DD of child with failure to wt gain
Reading File
Finding Sources
Finding Sources
Searching PubMed
"failure to thrive" child differential diagnosis
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
I have enough comprehensive information. Let me compile the full answer now.
Differential Diagnosis: Failure to Thrive (FTT) / Failure to Gain Weight in a Child
Definition: FTT is broadly defined as weight consistently below the 3rd-5th percentile for age, or a sustained drop across 2 major percentile lines on a growth chart. ~90% of cases are nonorganic; ~10% are organic (or mixed).
Classification Framework
FTT is classically divided into three pathophysiologic categories:
| Mechanism | Question to ask | Examples |
|---|---|---|
| Inadequate intake | Is the child getting enough calories? | Psychosocial, feeding errors, poverty, anatomic |
| Inadequate absorption | Can the child absorb what it eats? | Celiac, CF, short gut, SIBO |
| Increased metabolic demand | Is the child burning too much? | CHD, chronic infection, hyperthyroidism, malignancy |
1. NONORGANIC CAUSES (~90%)
- Psychosocial / maternal deprivation - most common overall cause; parental neglect, lack of nurturing, parental depression or mental illness
- Errors in feeding technique - improper formula preparation (over-diluted), incorrect positioning, poor latch (breastfeeding)
- Inappropriate diet - excessive juice, early introduction of solids that displace calories, food restriction by parents
- Poverty / food insecurity - lower socioeconomic status, lower parental education level
- Behavioral feeding disorders - oral aversion, food refusal, sensory processing issues
2. ORGANIC CAUSES (~10%)
Inadequate Caloric Intake
- GERD / esophagitis - feeding refusal, vomiting, pain
- Oropharyngeal dysphagia - cleft palate, cricopharyngeal achalasia, laryngomalacia, choanal atresia
- Congenital heart disease (cyanotic) - fatigue during feeding, increased metabolic demand
- Neurologic disorders - cerebral palsy, hypotonia, neuromuscular diseases (poor suck/swallow)
- Lead poisoning - inner-city environments with older housing stock
- Prematurity - use corrected age on growth charts
Malabsorption / GI Causes
- Celiac disease - anti-tTG antibodies, biopsy; classic presentation with diarrhea, bloating
- Cystic fibrosis - exocrine pancreatic insufficiency, chronic pulmonary infections, sweat chloride test
- Cow's milk protein intolerance / food allergy - rectal bleeding, eczema, failure to gain in infants
- Short bowel syndrome - post-surgical
- Small intestinal bacterial overgrowth (SIBO)
- Chronic diarrhea (any cause) - parasites (Giardia, Cryptosporidium), inflammatory bowel disease
- Pancreatic insufficiency - Shwachman-Diamond syndrome in children
- Lysosomal storage/fat malabsorption disorders - intolerance to breast milk/formula is often first sign
Increased Metabolic Demand / Chronic Disease
- Chronic infections - HIV, TB, recurrent otitis media, UTI, parasites
- Congenital heart disease - especially cyanotic lesions
- Chronic renal disease / renal tubular acidosis - RTA is a classic cause in infants; check BUN/creatinine, urinalysis
- Hypothyroidism - check TSH/T4; also consider hyperthyroidism
- Diabetes mellitus / inborn errors of metabolism - check glucose, metabolic screen
- Malignancy - leukemia, lymphoma
- Obstructive uropathy (UPJO) - FTT is a recognized presentation in infants
Chromosomal / Genetic
- Turner syndrome - short stature, webbed neck, absent breast development
- Trisomy 21 (Down syndrome)
- Prader-Willi, Russell-Silver, Noonan syndromes
- Intrauterine growth restriction (IUGR)
Diagnostic Approach
Key history points: feeding history, stool character, parental heights, psychosocial environment, medications, travel, recurrent infections.
Physical exam: pattern of growth (weight only vs. weight + height vs. all three parameters affected guides diagnosis); dysmorphic features; organomegaly; signs of neglect.
Initial investigations:
- CBC, ESR
- Urinalysis + urine culture (rule out UTI/RTA)
- BUN, creatinine
- TSH, T4
- Serum lead level (inner-city, older housing)
- Liver enzymes
- Bone age radiograph (hand/wrist)
- Stool for ova and parasites
- Based on history: sweat chloride (CF), anti-tTG IgA (celiac), HIV, TB testing
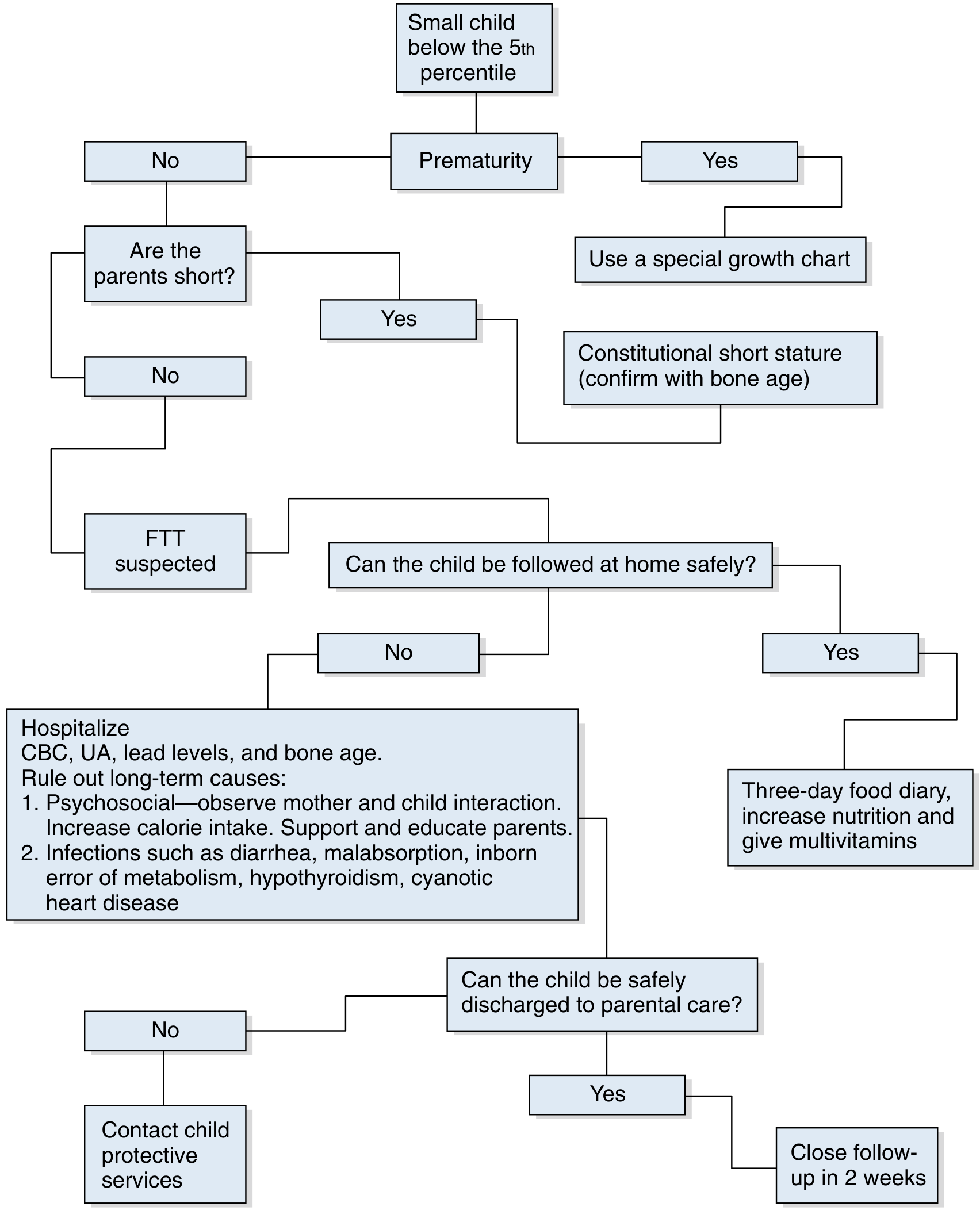
Diagnostic algorithm from Swanson's Family Medicine Review:
Key Pearls
- ~90% of FTT is nonorganic - always assess the psychosocial environment first
- Nonorganic FTT: weight is disproportionately low vs. height; organic FTT affecting all parameters suggests a systemic cause
- Children with a history of FTT remain at increased risk of recurrence even after normalization - long-term follow-up is important
- Appetite stimulants (cyproheptadine, megestrol) are NOT recommended unless significant underlying disease is identified
- Early intervention matters: FTT without treatment causes lasting neurodevelopmental sequelae
- If hospitalized and the child gains weight rapidly, this strongly supports nonorganic (psychosocial) etiology
Sources: Swanson's Family Medicine Review, pp. 557-560; Tietz Textbook of Laboratory Medicine 7e; Swanson's Family Medicine Review Chapter 104
This is a shared conversation. Sign in to Orris to start your own chat.