Give me a flowchart of pathophysiology of sepsis and septic shock based on Robbins Pathology and Bailey and Love Surgery
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Generating Image
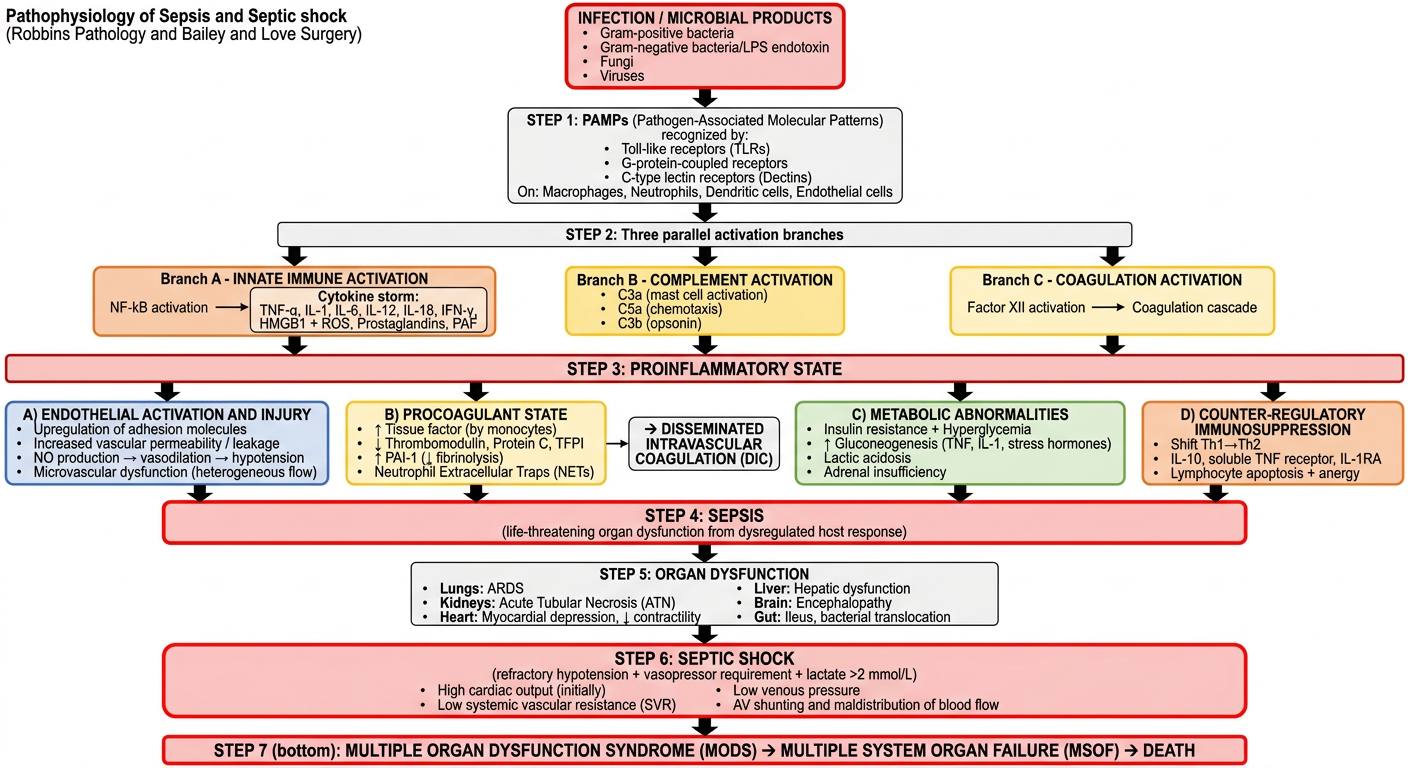
Here is the flowchart, synthesized directly from Robbins, Cotran & Kumar - Pathologic Basis of Disease (Fig. 4.20 and surrounding text) and Bailey and Love's Short Practice of Surgery, 28th Ed. (Chapter 5). Below is the full textual breakdown of the pathway:
Pathophysiology of Sepsis and Septic Shock
1. Trigger: Infection / Microbial Products
- Gram-positive bacteria (most common trigger)
- Gram-negative bacteria (LPS/endotoxin from dying bacilli, e.g. E. coli)
- Fungi, viruses (e.g. SARS-CoV-2)
Bailey & Love: "Serious infection may lead to SIRS through the release of lipopolysaccharide endotoxin from the walls of dying Gram-negative bacilli."
2. Pattern Recognition: PAMPs + PRRs
Microbial PAMPs (and DAMPs from injured cells) engage:
- Toll-like receptors (TLRs) - on macrophages, neutrophils, dendritic cells, endothelium
- G-protein-coupled receptors - detect bacterial peptides
- C-type lectin receptors (Dectins) - detect fungal antigens
This triggers NF-kB nuclear translocation and gene upregulation.
3. Three Parallel Pathogenic Arms (Robbins)
A. Proinflammatory Cytokine Cascade
- TNF-α, IL-1, IL-6, IL-12, IL-18, IFN-γ, HMGB1
- ROS, prostaglandins, platelet-activating factor (PAF)
- Elevated CRP and procalcitonin (acute phase markers)
- Complement activation: C3a (mast cell activation), C5a (chemotaxis), C3b (opsonin)
Bailey & Love: "Cytokines IL-1 and TNF-α stimulate neutrophil adhesion to endothelial surfaces... a respiratory burst occurs releasing lysosomal enzymes, oxidants and free radicals."
B. Endothelial Activation and Injury
- Upregulation of adhesion molecules
- Loosening of tight junctions → vascular leakage, protein-rich edema
- Increased NO production → vascular smooth muscle relaxation → systemic hypotension
- Microvascular dysfunction: heterogeneous capillary flow, AV shunting, loss of autoregulation → O₂ supply/demand mismatch
C. Procoagulant State → DIC
- ↑ Tissue factor expression (monocytes, endothelium)
- ↓ Thrombomodulin, Protein C, TFPI (anticoagulant factors)
- ↑ PAI-1 → impaired fibrinolysis
- Neutrophil Extracellular Traps (NETs) promote both intrinsic and extrinsic coagulation
- Fibrin-rich thrombi in small vessels throughout the body
- In full-blown DIC: consumption of coagulation factors + platelets → paradoxical bleeding
4. Metabolic Derangements (Robbins)
- Insulin resistance + hyperglycemia
- ↑ Gluconeogenesis (driven by TNF, IL-1, glucagon, cortisol, catecholamines)
- Hyperglycemia suppresses neutrophil bactericidal function
- Cellular hypoxia + impaired mitochondrial oxidative phosphorylation → lactic acidosis
- Adrenal insufficiency (from DIC-induced adrenal necrosis - Waterhouse-Friderichsen syndrome)
5. Counter-regulatory Immunosuppression (Robbins)
The hyperinflammatory state triggers opposing mechanisms:
- Th1 → Th2 cytokine shift
- IL-10, soluble TNF receptor, IL-1 receptor antagonist
- Lymphocyte apoptosis and anergy
This creates oscillation between hyperinflammatory and immunosuppressed states.
6. SEPSIS
"Life-threatening organ dysfunction caused by a dysregulated host response to infection" - Robbins Cotran
SIRS criteria (Bailey & Love): ≥2 of: fever/hypothermia, tachycardia/tachypnoea, WBC >12 or <4 × 10⁹/L. Sepsis = SIRS + documented source of infection.
7. Organ Dysfunction (MODS)
| Organ | Effect |
|---|---|
| Lungs | ARDS |
| Kidneys | Acute tubular necrosis (ATN) |
| Heart | ↓ Contractility, myocardial depression |
| Liver | Hepatic dysfunction |
| Brain | Encephalopathy |
| Gut | Ileus, bacterial translocation |
Bailey & Love: "The more organs that fail, the more likely it becomes that death will follow despite all that a modern ICU can do for organ support."
8. Septic Shock
"A subset of sepsis in which profound circulatory, cellular, and metabolic abnormalities are associated with a greater risk of mortality." - Robbins Cotran
Haemodynamic profile (Bailey & Love Table 2.1):
- High cardiac output (early/warm phase)
- Low systemic vascular resistance
- Low venous pressure
- High mixed venous saturation
Later phases: hypovolaemia from fluid extravasation + myocardial depression complicates the picture.
9. MSOF → Death
Vicious cycle: organ failure reduces host defences → further infection → further organ failure. Mortality remains 20-40% despite modern ICU support (Robbins).
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, Fig. 4.20 and pp. 134-137
- Robbins & Kumar - Basic Pathology, pp. 2782-2857
- Bailey and Love's Short Practice of Surgery, 28th Ed., Chapter 5 (pp. 779-800, 4451-4484)
Generate a presentation on the Surviving Sepsis Campaign bundles
Reading File
Finding Sources
Searching PubMed
"Surviving Sepsis Campaign" bundles guidelines
Reading File
Reading File
Searching the Web
Surviving Sepsis Campaign 2021 guidelines 1-hour bundle elements update
Running Command
Writing File
Running Command
Running Command
Your presentation is ready! Here's the download link:
Surviving Sepsis Campaign Bundles
Presentation · PPTX
What's Inside (14 Slides)
| # | Slide | Content |
|---|---|---|
| 1 | Title Slide | Dark navy theme with teal accents |
| 2 | Agenda | 10-topic overview with numbered cards |
| 3 | What is the SSC? | Timeline (2002–2021) + SSC mission & goals |
| 4 | Sepsis-3 Definitions | Infection → SIRS → Sepsis → Septic Shock with diagnostic criteria |
| 5 | Hour-1 Bundle | All 5 elements with colour-coded action panels |
| 6 | Fluid Resuscitation | 30 mL/kg crystalloid, balanced fluids (2021 update), dynamic assessment |
| 7 | Antimicrobials | Timing rules, empiric coverage, source control, stewardship |
| 8 | Vasopressors & Steroids | Full vasopressor table, peripheral IV use (2021 NEW), hydrocortisone, glycaemic control |
| 9 | Lactate & Monitoring | Lactate level tiers with actions, resuscitation targets, screening tools |
| 10 | Sepsis Six | Bailey & Love / UK Sepsis Trust — Give 3 vs Take 3 side-by-side layout |
| 11 | SSC 2021 Key Updates | Comparison table vs 2016 (7 new/changed recommendations) |
| 12 | Outcomes & Evidence | Mortality statistics + ANDROMEDA-SHOCK trial + bundle compliance data |
| 13 | Quick Reference Card | Bedside summary — colour-coded action steps with time targets |
| 14 | Key Takeaways | 8-point summary with references |
Sources used: Bailey & Love Surgery 28e, SSC 2021 International Guidelines (Evans et al., Crit Care Med 2021), SSC Hour-1 Bundle 2018, Robbins Pathology.
This is a shared conversation. Sign in to Orris to start your own chat.