Hiw to check IVC diameter
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete guide to measuring IVC diameter by ultrasound (POCUS/echocardiography), based on authoritative textbooks.
How to Check IVC Diameter
1. Probe and Patient Position
- Patient lies supine
- Use a phased-array or curvilinear (abdominal) probe
- Place the probe at the subxiphoid (subcostal) region, below the xiphoid process, with the indicator toward the patient's head
2. Getting the View
- Start with a subcostal 4-chamber view of the heart (marker toward patient's left, fan toward the liver)
- Rotate the probe counterclockwise and tilt it to align with the IVC in its long axis
- Keep the right atrium in the center of screen during rotation
- Identify the IVC by confirming:
- It enters the right atrium directly
- It connects with the hepatic vein (this confirms it is IVC, not aorta)
The aorta lies just medial to the IVC and can be confused with it - always confirm by seeing the RA junction and hepatic vein connection. - Murray & Nadel's Textbook of Respiratory Medicine
3. Where to Measure
- Measure just proximal to (before) the entrance of the hepatic veins into the IVC, in the subcostal long-axis view
- This is typically 1-2 cm from the RA-IVC junction
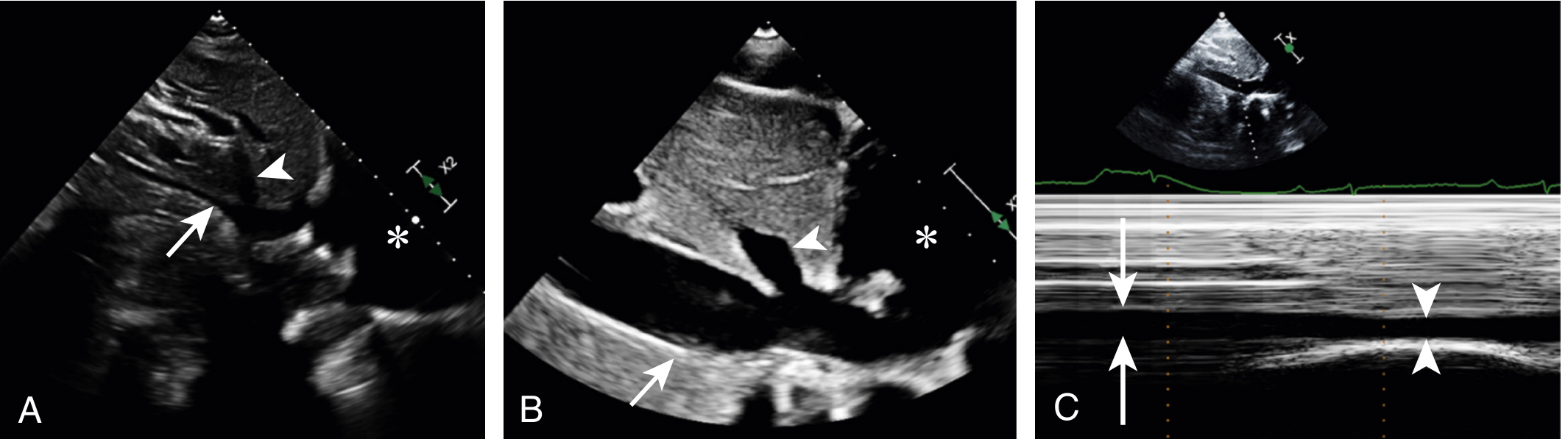
A = small, collapsed IVC (low RA pressure); B = large, dilated IVC (high RA pressure); C = M-mode tracing showing maximum (arrows) and minimum (arrowheads) diameter over respiratory cycle
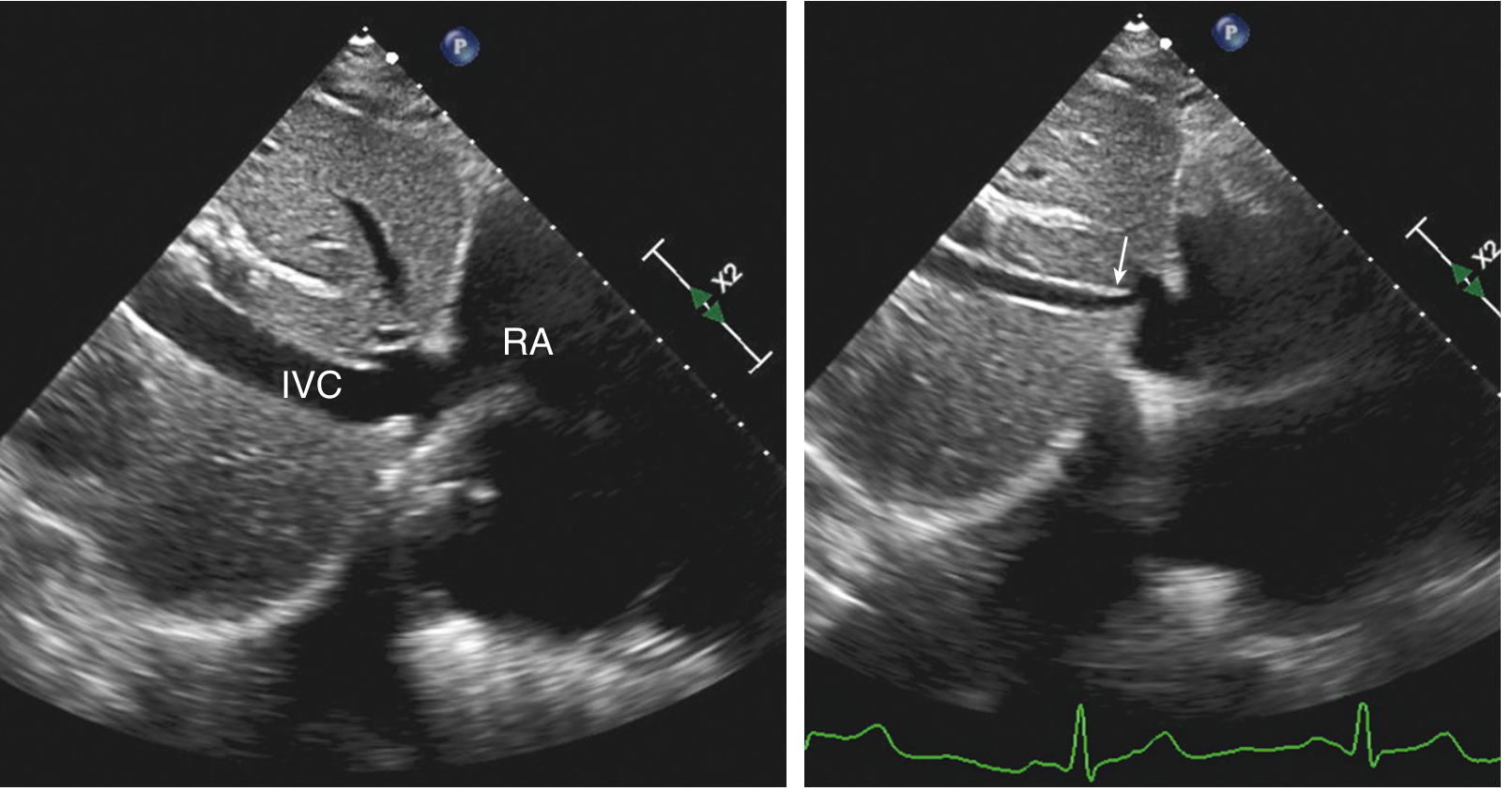
Left: IVC visible entering RA on expiration. Right: IVC collapses with inspiration (arrow), consistent with normal RA pressure.
4. How to Measure
Two methods:
a) 2D (B-mode): Measure the IVC diameter directly on the frozen image, in the anteroposterior dimension
b) M-mode (preferred for respiratory variation):
- Place the M-mode cursor perpendicular to the IVC, just distal to the hepatic vein
- This gives a time-motion trace showing IVC diameter over the respiratory cycle
- Read off the maximum diameter on expiration (D-max) and minimum diameter on inspiration (D-min)
5. The Collapsibility Index (cIVC)
For spontaneously breathing patients:
cIVC (%) = (D-max - D-min) / D-max × 100
Ask the patient to "sniff" (a quick, sharp nasal inspiration) to accentuate the response. - Miller's Anesthesia, 10th ed.
6. Interpreting the Results (ASE Guidelines)
The ASE table for estimating Right Atrial Pressure (RAP):
| IVC Diameter | Change with Sniff | RAP Estimate | ASE Value |
|---|---|---|---|
| Normal (≤ 2.1 cm) | Collapse > 50% | 0-5 mmHg | 3 mmHg |
| Normal (≤ 2.1 cm) | Collapse ≤ 50% | 5-10 mmHg | 8 mmHg |
| Dilated (≥ 2.1 cm) | Collapse > 50% | 10-15 mmHg | - |
| Dilated (≥ 2.1 cm) | Collapse ≤ 50% | 15-20 mmHg | 15 mmHg |
- Textbook of Clinical Echocardiography (ASE guidelines per Rudski et al., 2010)
An IVC diameter ≤ 2.1 cm and collapsibility > 50% with sniff indicates normal RA pressure of ~3 mmHg (0-5 mmHg). - Comprehensive Clinical Nephrology, 7th Ed.
7. Additional Clinical Notes
- An IVC diameter > 2.0 cm suggests elevated PCWP ≥ 17 mmHg (sensitivity 75%, specificity 83%, LR+ 4.4) - Symptom to Diagnosis, 4th Ed.
- In mechanically ventilated patients, IVC diameter changes are not reliable for RAP estimation. Instead, use the IVC distensibility index: (D-max inspiration - D-min expiration) / D-min × 100
- For intermediate RAP estimates, use secondary indices: tricuspid E/E', diastolic hepatic vein flow, RA size, and septal position to upgrade/downgrade the estimate
- Always confirm IVC identity by the hepatic vein junction - do not confuse with the aorta
Summary: Subcostal long-axis view → measure AP diameter just proximal to hepatic vein junction → apply M-mode for respiratory variation → use the collapsibility index with a sniff maneuver → interpret with the ASE table above.
What does IVC diameter tell me about volume status in shock?
Finding Sources
Finding Sources
Searching PubMed
"inferior vena cava" AND "fluid responsiveness" AND shock
Reading File
Reading File
Reading Article
PMID: 40187099
Reading File
Here is a thorough, evidence-based breakdown of what IVC diameter tells you in shock:
IVC Diameter and Volume Status in Shock
The Core Concept
IVC diameter is a surrogate for central venous pressure (CVP) and, by extension, right atrial pressure. The key distinction is between two types of measures:
- Static measure: IVC diameter at a single time point - tells you about preload, but is a poor predictor of fluid responsiveness alone
- Dynamic measure: Respiratory variation in IVC diameter (collapsibility/distensibility) - more useful for predicting whether a patient will respond to a fluid bolus
Volume responsiveness is defined as a 10-15% increase in stroke volume or cardiac output with a 250-500 mL crystalloid/colloid bolus. Only ~50% of hemodynamically unstable patients will actually respond to fluid. - Murray & Nadel's Textbook of Respiratory Medicine
Static IVC Diameter: What It Means
| IVC Diameter | Interpretation | CVP Estimate |
|---|---|---|
| Small (< 2.0 cm), collapses > 50% | Low preload - likely hypovolemic | Low / normal |
| Large (> 2.0 cm), collapses < 50% | High preload - elevated right-sided pressures | Elevated |
| IVC < 1 cm (in trauma/shock) | "Transient responder" - strongly fluid responsive | Very low |
In trauma and shock specifically: an IVC diameter < 1 cm at end-expiration is consistent with a transient responder and correlates strongly with fluid responsiveness. - Mulholland & Greenfield's Surgery, 7th Ed.
Dynamic IVC Measurements: Three Indices
All three use respiratory variation to predict fluid responsiveness. Each has a different denominator:
| Index | Formula | Best For |
|---|---|---|
| IVC Collapsibility Index (cIVC) | (IVC-max - IVC-min) / IVC-max × 100 | Spontaneously breathing patients |
| IVC Distensibility Index (dIVC) | (IVC-max - IVC-min) / IVC-min × 100 | Mechanically ventilated patients |
| IVC Diameter Variation (ΔIVC) | (IVC-max - IVC-min) / mean × 100 | Mechanically ventilated patients |
Key thresholds:
- cIVC ≥ 40% in spontaneously breathing patients suggests fluid responsiveness
- dIVC > 15% in mechanically ventilated patients (on large tidal volumes ~10 mL/kg) suggests fluid responsiveness
All three dynamic IVC measures have limited predictive utility with multiple different cutoff values reported - none should be used in isolation. - Murray & Nadel's Textbook of Respiratory Medicine
The 2025 Meta-Analysis: How Good Is IVC Actually?
A recent systematic review and meta-analysis (Yang et al., 2025, PMID 40187099) pooled 29 studies (1833 shock patients) and found:
| Metric | Value |
|---|---|
| Pooled Sensitivity | 0.82 (95% CI 0.75-0.87) |
| Pooled Specificity | 0.82 (95% CI 0.77-0.87) |
| Positive LR | 4.58 |
| Negative LR | 0.22 |
| AUC (SROC) | 0.89 (95% CI 0.86-0.91) |
Conclusion: IVC indices show moderate-to-good diagnostic accuracy for fluid responsiveness in shock, but significant heterogeneity exists across studies. The type of measurement, fluid used, and reference standard all contributed to variability.
Clinical Decision Algorithm by Scenario
Based on Murray & Nadel's Textbook of Respiratory Medicine:
1. Large IVC, no collapse - spontaneously breathing:
- Patient is unlikely to benefit from more fluid
- Rule out tamponade/obstructive shock (get cardiac views)
- Check for B-lines on lung ultrasound (pulmonary edema)
- Consider diuresis if heart failure is suspected
2. Small IVC, collapses - spontaneously breathing:
- Patient may benefit from a fluid bolus
- If in shock, administer fluid
- Beware deep breathing, which can exaggerate collapsibility
3. Large IVC, no collapse - mechanically ventilated:
- Unclear whether fluid will help or harm
- Do not use IVC alone to guide fluid decisions
- Combine with full echocardiographic assessment and clinical data
4. Small IVC, collapses - mechanically ventilated:
- Patient is likely volume responsive
- Administer a fluid bolus if in shock and respiratory status permits
Key Limitations to Know
- Mechanical ventilation confounds everything - IVC changes become an distensibility pattern (opposite direction), and tidal volume, PEEP, and patient effort all affect the reading
- Respiratory movement artifact - the IVC can move out of the scanning plane during inspiration, overestimating collapsibility
- IVC can be confused with aorta - always confirm by hepatic vein junction and RA entry
- Right heart failure, tamponade, raised intra-abdominal pressure - all cause a large non-collapsible IVC independent of volume status
- IVC examination is most reliable at extremes - a very small IVC or a very dilated, fixed IVC are the most actionable findings; intermediate values are unreliable without additional data
- High-flow nasal cannula, CPAP, BiPAP - all make IVC variation extremely difficult to interpret due to mixed respiratory efforts
Bottom line: IVC diameter gives useful directional information about preload and volume status in shock, but should never be used as the sole decision-making tool for fluid resuscitation. It is most reliable at the extremes, most accurate in purely spontaneously breathing or fully sedated/paralyzed ventilated patients, and should always be interpreted alongside clinical findings, cardiac function assessment, and lung ultrasound.
This is a shared conversation. Sign in to Orris to start your own chat.