Dyshidrotic eczema
Reading File
Finding Sources
Finding Sources
Searching PubMed
"dyshidrotic eczema" OR "pompholyx"
Reading File
Reading File
Searching Images
dyshidrotic eczema pompholyx vesicles hands
Reading File
Loading Image
Dyshidrotic Eczema (Pompholyx)
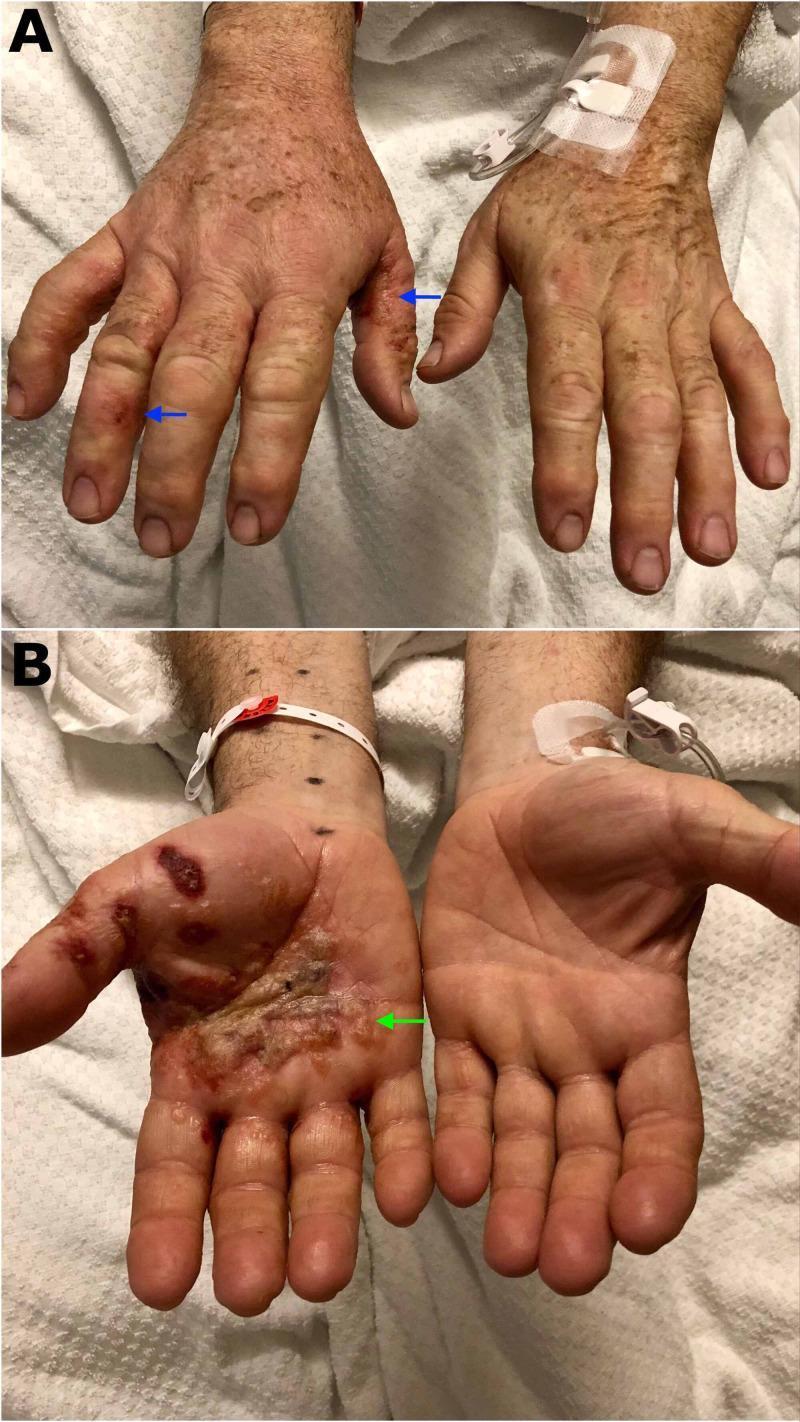
Panel A: Deep-seated vesicles along lateral finger aspects (blue arrows). Panel B: Severe palmar presentation with confluent bullae and crusting (green arrow).
Definition & Overview
Dyshidrotic eczema is a chronic, relapsing palmoplantar eczematous dermatosis characterized by firm, pruritic vesicles and bullae. The vesicles arise from spongiosis within the epidermis; their intact nature reflects the thick, tear-proof stratum corneum at acral sites. It is not an independent disease entity — it is most often a manifestation of atopic dermatitis, or irritant/allergic contact dermatitis.
- Synonyms: Pompholyx (larger vesicles/bullae), acute and recurrent vesicular hand dermatitis
- Epidemiology: Affects all ages; women twice as often as men
Pathogenesis
Despite the misleading name ("dyshidrotic" = disordered sweat), vesicle formation is not linked to sweat gland dysfunction or sweat trapping. Key triggers and associations include:
| Factor | Notes |
|---|---|
| Atopic dermatitis | Most common underlying association; late-stage manifestation |
| Allergic/irritant contact dermatitis | Can cause acute or subacute flares |
| Hyperhidrosis | Aggravating factor; botulinum toxin A for hyperhidrosis may ameliorate DE |
| Ingestants (nickel, cobalt) | Low-nickel diet may help nickel-sensitive patients (positive oral provocation test) |
| IVIg | Can trigger acute episodes |
| Emotional stress | A recognized precipitant |
| Hot climates / sunlight | Rare triggers |
Clinical Features
- Distribution: Symmetric, deep-seated vesicles of the palms, lateral and medial finger aspects, and less commonly soles and toes
- Morphology: Firm, pruritic vesicles initially containing clear fluid; range from pinhead-sized to several centimeters (the larger "pompholyx")
- Tapioca sign: Clustered small vesicles resemble tapioca pudding — a classic descriptor
- Evolution: Vesicles rupture → purulent superinfection may occur → resolves via thick, characteristic desquamation
- Prodrome: Itching or burning of hands/feet before vesicles appear
- Minimal variant: Dyshidrosis lamellosa sicca (keratolysis exfoliativa) — no blisters, only small annular collarettes of white scale
Histopathology
Spongiotic dermatitis with micro- and macrovesicle formation within the epidermis. No association with sweat glands is seen. The thick stratum corneum is a clue to the acral location.
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Inflammatory tinea manuum/pedis | KOH prep positive; asymmetric |
| Scabies | Burrows; interdigital spaces; systemic itch |
| Palmoplantar pustular psoriasis | Sterile pustules; associated nail/skin psoriasis |
| Dyshidrosiform pemphigoid | Elderly; serology (anti-BP180/BP230) positive |
| Dyshidrotic cutaneous T-cell lymphoma | Skin biopsy with atypical lymphocytes |
| Erythema multiforme | Target lesions; mucosal involvement |
| Fixed drug eruption | Recurs at same site; drug history |
| Id reaction | Related to distant infection/dermatophytosis |
| Infantile acropustulosis | Children; recurrent pruritic acral pustules |
Treatment
First-line (mild–moderate):
- High-potency topical corticosteroids — mainstay; apply twice daily during flares
- Cold compresses — symptomatic relief of burning/itch
- Greasy emollients — moisturize, protect barrier, prevent fissures
- Cyanoacrylate ("superglue") — seals painful skin fissures
Second-line (refractory/chronic):
- Topical calcineurin inhibitors (tacrolimus, pimecrolimus)
- Topical retinoids
- Phototherapy: Bath PUVA > systemic PUVA; NB-UVB; note that bath PUVA may be less effective in smokers
- Short-course oral corticosteroids — for acute severe flares
- Systemic immunosuppressants: Cyclosporine, oral retinoids for chronic recalcitrant cases
- Botulinum toxin A: Addresses co-existing hyperhidrosis and may reduce flare frequency
Address underlying causes: Patch testing to exclude allergic contact dermatitis; nickel-restricted diet in sensitized patients.
Recent Evidence
Two 2025 systematic reviews are relevant:
- Dupilumab in chronic hand eczema (Asamoah et al., Arch Dermatol Res 2025) — PMID 39976781 — supports dupilumab as an emerging systemic option
- Pediatric chronic hand eczema patterns (Yeung et al., J Cutan Med Surg 2025) — PMID 40008983 — reviews causes and management in children
Sources: Dermatology 2-Volume Set 5e (Bologna et al.); Textbook of Family Medicine 9e; Fitzpatrick's Dermatology, 9e
This is a shared conversation. Sign in to Orris to start your own chat.