Post traumatic arthritis
Reading File
Finding Sources
Searching PubMed
"post-traumatic arthritis" AND pathogenesis
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information to compile a thorough overview of post-traumatic arthritis. Let me write the full answer.
Post-Traumatic Arthritis (PTA)
Definition and Epidemiology
Post-traumatic arthritis is a form of secondary osteoarthritis that develops following injury to a joint - including intra-articular fractures, dislocations, ligament tears, or repetitive mechanical trauma. It accounts for approximately 12% of all osteoarthritis cases and is classified under the broader category of secondary OA, where a predisposing condition (prior joint injury) places the joint at risk of progressive cartilage degeneration.
Arthritis as a whole affects about 22% of U.S. adults (~55 million), with OA being the most common form. PTA is one of the more preventable subtypes, as it often follows a specific, identifiable injury event. - Schwartz's Principles of Surgery, 11th Ed.
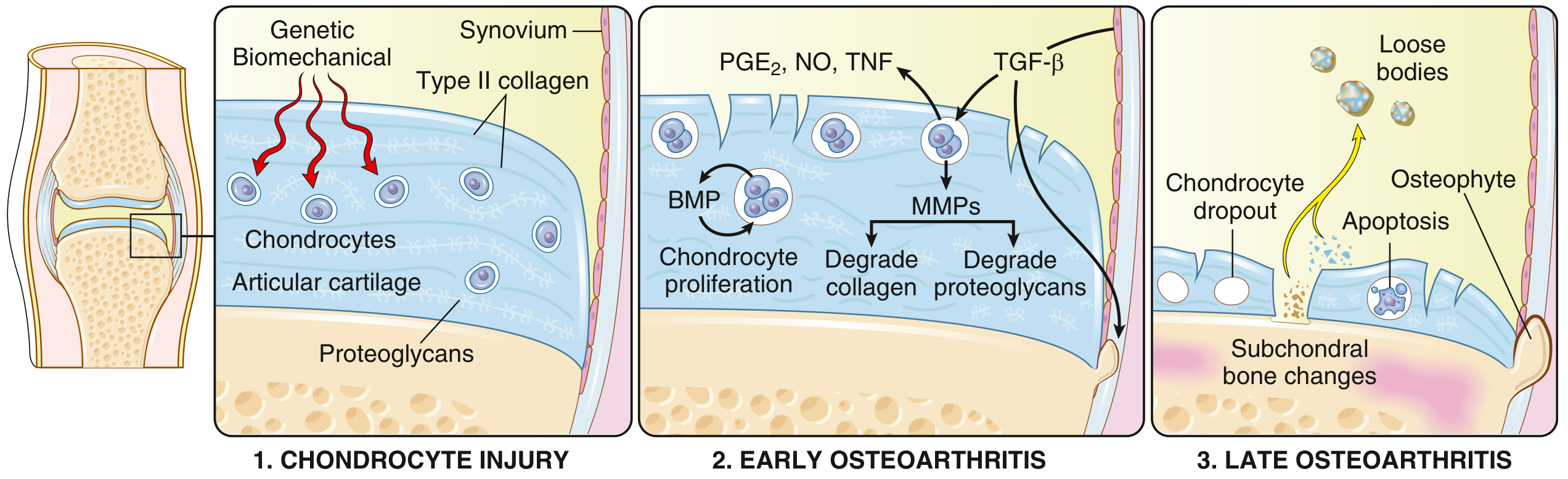
Pathogenesis
PTA shares the fundamental disease mechanism with osteoarthritis but is initiated by a specific traumatic insult:
Stage 1 - Chondrocyte Injury
Biomechanical stress from the initial trauma (fracture, dislocation, repeated impact) injures chondrocytes and disrupts the extracellular matrix of articular cartilage. Genetic factors influencing matrix components can amplify susceptibility.
Stage 2 - Early OA Changes
Injured chondrocytes attempt to repair damaged matrix by proliferating and releasing cytokines and enzymes:
- Matrix metalloproteinases (MMPs) degrade the type II collagen network
- Inflammatory mediators including IL-1, IL-6, TNF, PGE2, and nitric oxide are released by chondrocytes, synovial cells, and recruited macrophages
- TGF-β drives MMP production
- Water content of the matrix increases; proteoglycan concentration falls
- Collagen fibers become cleaved - articular surface develops fissures and clefts, becoming granular and soft
Stage 3 - Late OA
-
Severe chondrocyte loss and full-thickness cartilage sloughing
-
Dislodged fragments form loose bodies (joint mice)
-
Exposed subchondral bone becomes the new articulating surface - friction burnishes it to polished ivory (bone eburnation)
-
Small fractures allow synovial fluid to be forced into subchondral bone in a ball-valve mechanism, forming subchondral cysts
-
Osteophytes (bony outgrowths) develop at joint margins, driven by TGF-β and BMPs
-
Synovium shows mild congestion, fibrosis, and scattered chronic inflammatory cells
-
Robbins & Kumar Basic Pathology, p. 790-791
Causes / Risk Factors for PTA
Secondary OA (including PTA) may arise from:
- Intra-articular fractures (pilon, calcaneus, tibial plateau, distal radius, acetabulum)
- Joint dislocations (hip, knee, ankle)
- Ligament injuries disrupting joint congruity
- Repetitive occupational trauma (miners, carpet layers, shipyard workers)
- Congenital joint abnormalities (acetabular dysplasia, slipped capital femoral epiphysis)
- Neuropathies, metabolic disorders (gout, CPPD, hemochromatosis), and previous inflammatory arthritis
High-impact activity resulting in injury is associated with PTA; repetitive low-impact activity in a normal joint is generally not. - Textbook of Family Medicine, 9e, p. 873
Common Sites
| Joint | Common Preceding Injury |
|---|---|
| Ankle | Pilon/malleolar fractures, ligament tears |
| Knee | Tibial plateau fractures, ACL/meniscal injuries |
| Hip | Acetabular fractures, posterior dislocations |
| Wrist/Distal Radius | Intra-articular distal radius fractures |
| Elbow | Distal humeral fractures, radial head fractures |
| CMC joints (hand) | Metacarpal fractures with delayed treatment |
Clinical Features
Symptoms:
- Joint pain that is activity-related and worsens through the day, relieved by rest
- Morning stiffness < 30 minutes (contrast with > 60 min in RA)
- Gel phenomenon - stiffness after rest, resolving quickly with movement
- Pain may become continuous in advanced disease, including at night
- Buckling or instability (especially knee OA descending stairs)
Signs:
- Joint swelling, tenderness, crepitus
- Bony enlargement at joint margins causing deformity
- Reduced range of motion
- In severe cases: joint instability, locking (loose bodies)
- Mild warmth and effusion may be present; marked erythema/heat suggests septic or crystal arthritis
OA vs RA - Key Comparison
| Feature | Osteoarthritis / PTA | Rheumatoid Arthritis |
|---|---|---|
| Primary mechanism | Mechanical cartilage injury | Autoimmunity |
| Inflammation | Secondary; worsens damage | Primary driver |
| Joints | Weight-bearing (knee, hip, ankle) | Small joints of hands first |
| Pathology | Cartilage degeneration, osteophytes, subchondral cysts | Pannus invasion, joint fusion (ankylosis) |
| Serology | None | ACPA, RF positive |
| Other organs | Not involved | Lungs, heart, etc. |
- Robbins & Kumar Basic Pathology, Table 19.2
Diagnosis
Radiographic Features (X-ray - first-line):
- Osteophyte formation at joint margins
- Asymmetric joint space narrowing (< 3 mm weight-bearing in knee)
- Subchondral bone sclerosis
- Subchondral cysts (late finding) with sclerotic walls
- History of prior fracture or malalignment on imaging
Periarticular osteoporosis and marginal erosions point toward RA rather than OA.
ACR Classification Criteria for Knee OA:
Knee pain PLUS at least 5 of 9: age > 50, stiffness < 30 min, crepitus, bony tenderness, bony enlargement, no palpable warmth, ESR < 40 mm/hr, RF < 1:40, synovial fluid consistent with OA.
Lab Work:
- Usually normal ESR, CRP (mild elevation possible)
- RF and ANA negative
- Synovial fluid: mildly inflammatory (< 2000 WBC/mm³), no crystals
Management
Goal: Pain relief, preserve function, prevent disability - no currently available treatment alters the natural history. - Textbook of Family Medicine, 9e
Nonpharmacologic (First-line)
- Rest during pain episodes
- Exercise - ROM and strengthening; aerobic conditioning
- Weight control (each kilogram lost reduces knee load by ~4 kg)
- Physical and occupational therapy
- Assistive devices (canes, braces, orthotics)
- Patient and family education
Pharmacologic
| Agent | Role |
|---|---|
| Acetaminophen 1000 mg QID | First-line oral analgesic (avoid in liver disease) |
| NSAIDs (ibuprofen, naproxen) | Superior to acetaminophen for pain; add PPI (e.g. omeprazole) if GI risk factors present |
| Topical NSAIDs/capsaicin | Adjunct, limited benefit |
| Intraarticular corticosteroids | Useful when NSAIDs fail or contraindicated; limit to ~4 injections/joint/year |
| Tramadol | Useful adjunct; can reduce NSAID dose needed |
| Opioids | Short-term for acute exacerbations only; avoid long-term |
NSAIDs + PPI remain the pharmacologic backbone for symptomatic management.
Surgical
| Procedure | Indication |
|---|---|
| Osteotomy | Joint realignment; younger patients with unicompartmental disease |
| Arthroscopic debridement/lavage | Mechanical symptoms (loose bodies), selected cases |
| Joint arthroplasty (total/partial) | End-stage disease with functional limitation refractory to conservative care |
| Arthrodesis (fusion) | Salvage for failed arthroplasty, severe instability, young high-demand patients |
Important in PTA specifically: Post-traumatic OA carries higher complication rates after total joint replacement than primary OA. For example, in total ankle arthroplasty (TAA), fracture-related PTA is associated with higher revision rates, periprosthetic bone cysts, valgus malalignment, and risk of prosthesis explant compared to primary OA. Pilon fracture patients have particular risk of talar implant subsidence. - Campbell's Operative Orthopaedics, 15th Ed. 2026, p. 646
For the elbow, post-traumatic arthritis (e.g., after distal humeral fractures) carries reoperation rates ~25% with interposition arthroplasty, versus ~11.7% for inflammatory arthritis. - Campbell's Operative Orthopaedics, 15th Ed. 2026
Prevention
The primary strategy to prevent PTA is anatomic reduction and stable fixation of intra-articular fractures. Even small articular step-offs (> 2 mm) significantly increase PTA risk. Additional strategies:
- Early mobilization post-injury
- Management of malalignment/malunion before secondary arthritic changes develop
- Experimental approaches (e.g., intra-articular IL-1 inhibition post-knee injury) have shown promise in animal models but are not yet standard of care
Recent evidence note: A 2026 systematic review (PMID 41475369) on total elbow arthroplasty for post-traumatic sequelae of distal humeral fractures confirms high rates of acceptable functional outcomes but significant reoperation risk, consistent with the textbook data above.
This is a shared conversation. Sign in to Orris to start your own chat.