th ed., p. 588
Special Considerations
- Vonoprazan (potassium-competitive acid blocker, 20 mg twice daily) can substitute for a PPI and achieves stronger acid suppression; increasingly used particularly in Asia
- Probiotics as add-on to standard therapy hasten symptom resolution and modestly improve eradication rates
- After successful eradication, reinfection risk is <1% per year in most settings
- Continue PPI after antibiotics only if symptoms persist or complicated ulcer disease exists - Goldman-Cecil Medicine, p. 1450
Recent Evidence (2024-2025)
- A 2025 meta-analysis in Gastroenterology (PMID 39824392) confirmed that H. pylori eradication significantly reduces gastric cancer incidence across both RCTs and observational studies - supporting population-wide test-and-treat strategies.
- A 2025 systematic review in Annals of Medicine (PMID 40697099) found that probiotic pretreatment before standard eradication therapy improves eradication rates and reduces adverse effects.
This is a shared conversation. Sign in to Orris to start your own chat.