Slight st depression in v1 and v5 marked right axis devation in Cad patient
Reading File
Finding Sources
Finding Sources
Searching the Web
ST depression V1 V5 right axis deviation ECG CAD interpretation posterior MI
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information for a thorough clinical analysis. Here is the full interpretation:
ECG Analysis: ST Depression in V1 & V5 + Marked Right Axis Deviation in a CAD Patient
This ECG pattern carries significant clinical weight in a CAD patient. Below is a systematic breakdown.
1. ST Depression in V1 - Posterior OMI Until Proven Otherwise
In a CAD patient with ischemic symptoms, ST depression in V1 (and V1-V4) is the classic mirror-image of posterior wall (inferobasal) STEMI - not benign subendocardial ischemia.
The posterior wall has no directly overlying leads in a standard 12-lead. When it infarcts, the standard leads record the reciprocal (mirror) picture:
| Posterior Wall Event | What V1-V4 Show |
|---|---|
| ST elevation (injury) | ST depression (horizontal) |
| Q wave (necrosis) | Tall, wide R wave |
| T wave inversion | Upright T wave |
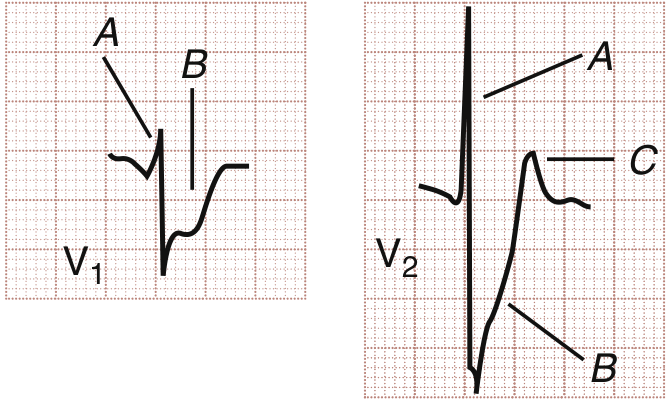
Classic V1/V2 findings of posterior MI (from Rosen's Emergency Medicine):
- Horizontal ST segment depression
- Upright T wave (not inverted - key distinguisher)
- Tall, wide R wave developing over time
- R:S ratio > 1 in V1
Rosen's Emergency Medicine: "ST segment depression in leads V1 to V4 may herald true posterior infarction on the 12-lead ECG. Acute posterior (inferobasal) MI is one entity wherein emergent revascularization is indicated in the absence of ST elevation."
Culprit artery: Most commonly the left circumflex (LCx) coronary artery or a dominant RCA with posterior descending/posterolateral branches. This MI pattern is notoriously under-recognized and often misclassified as "NSTEMI," leading to delayed catheterization.
Do not miss this: ST depression isolated to V1-V4 with upright T waves in a CAD patient = activate posterior leads (V7-V9) immediately. Only 0.5 mm ST elevation in V7-V9 is sufficient to confirm the diagnosis.
2. ST Depression in V5 - Lateral Wall Ischemia
V5 depression adds another critical dimension:
- Lateral wall ischemia (LCx or diagonal/obtuse marginal territory) - consistent with the posterior MI territory, both supplied by LCx
- Could also represent reciprocal change if there is high lateral or anterior wall STEMI (though you'd see elevation elsewhere)
- In the context of V1 depression, V5 depression spreading from V1 to V5 increases suspicion of a large posterior-lateral OMI (LCx occlusion extending to lateral wall)
- A study in PMC confirmed: "ST-segment depression maximal in V1-V4 is specific for occlusion MI (versus nonocclusive ischemia)" - any STD in these leads, even <1 mm, is abnormal
3. Marked Right Axis Deviation (RAD) - Differential in CAD
RAD (QRS axis > +100°, or "marked" when > +120°) in a CAD patient has several explanations:
Harrison's Principles of Internal Medicine (2025): Right axis deviation in CAD can be caused by:
| Cause | Mechanism | ECG Clue |
|---|---|---|
| Left Posterior Fascicular Block (LPFB) | Block of posterior fascicle of LBB, shifts axis rightward | RAD (+90 to +180°), rS in I/aVL, qR in III/aVF, narrow QRS - diagnosis of exclusion |
| Lateral wall MI | Loss of leftward forces from lateral LV | RAD + Q waves in I, aVL, V5-V6 |
| Right Ventricular Strain/RV MI | RV predominance | RAD + ST elevation V1 (RV MI) or RV hypertrophy pattern |
| Pulmonary hypertension (complication) | RV overload | RAD + P pulmonale + S1Q3T3 |
Most relevant in this context:
-
LPFB is the most common isolated cause of RAD in CAD. Harrison's states: "Left posterior fascicular block (QRS axis more rightward than +110-120°) is extremely rare as an isolated finding and requires exclusion of other factors causing right axis deviation." If LPFB is new or changing, it suggests infarction of the posterior fascicle - ischemic territory overlapping with inferior/posterior MI.
-
Lateral MI causing loss of leftward vectors: if V5 depression evolves into Q waves in I, aVL, V5 - this shifts axis rightward.
4. Integrated Clinical Picture in This CAD Patient
Putting V1 depression + V5 depression + marked RAD together:
Most likely scenario: Acute Posterior-Lateral OMI (LCx or dominant RCA occlusion) + Left Posterior Fascicular Block
- LCx occlusion causes posterior wall ischemia (ST depression V1) and lateral ischemia (ST depression V5)
- Involvement of the posterior fascicle (supplied by RCA or LCx) causes LPFB and RAD
- This pattern can occur without any ST elevation on the standard 12-lead, making it an "STEMI equivalent" that is easy to miss
Alternative (must exclude): Inferior STEMI with posterior extension
- RCA occlusion with inferior leads (II, III, aVF) showing ST elevation
- Posterior extension giving V1 depression
- LPFB contributing RAD
- Check inferior leads - if elevation is present, this is inferoposterior STEMI
5. Immediate Management Steps
- 12-lead + posterior leads (V7-V9) - look for even 0.5 mm ST elevation confirming posterior STEMI equivalent
- Right-sided leads (V3R, V4R) - rule out concurrent RV infarction (avoid nitrates if positive)
- Serial ECGs every 15-30 min - evolving changes
- Urgent cardiology/cath lab activation - ST depression in V1-V4 + CAD history is a cath lab trigger regardless of "STEMI" label
- Dual antiplatelet + anticoagulation while workup proceeds
- Troponin serial measurements - though do not wait for results to act
- Bedside echo - regional wall motion abnormalities confirm ischemia territory
- Avoid nitrates until RV infarction is excluded (can precipitate profound hypotension)
Key References
- Rosen's Emergency Medicine, Posterior Leads section (block11)
- Harrison's Principles of Internal Medicine 22E, Bundle Branch Blocks and QRS Complex (block27)
- Meyers et al. (2022): ST depression maximal in V1-V4 is specific for occlusion MI - PMID 35535519
- Emergency Medicine Cases - Posterior MI: among ACS patients with STD isolated to V1-V4, one-quarter had occluded arteries with average time to reperfusion of 29 hours, highlighting the under-recognition problem
Bottom line: In a CAD patient, this ECG combination is a posterior-lateral OMI until proven otherwise. The marked RAD likely reflects LPFB from posterior fascicle ischemia. Activate the cath lab, perform posterior/right-sided leads, and do not let the absence of ST elevation delay intervention.
This is a shared conversation. Sign in to Orris to start your own chat.