Create a very smart technique to interpret ABG. It should be a very simplified version and I should understand ABG really well just by looking at the report. So, create a mental formula.
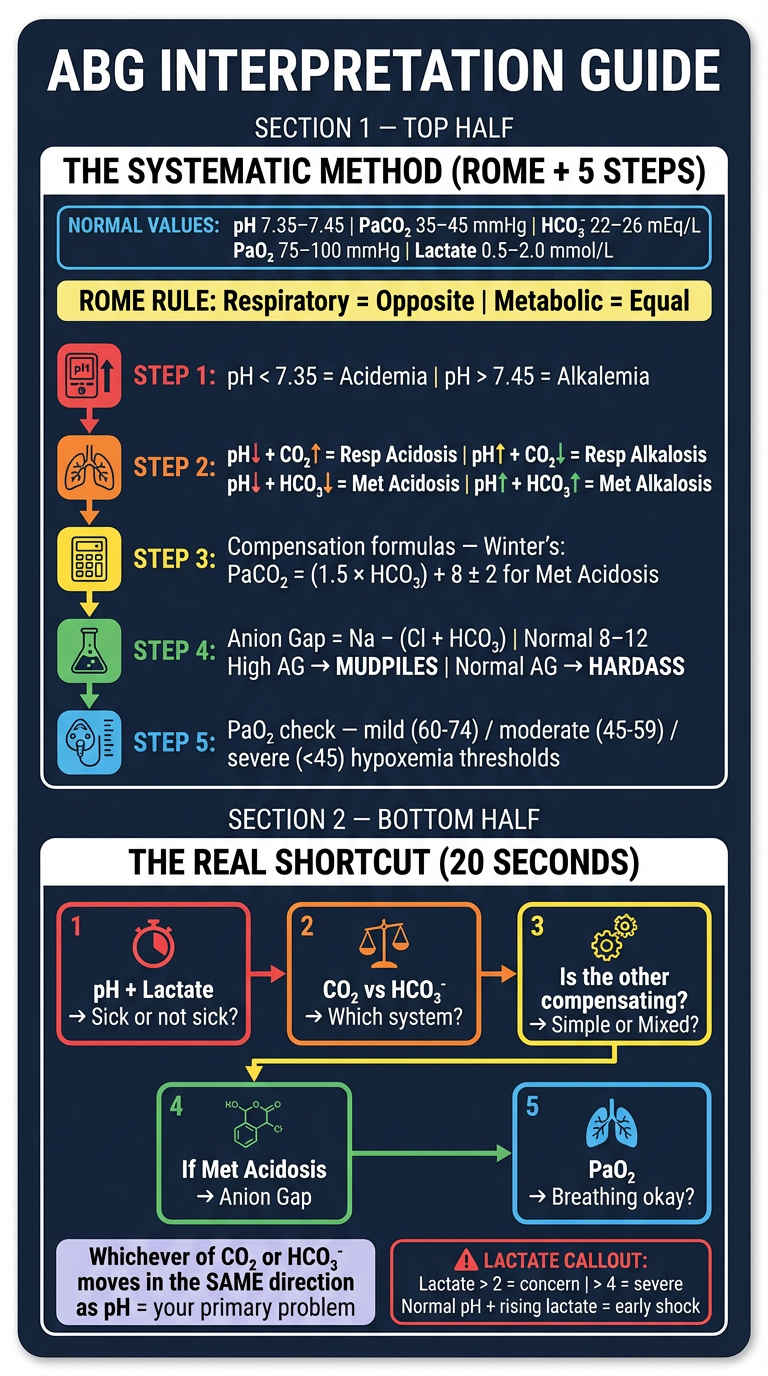
🧠 The ABG Mental Formula — "ROME + 5 Steps"
First: Know the 4 Normal Values by Heart
| Parameter | Normal | Meaning |
|---|---|---|
| pH | 7.35–7.45 | Acid-base balance |
| PaCO₂ | 35–45 mmHg | Respiratory component |
| HCO₃⁻ | 22–26 mEq/L | Metabolic component |
| PaO₂ | 75–100 mmHg | Oxygenation |
The ROME Rule (Memorize This First)
Respiratory = Opposite | Metabolic = Equal
| Disorder | pH | PaCO₂ or HCO₃⁻ |
|---|---|---|
| Respiratory Acidosis | ↓ | PaCO₂ ↑ (opposite) |
| Respiratory Alkalosis | ↑ | PaCO₂ ↓ (opposite) |
| Metabolic Acidosis | ↓ | HCO₃⁻ ↓ (same/equal) |
| Metabolic Alkalosis | ↑ | HCO₃⁻ ↑ (same/equal) |
The 5-Step Mental Formula
Step 1 — Check pH: Is the patient acidic or alkalotic?
pH < 7.35 → ACIDEMIA
pH > 7.45 → ALKALEMIA
pH 7.35–7.45 → NORMAL (but disorder may still exist — keep going!)
Step 2 — Find the culprit: Respiratory or Metabolic?
pH ↓ + PaCO₂ ↑ → Respiratory Acidosis (hypoventilation)
pH ↑ + PaCO₂ ↓ → Respiratory Alkalosis (hyperventilation)
pH ↓ + HCO₃⁻ ↓ → Metabolic Acidosis
pH ↑ + HCO₃⁻ ↑ → Metabolic Alkalosis
Trick: PaCO₂ is the lungs knob. HCO₃⁻ is the kidneys knob. Ask yourself: which knob is turned the wrong way?
Step 3 — Is the body compensating?
- Lung problem → kidneys compensate (slow, hours to days)
- Kidney problem → lungs compensate (fast, minutes to hours)
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic Acidosis | PaCO₂ = (1.5 × HCO₃⁻) + 8 ± 2 → Winter's Formula |
| Metabolic Alkalosis | PaCO₂ = (0.7 × HCO₃⁻) + 20 ± 5 |
| Acute Resp. Acidosis | HCO₃⁻ rises by 1 per 10 mmHg ↑ PaCO₂ |
| Chronic Resp. Acidosis | HCO₃⁻ rises by 4 per 10 mmHg ↑ PaCO₂ |
| Acute Resp. Alkalosis | HCO₃⁻ falls by 2 per 10 mmHg ↓ PaCO₂ |
| Chronic Resp. Alkalosis | HCO₃⁻ falls by 5 per 10 mmHg ↓ PaCO₂ |
Compensation matches prediction → SIMPLE disorder
Compensation doesn't match → MIXED disorder (two things going on)
Step 4 — If Metabolic Acidosis: Calculate the Anion Gap
Anion Gap (AG) = Na⁺ − (Cl⁻ + HCO₃⁻)
Normal AG = 8–12 mEq/L
| AG Result | Type | Common Causes |
|---|---|---|
| AG > 12 (High AG) | Acids piling up | MUDPILES: Methanol, Uremia, DKA, Propylene glycol, Infection/Isoniazid, Lactic acidosis, Ethanol/Ethylene glycol, Salicylates |
| AG normal (Non-AG) | HCO₃⁻ being lost | HARDASS: Hyperalimentation, Acetazolamide, Renal tubular acidosis, Diarrhea, Addison's disease, Spancreatic fistula, Saline infusion |
Albumin correction: If albumin is low, correct AG: Add 2.5 × (4 − albumin) to the measured AG. Low albumin falsely lowers the AG.
Step 5 — Check PaO₂: Is the patient hypoxic?
PaO₂ 75–100 mmHg → Normal
PaO₂ 60–74 mmHg → Mild hypoxemia
PaO₂ 45–59 mmHg → Moderate hypoxemia
PaO₂ < 45 mmHg → Severe hypoxemia (life-threatening)
Don't let a fascinating acid-base picture distract you from hypoxia — it can kill first.
🔑 The Single-Glance Cheat Sheet
Look at pH first
|
< 7.35 = Acidemia > 7.45 = Alkalemia
| |
PaCO₂ ↑? → Resp. Acidosis PaCO₂ ↓? → Resp. Alkalosis
HCO₃⁻ ↓? → Met. Acidosis HCO₃⁻ ↑? → Met. Alkalosis
|
If Met. Acidosis → Calculate Anion Gap
|
If AG High → MUDPILES
If AG Normal → HARDASS (HCO₃⁻ lost)
|
Check compensation → matches? Simple. Doesn't match? Mixed.
|
Always check PaO₂ last
Bonus: Base Excess (BE) — The Shortcut
BE = 0 ± 4 → Normal
BE < −4 → Metabolic acidosis (base deficit)
BE > +4 → Metabolic alkalosis
Quick Practice Example
- pH 7.28 → Acidemia ✓
- HCO₃⁻ ↓ + pH ↓ → Metabolic Acidosis (ROME: equal)
- Compensation check: Winter's → PaCO₂ = (1.5 × 9) + 8 = 21.5 ± 2 → Actual PaCO₂ = 20 ✓ Appropriate → Simple disorder
- Anion Gap = (depends on Na⁺/Cl⁻ — calculate it)
- PaO₂ 98 → Normal
Sources: Current Surgical Therapy 14e, p. 1608 | Barash's Clinical Anesthesia 9e, p. 1158–1159 | Brenner & Rector's The Kidney, p. 704
What about lactate? And how is this a shortcut..?
Lactate on ABG
Normal lactate: 0.5–2.0 mmol/L
Elevated: 2–4 mmol/L → Concern, investigate
High: > 4 mmol/L → Severe lactic acidosis, high mortality risk
| Scenario | Meaning |
|---|---|
| High AG metabolic acidosis + high lactate | Lactic acidosis (Type A = hypoperfusion; Type B = drugs/liver/seizures) |
| High AG + normal lactate | Look elsewhere — DKA, uremia, toxins |
| Normal pH + rising lactate | Compensated shock — act now, don't wait |
On "this isn't a shortcut"
The Real Shortcut: "pH → CO₂ → Bic → Gap" in 20 seconds
| Value | One Question |
|---|---|
| pH | Which side of 7.4 is it on? |
| CO₂ | Does it explain the pH? (same direction = metabolic cause, opposite = respiratory cause) |
| HCO₃⁻ | Does it explain the pH instead? |
| Lactate | Is tissue perfusion failing? |
| PaO₂ | Is the patient hypoxic? |
Whichever of CO₂ or HCO₃⁻ is abnormal in the same direction as the pH disturbance — that's your primary problem.
- pH ↓, CO₂ ↑ → CO₂ is moving opposite to pH → respiratory cause
- pH ↓, HCO₃⁻ ↓ → HCO₃⁻ is moving same as pH → metabolic cause
1. Sick or not sick? → pH + Lactate (30 seconds)
2. Which system? → CO₂ vs HCO₃⁻ (10 seconds)
3. Simple or mixed? → Is the other one compensating? (eyeball it)
4. If met. acidosis: → Anion gap (one calculation)
5. Breathing okay? → PaO₂
Now create image including both
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or missing"
Use generate image tool
A clean, professional medical reference card titled "ABG Interpretation Guide" with two clearly separated sections on a dark navy background with white and colored text. SECTION 1 — TOP HALF: "THE SYSTEMATIC METHOD (ROME + 5 STEPS)" - A colored box showing NORMAL VALUES in a small table: pH 7.35–7.45 | PaCO₂ 35–45 | HCO₃⁻ 22–26 | PaO₂ 75–100 | Lactate 0.5–2.0 - ROME rule in a highlighted banner: "Respiratory = Opposite | Metabolic = Equal" - 5 numbered steps in vertical flow with icons: STEP 1: pH < 7.35 = Acidemia | pH > 7.45 = Alkalemia STEP 2: pH↓ + CO₂↑ = Resp Acidosis | pH↑ + CO₂↓ = Resp Alkalosis | pH↓ + HCO₃↓ = Met Acidosis | pH↑ + HCO₃↑ = Met Alkalosis STEP 3: Compensation formulas — Winter's: PaCO₂ = (1.5 × HCO₃) + 8 ± 2 for Met Acidosis STEP 4: Anion Gap = Na − (Cl + HCO₃) | Normal 8–12 | High AG → MUDPILES | Normal AG → HARDASS STEP 5: PaO₂ check — mild/moderate/severe hypoxemia thresholds SECTION 2 — BOTTOM HALF: "THE REAL SHORTCUT (20 SECONDS)" - A bold flowchart with 5 boxes connected by arrows: Box 1 (red): pH + Lactate → Sick or not sick? Box 2 (orange): CO₂ vs HCO₃⁻ → Which system? Box 3 (yellow): Is the other compensating? → Simple or Mixed? Box 4 (green): If Met Acidosis → Anion Gap Box 5 (blue): PaO₂ → Breathing okay? - A highlighted rule: "Whichever of CO₂ or HCO₃⁻ moves in the SAME direction as pH = your primary problem" - Lactate callout box: Lactate > 2 = concern | > 4 = severe | Normal pH + rising lactate = early shock Clean modern infographic style, high contrast, easy to read at a glance, medical student reference card format.
What is the mudpiles you were talking about
MUDPILES
| Letter | Cause | Mechanism |
|---|---|---|
| M | Methanol | Metabolized to formic acid |
| U | Uremia | Phosphates & sulfates accumulate in renal failure |
| D | Diabetic Ketoacidosis (DKA) | Ketoacids (β-hydroxybutyrate, acetoacetate) |
| P | Propylene glycol / Paracetamol (acetaminophen OD) | Toxic metabolites |
| I | Isoniazid / Iron overdose | Lactic acidosis + direct toxicity |
| L | Lactic acidosis | Tissue hypoperfusion, sepsis, liver failure |
| E | Ethylene glycol (antifreeze) | Metabolized to oxalic acid |
| S | Salicylates (aspirin OD) | Direct acid load + uncoupled oxidative phosphorylation |
When to Think MUDPILES
- L (Lactic acidosis) — sepsis, shock, any critically ill patient
- D (DKA) — diabetes, missed insulin
- M (Methanol) — can cause blindness within hours
- E (Ethylene glycol) — causes renal failure rapidly
Quick Tip to Narrow It Down Further
- Lactate → rules in/out lactic acidosis immediately
- Glucose + ketones → rules in/out DKA
- Osmolar gap (measured osmolality − calculated osmolality) → if > 10, think methanol or ethylene glycol (toxic alcohols raise osmolality before the AG even rises)
No actually I asked about lactate because many times when a patient comes for respiratory distress or chest pain or chest discomfort, so in casualty or emergency room, we usually check ABG for different purposes. So ABG is not just for acidosis-alkalosis, it's a multifoc tool to assess the overall condition of the patient .
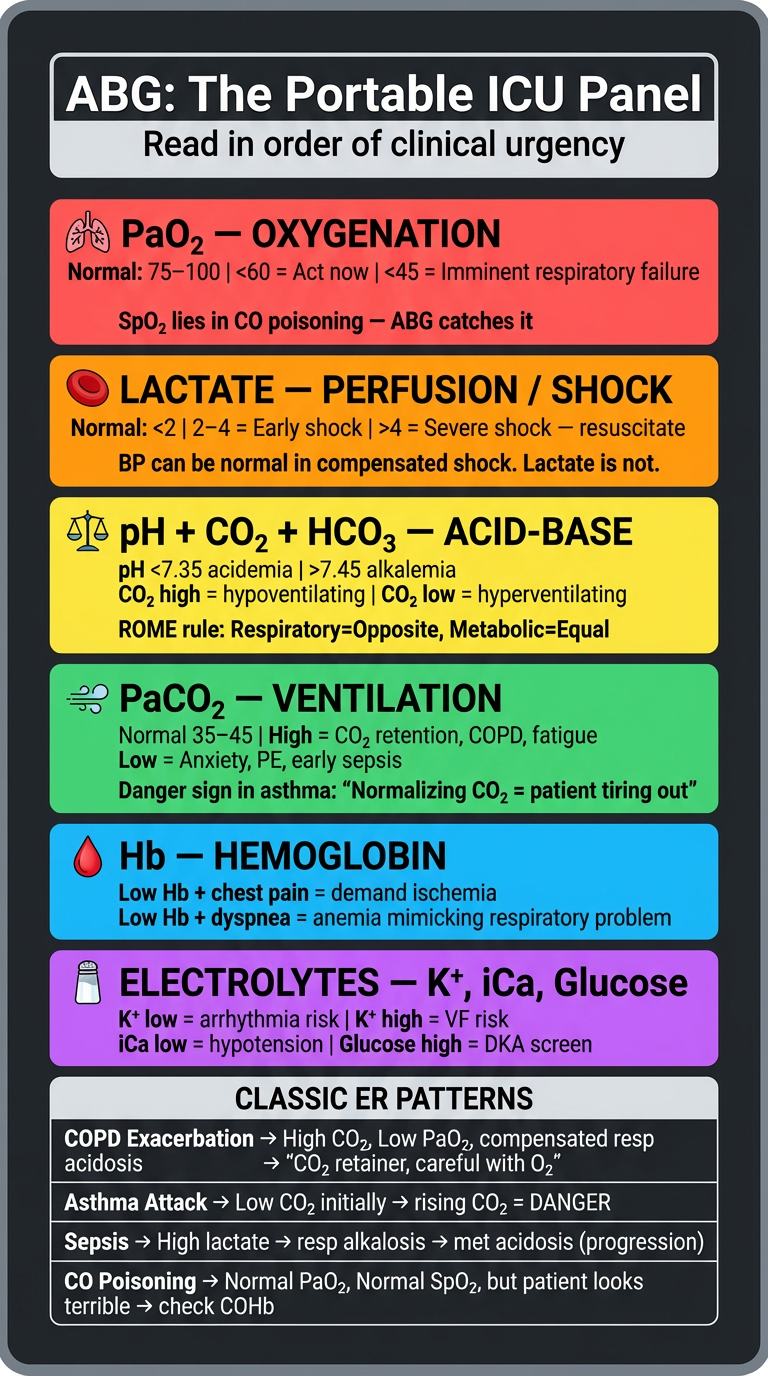
ABG as a Multi-Focal Emergency Assessment Tool
1. 🫁 Ventilation — Is the patient breathing effectively?
PaCO₂ normal (35–45) → Ventilating fine
PaCO₂ ↑ (> 45) → Hypoventilating — CO₂ retention
(COPD exacerbation, fatigue, CNS depression)
PaCO₂ ↓ (< 35) → Hyperventilating — anxiety, pain, PE, early sepsis
2. 🩸 Oxygenation — Is the patient getting enough oxygen?
PaO₂ > 75 → Fine
PaO₂ 60–75 → Mild hypoxemia — watch closely
PaO₂ < 60 → Significant hypoxemia — act now
PaO₂ < 45 → Severe — imminent respiratory failure
Also check SpO₂ vs PaO₂ — if SpO₂ looks okay but PaO₂ is low, suspect CO poisoning (SpO₂ is falsely normal in CO poisoning — ABG catches it).
3. 🔴 Perfusion / Shock — Is tissue being perfused?
Lactate < 2 → Perfusion adequate
Lactate 2–4 → Hypoperfusion — early shock, investigate
Lactate > 4 → Severe shock — aggressive resuscitation needed
This is your shock detector. BP can be normal in compensated shock. Lactate is not.
4. ⚖️ Acid-Base — What is the metabolic state?
- Metabolic acidosis + high lactate → cardiogenic or distributive shock
- Respiratory alkalosis → PE, anxiety, early sepsis (hyperventilating to compensate)
- Respiratory acidosis → COPD exacerbation, acute severe asthma, fatigue
5. 🩸 Hemoglobin — Is the blood carrying enough oxygen?
Hb on ABG → Quick anemia screen
Low Hb + chest pain = demand ischemia from anemia
Low Hb + dyspnea = anemia masquerading as respiratory problem
6. 🧂 Electrolytes — Potassium, iCa, Sodium (on most modern ABG machines)
K⁺ on ABG → Critical in chest pain / arrhythmia
Hypokalemia → arrhythmia risk
Hyperkalemia → peaked T waves, VF risk
iCa ↓ → Post-transfusion, sepsis, causes hypotension
Glucose → Quick DKA/hypoglycemia screen
The ER ABG Reading Framework
1. PaO₂ → Is the patient hypoxic RIGHT NOW?
2. Lactate → Is the patient in shock RIGHT NOW?
3. pH → How sick is the metabolic state?
4. PaCO₂ → Ventilating or tiring out?
5. HCO₃⁻ → Acute or chronic problem?
6. Hb → Is anemia contributing?
7. K⁺ → Arrhythmia risk?
Classic ER Scenarios — What ABG Tells You at a Glance
| Presentation | ABG Pattern | Interpretation |
|---|---|---|
| Chest pain + dyspnea | Low PaO₂, respiratory alkalosis, high lactate | Possible PE or cardiogenic shock |
| COPD exacerbation | High CO₂, low PaO₂, compensated resp. acidosis | CO₂ retainer — careful with O₂ |
| Asthma attack | Initially low CO₂ (hyperventilating) → rising CO₂ = danger sign (tiring out) | Normalize CO₂ = impending respiratory failure |
| Sepsis | High lactate, respiratory alkalosis initially, then met. acidosis | Early → late progression |
| CO poisoning | Normal PaO₂, normal SpO₂, but patient looks terrible | Check COHb on ABG — SpO₂ lies here |
| DKA | Low pH, low HCO₃⁻, high AG, high glucose | Ketoacidosis |
Now create image for this
A professional medical emergency reference card titled "ABG in the Emergency Room — Multi-Focal Assessment Tool" on a dark charcoal background with vibrant color-coded sections. TOP BANNER: Bold white title "ABG: The Portable ICU Panel" with subtitle "Read in order of clinical urgency" MAIN CONTENT — 6 color-coded horizontal sections, each with an icon, parameter name, normal value, and what abnormal means: Section 1 (RED — most urgent): 🫁 PaO₂ — OXYGENATION Normal: 75–100 | <60 = Act now | <45 = Imminent respiratory failure Note: "SpO₂ lies in CO poisoning — ABG catches it" Section 2 (ORANGE): 🔴 LACTATE — PERFUSION / SHOCK Normal: <2 | 2–4 = Early shock | >4 = Severe shock — resuscitate Note: "BP can be normal in compensated shock. Lactate is not." Section 3 (YELLOW): ⚖️ pH + CO₂ + HCO₃ — ACID-BASE pH <7.35 acidemia | >7.45 alkalemia | CO₂ high = hypoventilating | CO₂ low = hyperventilating ROME rule: Respiratory=Opposite, Metabolic=Equal Section 4 (GREEN): 💨 PaCO₂ — VENTILATION Normal 35–45 | High = CO₂ retention, COPD, fatigue | Low = Anxiety, PE, early sepsis Danger sign in asthma: "Normalizing CO₂ = patient tiring out" Section 5 (BLUE): 🩸 Hb — HEMOGLOBIN Low Hb + chest pain = demand ischemia | Low Hb + dyspnea = anemia mimicking respiratory problem Section 6 (PURPLE): 🧂 ELECTROLYTES — K⁺, iCa, Glucose K⁺ low = arrhythmia risk | K⁺ high = VF risk | iCa low = hypotension | Glucose high = DKA screen BOTTOM SECTION — "CLASSIC ER PATTERNS" table with 4 rows: Row 1: COPD Exacerbation → High CO₂, Low PaO₂, compensated resp acidosis → "CO₂ retainer, careful with O₂" Row 2: Asthma Attack → Low CO₂ initially → rising CO₂ = DANGER Row 3: Sepsis → High lactate → resp alkalosis → met acidosis (progression) Row 4: CO Poisoning → Normal PaO₂, Normal SpO₂, but patient looks terrible → check COHb Clean modern infographic, bold readable fonts, dark background, high contrast colors per section, emergency medicine reference card style.
Can you create a simple explanation for ventilator settings and what each setting represents for mental shortcuts.. so its easier for me to understand ventilators
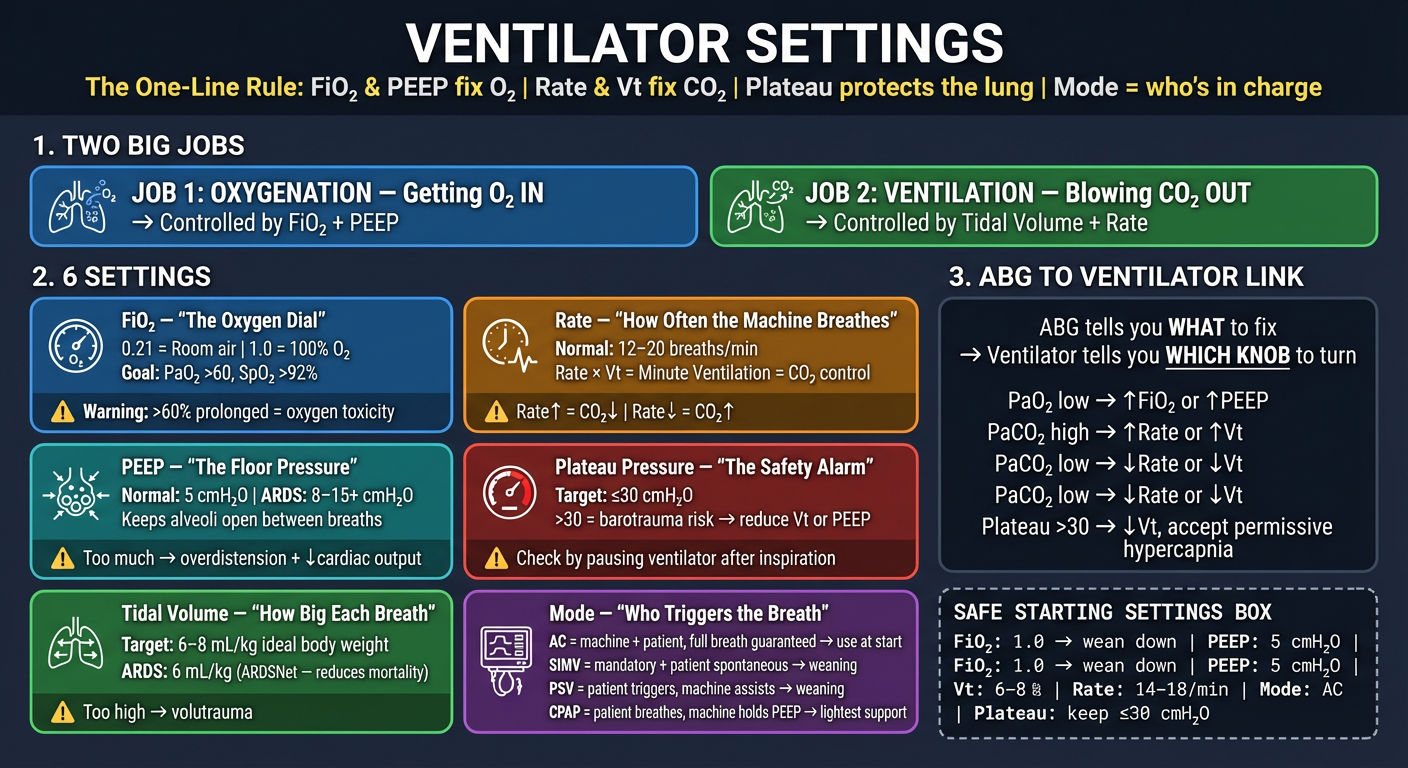
Ventilator Settings — The Simple Mental Model
The Big Picture First
Job 1 — Oxygenation (getting O₂ in) → controlled by FiO₂ and PEEP Job 2 — Ventilation (blowing CO₂ out) → controlled by Tidal Volume and Rate
The 6 Core Settings
1. FiO₂ — Fraction of Inspired Oxygen
FiO₂ 0.21 = Room air (21%)
FiO₂ 1.0 = 100% oxygen
- Turn it up → more oxygen delivered
- Goal: keep PaO₂ > 60 mmHg, SpO₂ > 92%
- Risk: FiO₂ > 60% for prolonged periods → oxygen toxicity, absorptive atelectasis
- Rule: Use the minimum FiO₂ that achieves acceptable oxygenation
2. PEEP — Positive End-Expiratory Pressure
Normal PEEP: 5 cmH₂O (physiologic)
ARDS PEEP: 8–15+ cmH₂O
- Without PEEP → alveoli collapse at the end of each breath → atelectasis → worse oxygenation
- PEEP recruits and keeps alveoli open
- Too much PEEP → overdistension → barotrauma, decreased cardiac output (compresses great vessels)
- PEEP fixes oxygenation. It does NOT fix CO₂.
3. Tidal Volume (Vt) — Volume per Breath
Target: 6–8 mL/kg of ideal body weight
For a 70 kg person: ~420–560 mL per breath
- Too high → volutrauma (lung tears from overdistension)
- Too low → CO₂ retention, atelectasis
- ARDS golden rule: 6 mL/kg — proven to reduce mortality (ARDSNet trial)
4. Respiratory Rate (RR) — Breaths per Minute
Normal setting: 12–20 breaths/min
- Rate × Tidal Volume = Minute Ventilation (how much CO₂ you blow off)
- Rate ↑ → CO₂ ↓ (more blowing off)
- Rate ↓ → CO₂ ↑ (less blowing off)
- CO₂ problem on ABG? Adjust rate or tidal volume, not FiO₂ or PEEP.
5. Plateau Pressure — The Safety Limit
Target: ≤ 30 cmH₂O
- Measured by pausing the ventilator briefly after inspiration
- Reflects the actual pressure inside the alveoli
-
30 cmH₂O → barotrauma risk → reduce Vt or PEEP
- This is your lung protection alarm
6. Ventilator Mode — Who's in Charge of Each Breath?
| Mode | Who Triggers | What's Guaranteed | Use When |
|---|---|---|---|
| AC (Assist-Control) | Machine + patient can trigger; machine delivers full breath either way | Every breath is full preset volume | Newly intubated, deeply sedated, exhausted patient |
| SIMV | Machine gives mandatory breaths; patient can add own breaths in between | Minimum rate guaranteed | Weaning off ventilator |
| PSV (Pressure Support) | Patient triggers only; machine assists each breath with set pressure boost | Patient controls rate | Weaning, spontaneously breathing |
| CPAP | Patient breathes fully spontaneously with continuous positive pressure | Just PEEP maintained | Weaning, mild respiratory failure |
The ABG ↔ Ventilator Connection
PaO₂ low (hypoxia)? → ↑ FiO₂ or ↑ PEEP
PaCO₂ high (CO₂ retained)? → ↑ Rate or ↑ Tidal Volume
PaCO₂ low (blowing off)? → ↓ Rate or ↓ Tidal Volume
Plateau pressure > 30? → ↓ Tidal Volume, accept permissive hypercapnia
The Safe Starting Settings (Adult, 70 kg)
FiO₂: 1.0 initially → wean down rapidly
PEEP: 5 cmH₂O (titrate up in ARDS)
Vt: 6–8 mL/kg ideal body weight (~420–500 mL)
Rate: 14–18 breaths/min
Mode: Assist-Control (AC) initially
Plateau pressure: check and keep ≤ 30 cmH₂O
The One-Sentence Mental Model
FiO₂ and PEEP fix oxygen. Rate and Vt fix CO₂. Plateau pressure protects the lung. Mode decides who's in charge.
— Roberts & Hedges' Clinical Procedures in Emergency Medicine | Current Surgical Therapy 14e | Harrison's Principles of Internal Medicine 22e
Now create image for this
A professional medical reference card titled "Ventilator Settings — Mental Model" on a deep dark navy background with clean white and color-coded text. Modern clinical infographic style. TOP BANNER: Bold white title "VENTILATOR SETTINGS" with a subtitle in yellow: "The One-Line Rule: FiO₂ & PEEP fix O₂ | Rate & Vt fix CO₂ | Plateau protects the lung | Mode = who's in charge" SECTION 1 — TWO BIG JOBS (side by side boxes): Left box (BLUE): "JOB 1: OXYGENATION — Getting O₂ IN" → Controlled by FiO₂ + PEEP Right box (GREEN): "JOB 2: VENTILATION — Blowing CO₂ OUT" → Controlled by Tidal Volume + Rate SECTION 2 — 6 SETTINGS (two columns of 3 cards each, color-coded): Card 1 (BLUE): FiO₂ — "The Oxygen Dial" 0.21 = Room air | 1.0 = 100% O₂ Goal: PaO₂ >60, SpO₂ >92% Warning: >60% prolonged = oxygen toxicity Card 2 (TEAL): PEEP — "The Floor Pressure" Normal: 5 cmH₂O | ARDS: 8–15+ cmH₂O Keeps alveoli open between breaths Too much → overdistension + ↓cardiac output Card 3 (GREEN): Tidal Volume — "How Big Each Breath" Target: 6–8 mL/kg ideal body weight ARDS: 6 mL/kg (ARDSNet — reduces mortality) Too high → volutrauma Card 4 (ORANGE): Rate — "How Often the Machine Breathes" Normal: 12–20 breaths/min Rate × Vt = Minute Ventilation = CO₂ control Rate↑ = CO₂↓ | Rate↓ = CO₂↑ Card 5 (RED): Plateau Pressure — "The Safety Alarm" Target: ≤30 cmH₂O >30 = barotrauma risk → reduce Vt or PEEP Check by pausing ventilator after inspiration Card 6 (PURPLE): Mode — "Who Triggers the Breath" AC = machine + patient, full breath guaranteed → use at start SIMV = mandatory + patient spontaneous → weaning PSV = patient triggers, machine assists → weaning CPAP = patient breathes, machine holds PEEP → lightest support SECTION 3 — ABG TO VENTILATOR LINK (dark box, arrow diagram): "ABG tells you WHAT to fix → Ventilator tells you WHICH KNOB to turn" PaO₂ low → ↑FiO₂ or ↑PEEP PaCO₂ high → ↑Rate or ↑Vt PaCO₂ low → ↓Rate or ↓Vt Plateau >30 → ↓Vt, accept permissive hypercapnia BOTTOM — SAFE STARTING SETTINGS BOX (monospace style): FiO₂: 1.0 → wean down | PEEP: 5 cmH₂O | Vt: 6–8 mL/kg | Rate: 14–18/min | Mode: AC | Plateau: keep ≤30 cmH₂O Clean modern infographic, high contrast, medical ICU reference card style, bold readable fonts, icons for each section.