Tell about glaucoma
Reading File
Finding Sources
Searching PubMed
glaucoma diagnosis treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile everything.
Glaucoma - A Comprehensive Overview
Glaucoma is a group of diseases characterized by progressive optic neuropathy, usually associated with elevated intraocular pressure (IOP), leading to characteristic visual field loss and, if untreated, blindness. It is the leading cause of irreversible blindness worldwide.
Aqueous Humor Dynamics (Pathophysiology Foundation)
Understanding glaucoma requires knowing how aqueous humor flows:
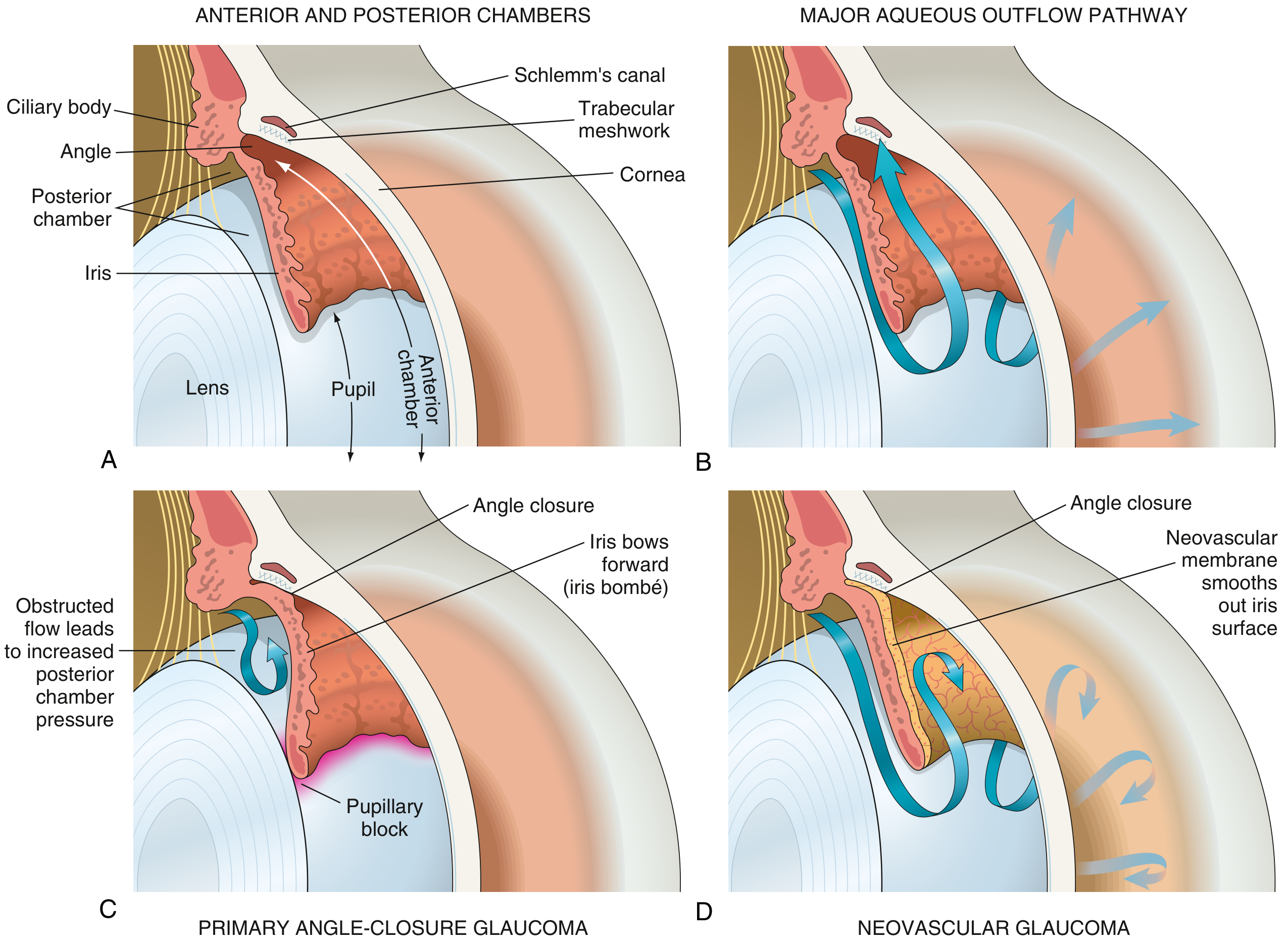
Fig. 21.38 - Robbins & Kumar: (A) Normal eye anatomy. (B) Normal aqueous outflow through trabecular meshwork into Schlemm's canal. (C) Primary angle-closure glaucoma showing iris bombé and pupillary block. (D) Neovascular glaucoma with fibrovascular membrane occluding outflow.
Aqueous humor is produced by the ciliary body, flows from the posterior chamber through the pupil into the anterior chamber, and drains primarily through the trabecular meshwork into Schlemm's canal. Obstruction at any point raises IOP.
Classification
1. Primary Open-Angle Glaucoma (POAG)
The most common type, especially in people of European and African descent.
Definition (Kanski's): A chronic, progressive optic neuropathy of adult onset characterized by:
- Retinal nerve fiber layer (RNFL) thinning
- Glaucomatous optic nerve damage
- Characteristic visual field loss
- Open anterior chamber angle
- No secondary cause
IOP is the key modifiable risk factor, though some patients develop damage at normal pressures (normal-tension glaucoma).
Risk Factors:
| Factor | Details |
|---|---|
| IOP | Higher IOP = greater risk; asymmetry ≥4 mmHg is significant |
| Age | More common in older individuals |
| Race | ~4x more common, earlier onset, harder to control in Black patients |
| Family history | Siblings: 4x risk; offspring: 2x risk |
| Myopia | Increased incidence; more susceptible to damage |
| Vascular disease | Systemic HTN, cardiovascular disease, low ocular perfusion pressure |
| Anti-VEGF therapy | Repeated intravitreal injections (bevacizumab especially) can raise IOP |
| Calcium channel blockers | Meta-analysis shows higher glaucoma prevalence with monotherapy |
| Large optic disc | More vulnerable to IOP-induced damage |
Prevalence:
- Age >70: ~6% in White, ~16% in Black, ~3% in Asian populations
- Affects both genders equally
2. Primary Angle-Closure Glaucoma (PACG)
Most common in hyperopic patients with shallow anterior chambers. The iris obstructs the pupil (pupillary block), building posterior chamber pressure that bows the iris forward (iris bombé), closing the angle and blocking outflow.
Acute angle closure is an ophthalmic emergency:
- Sudden severe eye pain, headache, nausea/vomiting
- Halos around lights
- Blurred vision
- Fixed mid-dilated pupil
- Markedly elevated IOP (can exceed 50-60 mmHg)
- Conjunctival injection, corneal edema
3. Secondary Glaucomas
- Open-angle secondary: Red cells after trauma, necrotic tumor cells blocking trabecular meshwork; pseudoexfoliation syndrome; pigmentary dispersion
- Angle-closure secondary: Neovascular glaucoma (fibrovascular membrane over iris in chronic retinal ischemia - e.g., diabetic retinopathy, CRVO), uveitic glaucoma, lens-induced
- Congenital glaucoma: Trabeculodysgenesis; presents with buphthalmos (enlarged eye), epiphora, photophobia
Optic Nerve Changes
The hallmark of glaucoma is optic nerve cupping:
- Cup/disc (C/D) ratio - normally <0.6; a ratio >0.7 is seen in only 2% of the normal population
- ISNT rule - Normal neuroretinal rim is thickest Inferiorly > Superiorly > Nasally > Temporally; violations suggest glaucoma
- C/D asymmetry ≥0.2 between eyes is suspicious
- RNFL thinning is detectable by OCT before visual field loss
Visual Field Defects
Glaucoma causes characteristic visual field losses (tested with automated perimetry like the Humphrey visual field analyzer):
- Nasal step (respects the horizontal midline)
- Arcuate (Bjerrum) scotoma - arching defect from blind spot
- Paracentral scotoma
- Advanced disease - tubular (tunnel) vision, then total blindness
- The 24-2 pattern is the standard glaucoma-oriented perimetry test; 10-2 monitors advanced cases with split fixation
Diagnosis
Key investigations:
- Tonometry - measures IOP (normal 10-21 mmHg; note diurnal variation)
- Pachymetry - corneal thickness affects IOP reading; thin corneas underestimate, thick overestimate true IOP
- Gonioscopy - directly visualizes the angle; determines open vs. closed
- Fundus examination - dilated optic disc evaluation
- OCT (Optical Coherence Tomography) - quantitative RNFL and ganglion cell complex analysis
- Visual fields (perimetry) - detects and monitors functional loss
Treatment
The only proven treatment is lowering IOP. Even in normal-tension glaucoma, IOP reduction slows progression.
Pharmacological (Topical Eye Drops)
| Drug Class | Examples | Mechanism | Notes |
|---|---|---|---|
| Prostaglandin analogs | Latanoprost, bimatoprost, travoprost | Increase uveo-scleral outflow | First-line; once-daily dosing; SE: iris pigmentation, lash growth |
| Beta-blockers | Timolol, betaxolol, levobunolol | Decrease aqueous secretion | Avoid in asthma, heart block, bradycardia |
| Alpha-2 agonists | Brimonidine, apraclonidine | Decrease secretion + increase outflow | SE: allergy, drowsiness in children |
| Carbonic anhydrase inhibitors | Dorzolamide, brinzolamide (topical); Acetazolamide (oral) | Decrease aqueous secretion | Oral CAIs for acute attacks; SE: paresthesias, metabolic acidosis |
| Cholinomimetics | Pilocarpine, carbachol | Ciliary muscle contraction opens trabecular meshwork | Higher topical SE; used in angle closure |
| Rho kinase inhibitors | Netarsudil | Increase trabecular outflow | Newer agent |
Laser Treatment
- Selective Laser Trabeculoplasty (SLT) - now considered a first-line option for open-angle glaucoma; a 2024 meta-analysis in J Glaucoma confirmed SLT is as effective as medical therapy for open-angle glaucoma/ocular hypertension
- Laser peripheral iridotomy (LPI) - for angle-closure glaucoma; creates a hole in the iris to relieve pupillary block
- Diode laser cyclodestruction - reduces aqueous production by ablating ciliary body; reserved for refractory cases
Surgical Treatment
- Trabeculectomy - creates a new drainage channel (guarded filtration bleb); gold standard surgery; often augmented with mitomycin C
- Glaucoma drainage devices (tube shunts) - e.g., Ahmed, Baerveldt; for complex or refractory cases
- Minimally Invasive Glaucoma Surgery (MIGS) - iStent, OMNI, Hydrus; less risk, modest IOP reduction
- PreserFlo MicroShunt - a 2025 meta-analysis in Graefe's Archive found it comparable to trabeculectomy with a better safety profile
Monitoring and Target IOP
- The concept of a target IOP is individualized - typically 20-30% reduction from baseline, or lower in advanced disease
- OCT and visual fields are repeated every 6-12 months to assess progression
- Glaucoma is a lifelong condition requiring continuous treatment; blindness is preventable with early detection
Special Forms
| Type | Key Feature |
|---|---|
| Normal-tension glaucoma (NTG) | Damage occurs with IOP <21 mmHg; vascular/mechanical factors implicated |
| Pseudoexfoliation glaucoma | Most common identifiable cause of secondary open-angle glaucoma worldwide |
| Pigmentary glaucoma | Iris pigment deposits on trabecular meshwork; young myopic males |
| Neovascular glaucoma | Due to retinal ischemia (diabetic retinopathy, CRVO); very difficult to treat |
| Congenital/Infantile glaucoma | Trabeculodysgenesis; surgery (goniotomy/trabeculotomy) is primary treatment |
| Sturge-Weber syndrome | Glaucoma in ~30%; raised episcleral venous pressure mechanism |
Key Facts Summary
- Glaucoma is the #1 cause of irreversible blindness worldwide
- POAG is often asymptomatic until advanced - hence the name "silent thief of sight"
- The only modifiable risk factor with proven treatment benefit is IOP
- Peripheral vision is lost first; central vision is typically preserved until late
- Optic nerve damage is permanent - treatment only prevents further loss
- Regular screening is important, especially for high-risk groups (age >60, family history, Black ethnicity, high myopia)
This is a shared conversation. Sign in to Orris to start your own chat.