Part B: Hearing 149. Functional Anatomy and Functions of the Ear 1202 150. Auditory Pathways 1208 151. Mechanism of Hearing 1211 152. Hearing Defects and Hearing Tests Add clinical corelations all the diagrams possible in an image form Add importance of everything and drugs and treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching PubMed
hearing loss treatment cochlear implant sensorineural
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Searching PubMed
sudden sensorineural hearing loss corticosteroid treatment
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Searching the Web
auditory pathway diagram cochlear nucleus inferior colliculus medial geniculate body primary auditory cortex
Loading Image
Reading File
Searching the Web
Rinne Weber test tuning fork hearing loss clinical interpretation diagram
Loading Image
Loading Image
Part B: Hearing - Complete Study Notes
149. Functional Anatomy and Functions of the Ear
Overview of Ear Divisions
The ear is divided into three functional regions: the external ear (sound collection), the middle ear (impedance matching and amplification), and the inner ear (transduction and encoding).
External Ear
Pinna (Auricle)
- Cartilaginous funnel that collects and localizes sound
- Directs sound waves into the external auditory meatus (EAM)
- Contains lobule (earlobe) - only fibrofatty tissue without cartilage
External Auditory Meatus (EAM)
- Length: ~2.5 cm, S-shaped canal
- Outer 1/3: cartilaginous (contains ceruminous glands, hair follicles)
- Inner 2/3: bony
- Resonant frequency: ~3400 Hz - explains why this frequency is most efficiently transmitted
Tympanic Membrane (TM)
- Area: ~85 mm²; effective vibrating area: ~55 mm²
- Three layers: outer (squamous epithelium), middle (fibrous), inner (mucosal)
- Pars tensa (large, tight) and pars flaccida (Shrapnell's membrane, small, loose)
- Attached to malleus via umbo at its center
- Acts as a pressure transducer converting sound waves to mechanical vibrations
Clinical Correlation - Otitis Media with Effusion ("Glue Ear"): Eustachian tube dysfunction blocks middle ear ventilation, producing negative pressure and fluid accumulation. Seen commonly in children. Treatment: grommets (ventilation tubes) for persistent cases >3 months with bilateral hearing loss >25 dB.
Middle Ear (Tympanic Cavity)
Contents: Ossicles (malleus, incus, stapes), two muscles (tensor tympani, stapedius), chorda tympani nerve, Eustachian tube opening
Ossicular Chain - Impedance Matching:
The middle ear solves a fundamental physics problem: sound waves in air must be transferred to fluid (perilymph) in the cochlea. Without impedance matching, 99.9% of energy would be reflected (30 dB loss).
The middle ear achieves ~30 dB amplification through:
- Hydraulic lever ratio - TM area (55 mm²) vs. stapes footplate (3.2 mm²) = 17:1 pressure gain
- Ossicular lever ratio - malleus arm longer than incus arm = 1.3:1
- Combined gain = 17 × 1.3 = ~22:1 (≈27 dB)
Two Middle Ear Muscles:
| Muscle | Nerve | Reflex Trigger | Function |
|---|---|---|---|
| Tensor tympani | V3 (trigeminal) | Touch to face, loud sound | Tenses TM, reduces low-freq transmission |
| Stapedius | VII (facial) | Loud sounds (>70 dB) | Acoustic reflex - protects cochlea |
Clinical Correlation - Acoustic Reflex: Absent stapedius reflex = facial nerve lesion (Bell's palsy) distal to stapedius branch. Reflex decay in 10 seconds = retrocochlear lesion (acoustic neuroma). Used in tympanometry testing.
Clinical Correlation - Hyperacusis in Bell's Palsy: When the facial nerve is paralyzed, stapedius cannot contract. Ordinary sounds seem painfully loud (hyperacusis), confirming the stapedius branch is above the lesion level.
Eustachian Tube:
- Connects middle ear to nasopharynx
- Normally closed; opens with swallowing/yawning
- Function: pressure equalization, drainage, protection
- Length in adults: 3.5 cm; in children: shorter and more horizontal (higher infection risk)
Clinical Correlation - Barotrauma: Rapid altitude change prevents Eustachian tube from equilibrating pressure. Results in TM rupture, haemotympanum, or perilymph fistula. Prevention: Valsalva maneuver. Treatment: decongestants (pseudoephedrine), analgesics, surgical repair for persistent fistula.
Inner Ear - Cochlea
Cochlear Cross-Sectional Anatomy
The cochlea is a fluid-filled bony spiral (2.5 turns) divided into three scalae:
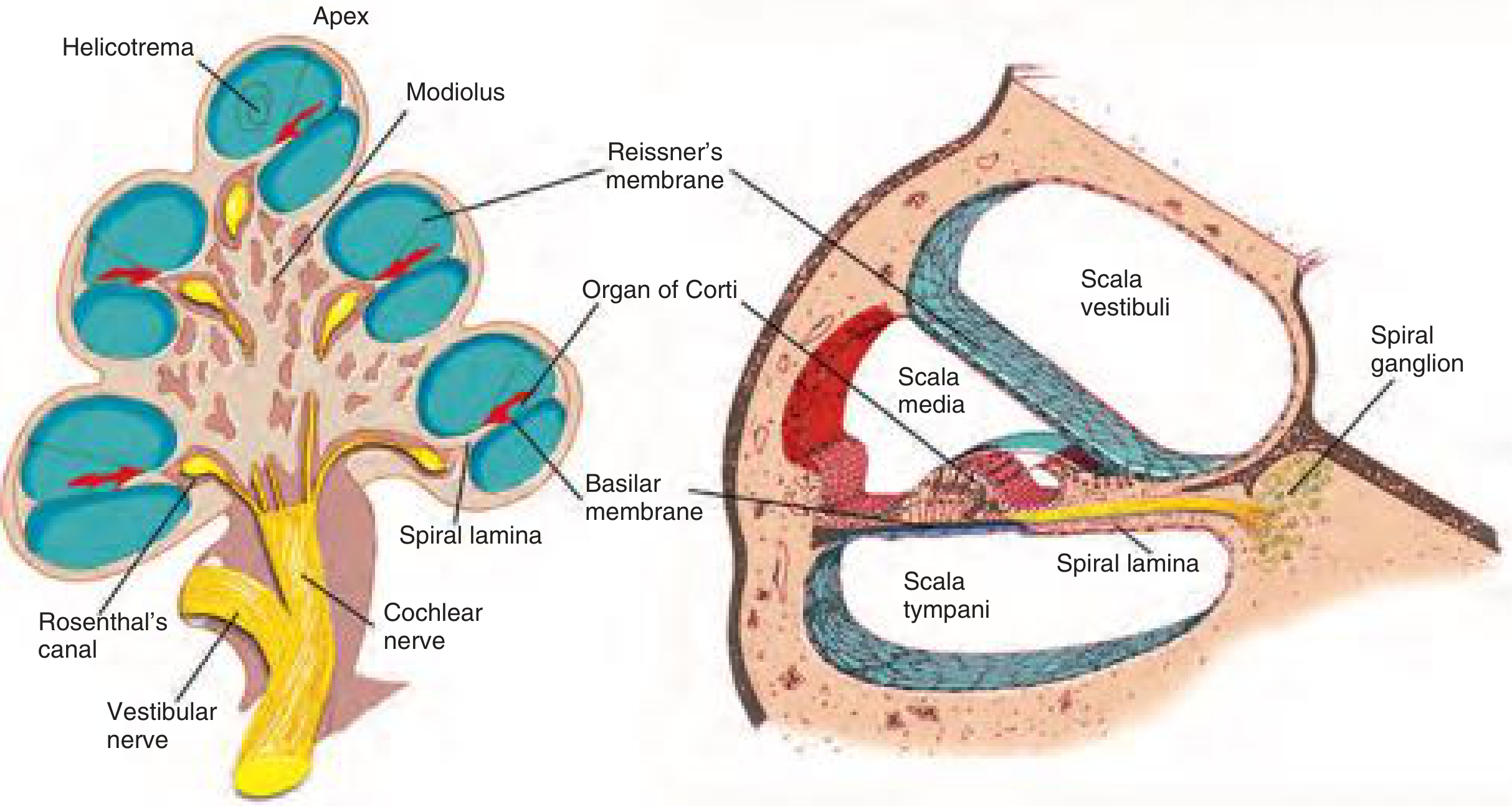
| Scala | Fluid | Composition | Clinical Note |
|---|---|---|---|
| Vestibuli | Perilymph | High Na+, Low K+ (like ECF) | Communicates with CSF via cochlear aqueduct - meningitis can enter here |
| Media (cochlear duct) | Endolymph | High K+, Low Na+ (like ICF) | Maintained by stria vascularis; disrupted in Meniere's disease |
| Tympani | Perilymph | High Na+, Low K+ | Terminates at round window |
The scalae vestibuli and tympani communicate at the apex through the helicotrema.
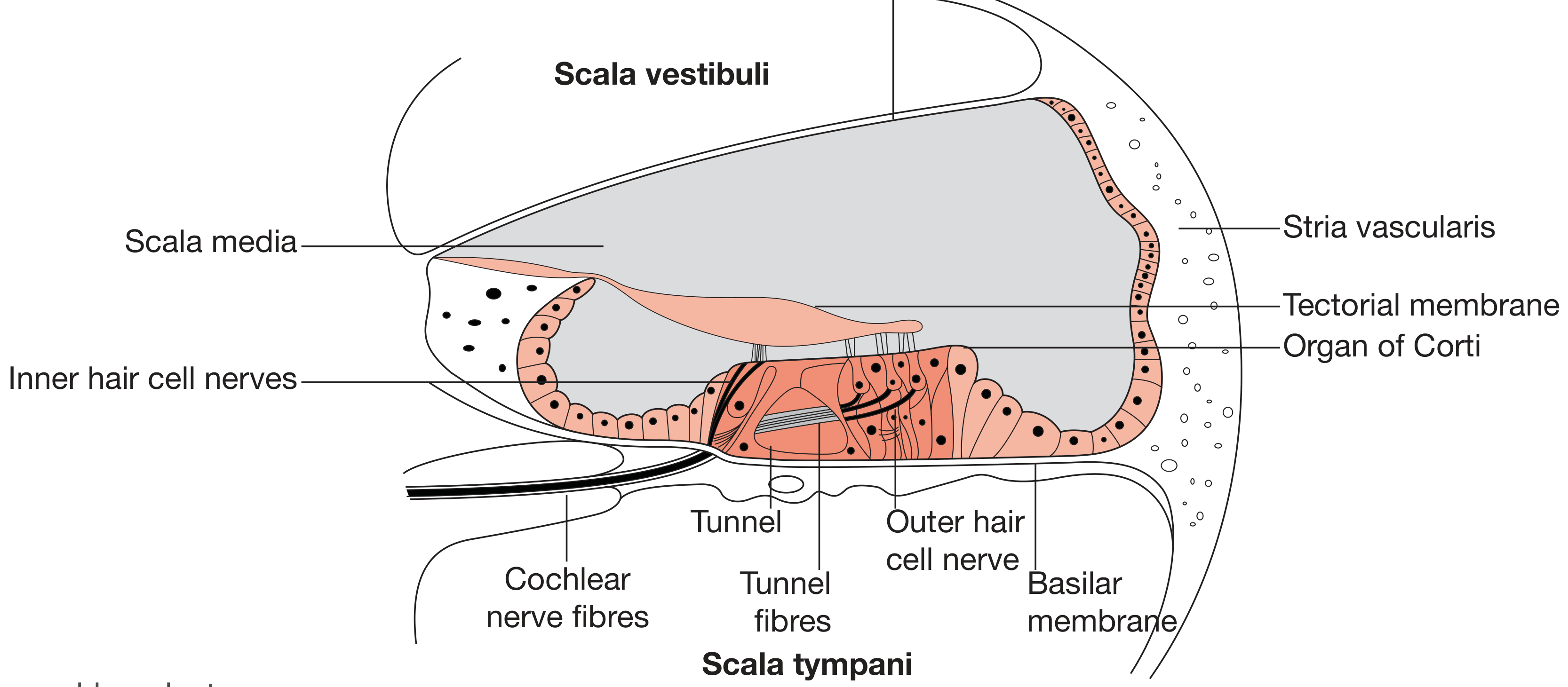
The Organ of Corti - The Receptor Organ
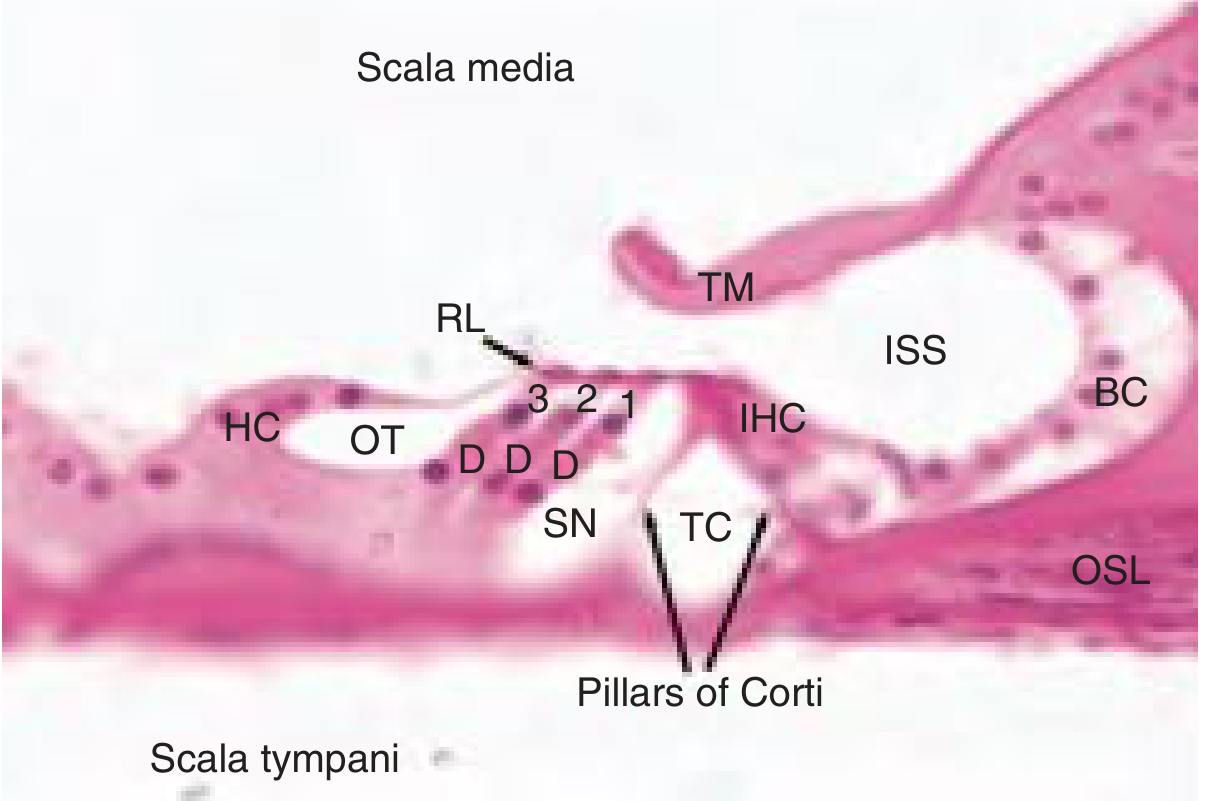
Hair Cells:
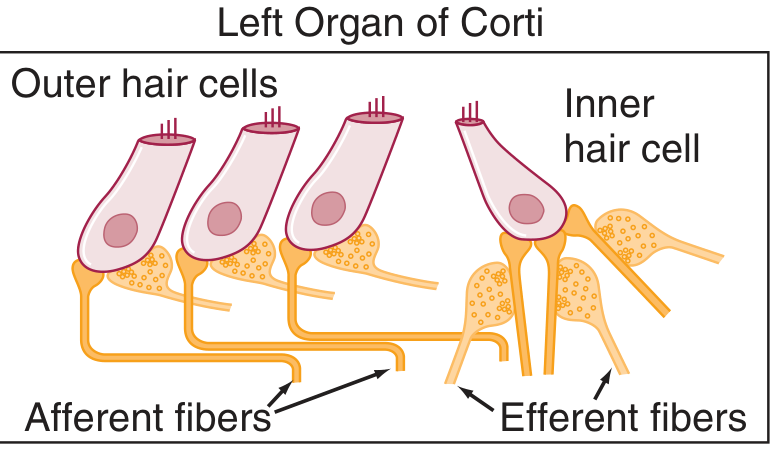
| Feature | Inner Hair Cells (IHC) | Outer Hair Cells (OHC) |
|---|---|---|
| Number | 3,500 (1 row) | 12,000 (3 rows) |
| Primary function | Afferent transducer | Active amplifier (electromotility) |
| Innervation | 95% of afferent fibers (Type I) | 5% of afferent fibers (Type II) |
| Efferent control | Sparse | Dense (olivocochlear bundle) |
| Clinical significance | Loss = sensorineural deafness | Loss of OHC = first sign of noise/drug-induced damage |
Clinical Correlation - Ototoxicity: Aminoglycoside antibiotics (gentamicin, tobramycin, neomycin) and loop diuretics (furosemide) preferentially destroy outer hair cells starting at the basal turn (high-frequency damage first). The basal OHC are most vulnerable because they have the lowest antioxidant capacity. This produces the classic high-frequency notch (4000 Hz) on audiogram. Cisplatin causes irreversible SNHL by generating reactive oxygen species. Monitoring: serial audiograms for at-risk patients.
150. Auditory Pathways
Peripheral Pathway
Spiral Ganglion → Cochlear Nerve → Brainstem
- ~30,000 auditory neurons with cell bodies in the spiral ganglion (located in Rosenthal's canal within the modiolus)
- Type I fibers (95%): Bipolar, myelinated, synapse 1:1 on a single IHC
- Type II fibers (5%): Smaller, synapse on multiple OHCs
- The cochlear nerve runs through the internal auditory meatus (IAM) with the vestibular nerve as CN VIII
Clinical Correlation - Acoustic Neuroma (Vestibular Schwannoma): Benign schwannoma arising from the vestibular portion of CN VIII within the IAM. Presents as unilateral SNHL + tinnitus + vertigo. ABR shows prolonged wave I-V latency. MRI with gadolinium is the gold standard. Treatment: microsurgical excision, stereotactic radiosurgery (Gamma Knife), or watchful waiting for small tumors.
Central Auditory Pathway
The ascending auditory pathway is the most complex sensory pathway in the CNS, with extensive bilateral representation at every relay station.
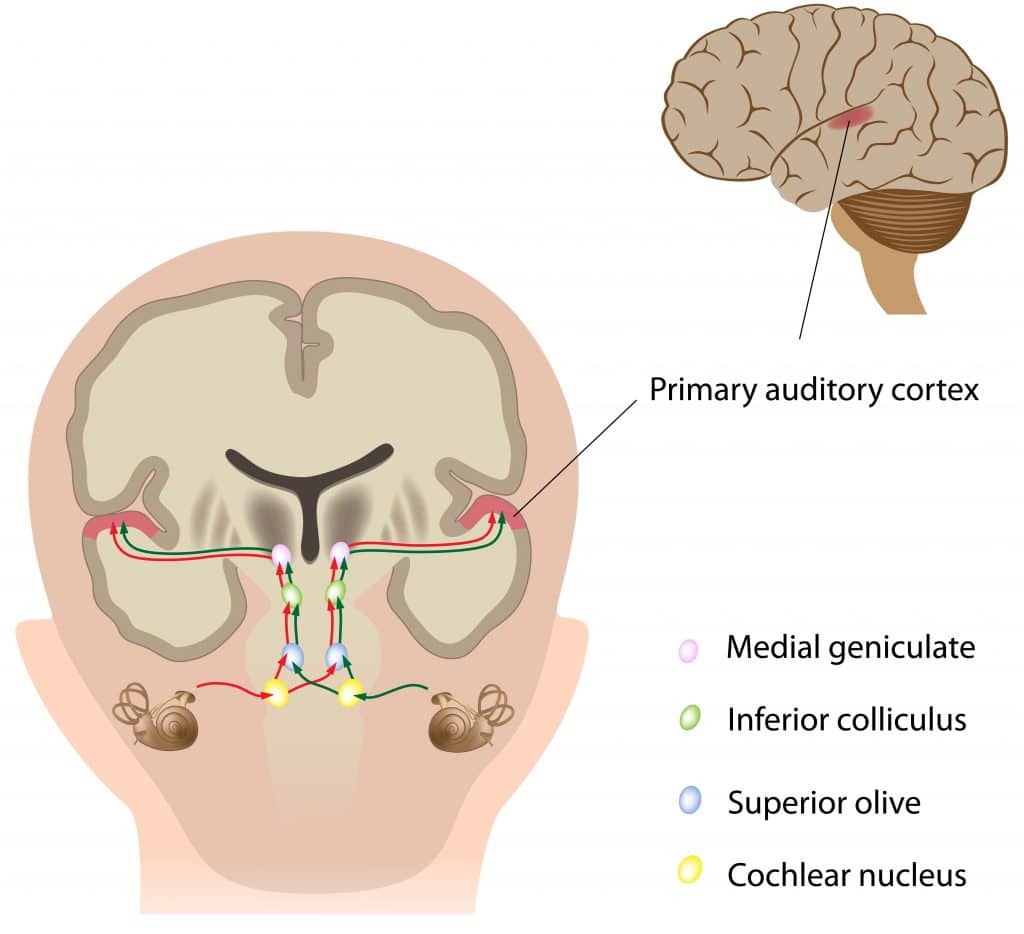
Step-by-Step Relay Stations
1. Cochlear Nuclei (Medulla - Ipsilateral)
- All cochlear nerve fibers synapse here first (obligatory relay)
- Three subdivisions: Dorsal cochlear nucleus, Anterior ventral, Posterior ventral
- Tonotopically organized
- Axons project via three acoustic striae:
- Ventral (trapezoid body) - most fibers, cross to contralateral side
- Intermediate - octopus cells
- Dorsal - contralateral inferior colliculus
Clinical Importance: Lesion here causes ipsilateral deafness. Unilateral cortical lesion does NOT cause complete deafness because of bilateral representation above the cochlear nuclei.
2. Superior Olivary Complex (SOC) (Caudal Pons)
- First binaural processing center
- Lateral superior olive (LSO): processes interaural intensity differences (IID)
- Medial superior olive (MSO): processes interaural time differences (ITD)
- Function: Sound localization in horizontal plane
- Gives rise to the olivocochlear bundle (efferent - descends to modulate OHC function)
Clinical Importance: Damage to the SOC impairs sound localization even with normal pure-tone thresholds.
3. Nucleus of Lateral Lemniscus (Pons/Midbrain Junction)
- Relay station for ascending fibers
4. Inferior Colliculus (IC) (Midbrain)
- ALL ascending auditory fibers synapse here
- Tonotopically organized
- Integrates binaural cues, spectral shape, and timing
- Connected to superior colliculus (coordinates audio-visual reflexes)
- Commissure of the inferior colliculus allows cross-hemisphere communication
Clinical Importance: Inferior colliculus lesion = binaural deficits, impaired localization. Also important in the "orienting reflex" to sounds.
5. Medial Geniculate Body (MGB) (Thalamus)
- Portal for all ascending auditory input to the cortex
- Three divisions: ventral (tonotopic, projects to primary cortex layers III/IV), dorsal, medial
- Medial division receives vestibular and somatosensory input too - role in "arousal" to sound
6. Primary Auditory Cortex (Heschl's Gyri)
- Brodmann area 41 (AI - primary) and 42 (AII - secondary)
- Located in the transverse gyri within the Sylvian fissure on the superior temporal gyrus
- Tonotopically organized: low frequencies anterolateral, high frequencies posteromedial
- Adjacent Wernicke's area (area 22) - receptive speech understanding
Clinical Correlation - Central Auditory Processing Disorder (CAPD): Normal audiogram but poor understanding in noise. Due to lesions/dysfunction in the central pathways. Common in elderly, post-stroke patients, and children with learning difficulties. Assessment: speech-in-noise tests, ABR, dichotic listening. Management: FM systems, auditory training programs.
Clinical Correlation - Wernicke's Aphasia: Lesion of Wernicke's area (dominant hemisphere, posterior STG) = fluent but incomprehensible speech with poor comprehension. The patient can hear but cannot decode linguistic meaning.
Mnemonic for Auditory Pathway
"Some Say Marry Lassie If Cute And Winning"
- Spiral ganglion → Superior olivary complex → Medulla (cochlear nuclei) → Lateral lemniscus → Inferior colliculus → Cortex (Auditory) → Wernicke's
Efferent (Descending) Auditory Pathway
The olivocochlear bundle (OCB) descends from the SOC to the cochlea:
- Medial OCB: projects to OHCs - suppresses OHC electromotility (reduces cochlear amplification, protects against noise)
- Lateral OCB: projects to afferent dendrites below IHCs
Clinical Importance: The OCB is the basis for otoacoustic emission suppression testing, used to detect brainstem lesions and auditory neuropathy. The presence of OAEs with absent ABR waves suggests auditory neuropathy spectrum disorder (ANSD).
151. Mechanism of Hearing
Steps in Sound Transduction
Step 1 - Sound Collection and Transmission (External Ear)
Sound waves travel through air → collected by pinna → funneled into EAM → strike the tympanic membrane.
Pinna's contribution: Directional cues for sound localization, particularly vertical plane (elevation) due to pinna ridges creating direction-dependent spectral filtering.
Step 2 - Middle Ear Impedance Matching
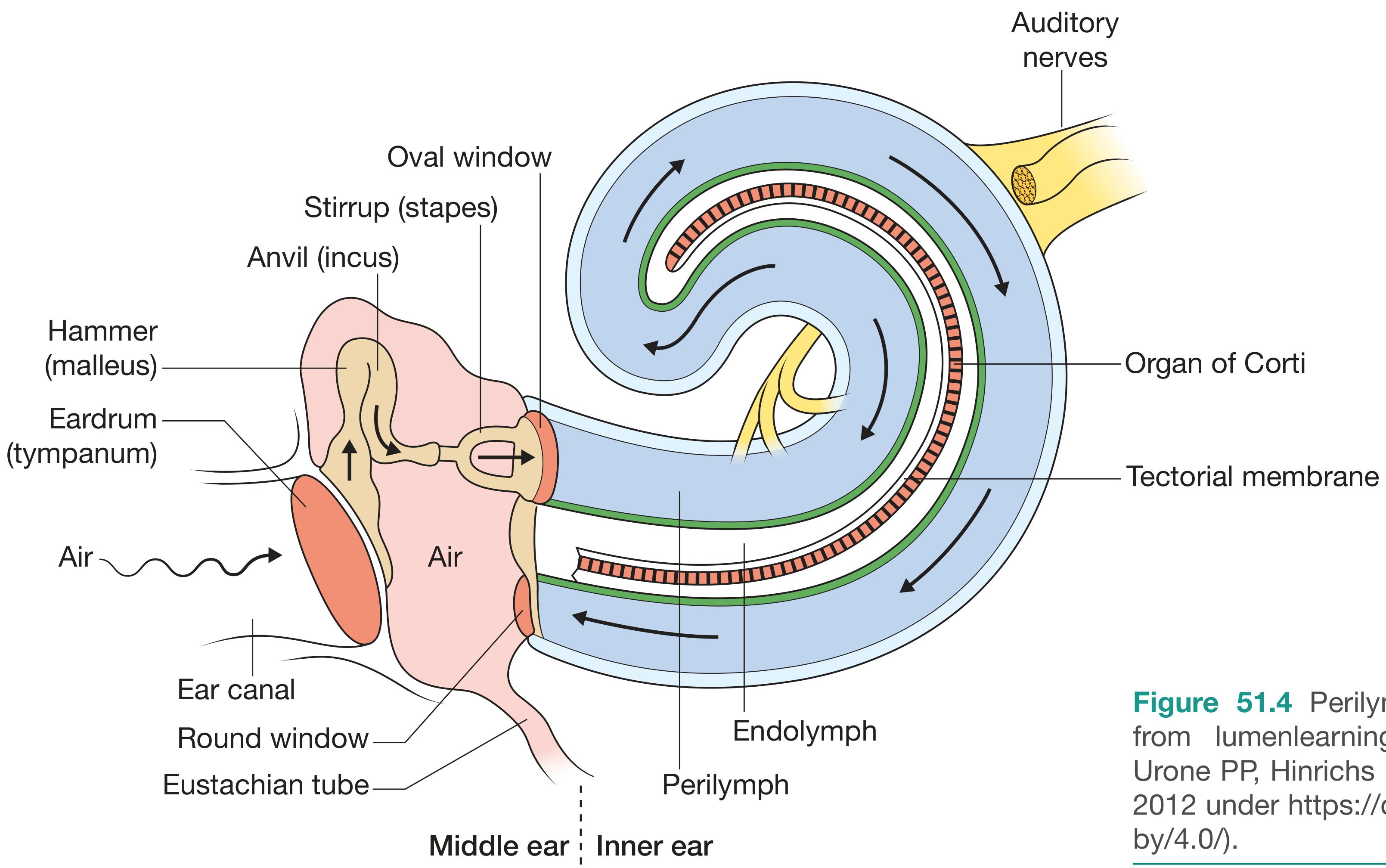
Sound waves → TM vibrates → malleus (handle attached to TM) → incus → stapes → stapes footplate vibrates in oval window → pressure wave in perilymph of scala vestibuli → travels up to helicotrema → down scala tympani → energy absorbed at round window (acts as a pressure-relief valve).
Why the round window matters clinically: Surgical obstruction of the round window (otosclerosis invading round window, adhesions) causes hearing loss independent of stapes mobility.
Step 3 - Basilar Membrane Traveling Wave (Von Bekesy's Theory)
The basilar membrane is NOT uniform:
- Base (near oval window): Narrow (0.04 mm), stiff - responds to HIGH frequencies
- Apex (helicotrema end): Wide (0.5 mm), floppy - responds to LOW frequencies
Sound creates a traveling wave that peaks at a specific location along the basilar membrane:
- 20,000 Hz → maximum displacement at the base
- 20 Hz → maximum displacement at the apex
- 1000 Hz → peaks ~20 mm from base
Why this matters clinically: This explains tonotopy - the spatial frequency map of the cochlea that is preserved throughout the entire auditory pathway. Noise-induced hearing loss first damages the 4000 Hz region because the 4 kHz region of the basilar membrane is adjacent to the region exposed to the maximum stapes-induced velocity.
Step 4 - Mechanoelectric Transduction (Hair Cell Transduction)
- Basilar membrane displacement causes a shearing motion between tectorial membrane and reticular lamina
- Stereocilia on OHCs (longest tips contact tectorial membrane) are deflected
- Tip links (fine filaments connecting tops of shorter stereocilia to sides of taller ones) are stretched
- Mechanically gated K+ ion channels open at stereocilia tips
- K+ flows INTO the hair cell (down its electrochemical gradient - from endolymph [+80 mV, high K+] into hair cell [−45 mV])
- Depolarization → Ca2+ entry at base → neurotransmitter release (glutamate)
- Excitatory postsynaptic potential in Type I afferent fibers → action potentials in cochlear nerve
The Endocochlear Potential (ECP): The scala media maintains a resting potential of +80 mV (relative to perilymph), maintained by the stria vascularis pumping K+ actively. The combined driving force for K+ entry is 80 mV (ECP) + ~45 mV (hair cell resting potential) = ~125 mV - an unusually large driving force that allows exquisite sensitivity. Conditions that damage the stria vascularis (Meniere's, endolymphatic hydrops) reduce the ECP and impair transduction.
Step 5 - Outer Hair Cell Amplification (Active Cochlear Mechanism)
OHCs contain the motor protein prestin in their lateral membrane. Prestin changes shape in response to membrane voltage changes - OHCs physically elongate and shorten (~0.5 μm at 100 kHz), amplifying basilar membrane motion by ~40 dB for soft sounds. This active amplification accounts for the extraordinary sensitivity of human hearing (~0 dB HL = 20 μPa SPL).
Clinical Importance - Otoacoustic Emissions (OAEs): OHC electromotility generates sounds back into the external ear canal that can be measured (OAEs). OAEs are absent when OHCs are damaged (noise, ototoxins) but present with retrocochlear lesions. Used in newborn hearing screening.
Frequency Coding
- Place coding (tonotopy): Basilar membrane location of maximum displacement encodes frequency - dominant for frequencies >200 Hz
- Temporal/phase-locking: Neurons fire in phase with the sound waveform - dominant for low frequencies (<4000 Hz)
- Combined: for frequencies 200-4000 Hz, both mechanisms contribute
Intensity Coding
- Rate coding: Higher stimulus intensity → higher firing rate in individual neurons
- Recruitment: More neurons (with higher thresholds) recruited at higher intensities
- Spread of excitation: Higher intensities excite a broader region of basilar membrane
Clinical Correlation - Recruitment: In cochlear (not retrocochlear) damage, there is an abnormally rapid growth of loudness. Patients say "don't shout!" even though they asked you to speak louder. This occurs because loss of OHC amplification removes the compressive nonlinearity of the cochlea. Recruitment helps localize the lesion to the cochlea (vs. nerve).
152. Hearing Defects and Hearing Tests
Classification of Hearing Loss
| Type | Location | Cause |
|---|---|---|
| Conductive | External/middle ear | Cerumen, otitis media, otosclerosis, TM perforation |
| Sensorineural (SNHL) | Cochlea/CN VIII/central | Noise, presbycusis, ototoxins, Meniere's, acoustic neuroma |
| Mixed | Both | Chronic otitis media with cochlear involvement |
| Central | Brainstem/cortex | Stroke, tumors, CAPD |
Tuning Fork Tests
Weber's Test (512 Hz)
- Place tuning fork on vertex of skull, glabella, or upper incisors
- Ask: "Does the sound sound the same in both ears, or louder in one?"
Rinne's Test (512 Hz)
- Compare Air Conduction (AC): fork tines near EAM
- vs. Bone Conduction (BC): fork base on mastoid

| Condition | Rinne's | Weber's | Why |
|---|---|---|---|
| Normal | AC > BC (positive) | Midline | Equal function bilaterally |
| Conductive HL (right) | BC > AC (negative - right ear) | Lateralizes to RIGHT (bad ear) | Masking effect of background noise eliminated; BC bypasses blockage |
| SNHL (right) | AC > BC (positive - false positive) | Lateralizes to LEFT (good ear) | Cochlea/nerve damaged, sound perceived better in functioning ear |
| Total deafness (right) | Negative (right) = Schwabach shortened | Lateralizes to LEFT |
Tuning Fork Frequencies: 256 Hz - feels vibration more than hears; 512 Hz - ideal for Rinne/Weber (best balance of tactile/auditory); 1024/2048 Hz - for very quiet environments.
Pure-Tone Audiometry
The audiogram is the cornerstone of hearing assessment. It plots hearing threshold (dB HL) vs. frequency (250-8000 Hz).
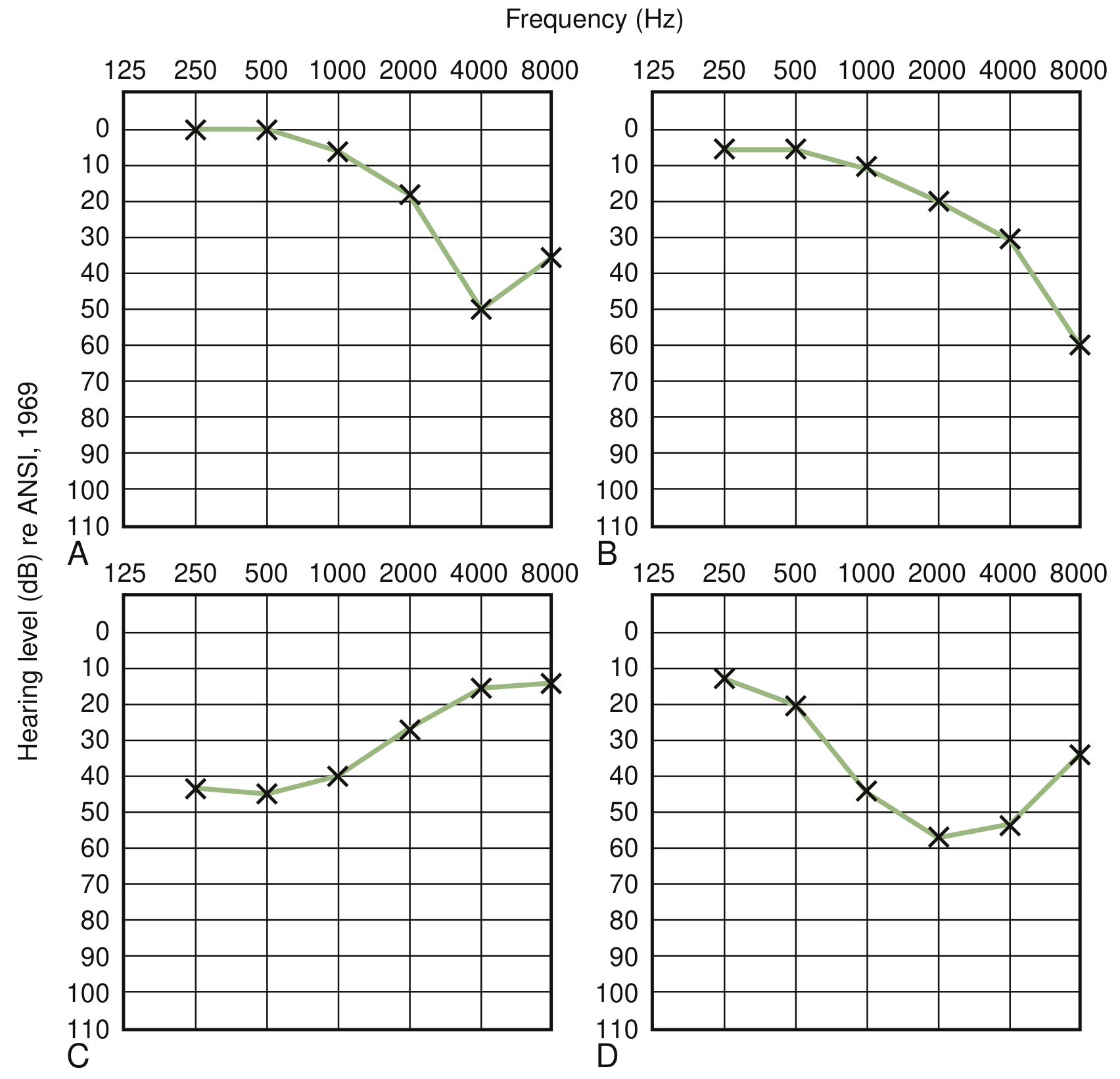
| Pattern | Diagnosis | Clinical Significance |
|---|---|---|
| High-freq slope (4 kHz notch) | Noise-induced HL, early presbycusis | First sign of NIHL; screen workers in noisy environments |
| Low-frequency trough (250-1000 Hz) | Meniere's disease (early) | Classic with fluctuating hearing + tinnitus + vertigo |
| Flat loss | Sudden SNHL, otosclerosis (conductive) | Sudden SNHL = medical emergency; treat within 2 weeks |
| Sloping high-frequency loss (presbycusis) | Age-related HL | Most common cause of HL worldwide |
| Cookie-bite (mid-frequency) | Hereditary HL | Genetic counseling indicated |
Audiogram Conventions:
- Air conduction: O (right, red), X (left, blue)
- Bone conduction: < (right), > (left)
- Air-bone gap >10 dB = conductive component
- Normal threshold: 0-25 dB HL
Hearing Loss Grading (WHO):
- Normal: ≤25 dB HL
- Mild: 26-40 dB (difficulty in noisy environments)
- Moderate: 41-60 dB (speech understanding impaired)
- Severe: 61-80 dB (shout not heard)
- Profound: >80 dB (candidate for cochlear implant)
Special Hearing Tests
Tympanometry
| Type | Description | Condition |
|---|---|---|
| Type A | Normal peak at 0 daPa | Normal middle ear |
| Type As | Low-amplitude peak | Stapes fixation (otosclerosis), tympanosclerosis |
| Type Ad | High-amplitude peak | Ossicular discontinuity, flaccid TM |
| Type B | Flat, no peak | Middle ear effusion, TM perforation |
| Type C | Peak at negative pressure | Eustachian tube dysfunction |
Clinical Correlation - Otosclerosis: Abnormal bone remodeling of the otic capsule, causing stapes footplate fixation. Audiogram: flat conductive HL with Carhart's notch (dip at 2 kHz on bone conduction - pathognomonic). Tympanogram: Type As. Treatment: Surgical stapedectomy/stapedotomy (prosthesis insertion). Medical: sodium fluoride (slows disease), hearing aids.
Otoacoustic Emissions (OAEs)
- Spontaneous OAEs (SOAEs): Generated without stimulus; present in ~70% of normal ears
- Transient evoked OAEs (TEOAEs): Evoked by click stimulus; used in newborn screening (NHS)
- Distortion product OAEs (DPOAEs): Two-tone stimulus; sensitive for OHC function at specific frequencies
- OAEs present = OHC intact (cochlear function adequate); OAEs absent = cochlear damage
Clinical Application: OAEs are absent in noise-induced hearing loss even before pure-tone thresholds shift, making them an early sensitive marker of cochlear damage. In auditory neuropathy spectrum disorder (ANSD): OAEs present (OHCs intact) but ABR absent (nerve/brainstem dysfunction).
Auditory Brainstem Response (ABR)
Five waves within 10 ms of a click stimulus:
- Wave I: Cochlear nerve (distal)
- Wave II: Cochlear nerve (proximal) or cochlear nucleus
- Wave III: Superior olivary complex
- Wave IV: Lateral lemniscus
- Wave V: Inferior colliculus
Clinical Application:
- Prolonged I-III interpeak latency = lesion between cochlear nerve and SOC (cerebellopontine angle tumor)
- Prolonged III-V interpeak latency = brainstem lesion
- Absent wave V with present wave I-III = midbrain lesion
- All waves absent = profound deafness
- ABR is used for: neonatal hearing screening, acoustic neuroma detection, intraoperative monitoring
Major Hearing Defects - Clinical Correlations, Drugs, and Treatment
1. Otosclerosis
Pathophysiology: Abnormal endochondral bone remodeling of the otic capsule, fixing the stapes footplate in the oval window.
Clinical: Young adults (2nd-3rd decade), females > males, bilateral in 70%, paracusis Willisii (hears better in noisy environments - paradoxical improvement in noise).
Audiogram: Conductive HL + Carhart's notch at 2000 Hz (bone conduction artefact).
Treatment:
- Surgery: Stapedectomy or stapedotomy (small fenestration + piston prosthesis) - curative
- Medical (slows progression): Sodium fluoride 20-60 mg/day (stabilizes abnormal bone remodeling)
- Hearing aid: For those refusing surgery or with cochlear involvement
- Estrogen accelerates progression - avoid OCP in suspected otosclerosis
2. Meniere's Disease (Endolymphatic Hydrops)
Pathophysiology: Excess endolymph distends the membranous labyrinth → rupture of Reissner's membrane → K+-rich endolymph floods perilymph space → vestibular/cochlear nerve depolarization block.
Classic Triad: Episodic vertigo (20 min - 12 hours) + fluctuating low-frequency SNHL + tinnitus + aural fullness (tetrad)
Audiogram: Low-frequency sensorineural HL; becomes flat/pan-cochlear in later stages.
Drugs and Treatment (stepped approach):
| Step | Treatment | Mechanism |
|---|---|---|
| 1st line | Low-sodium diet (<2g/day), diuretics | Reduce endolymph production |
| Diuretic | Hydrochlorothiazide + triamterene (Dyazide) | Reduces endolymph pressure |
| Vestibular suppressant (acute) | Prochlorperazine, cinnarizine, betahistine | Labyrinthine vasodilation (betahistine), antiemetic |
| Betahistine | 16-48 mg TDS | H1 agonist/H3 antagonist - improves cochlear microvascular flow |
| Intratympanic | Dexamethasone (hearing preservation) OR Gentamicin (ablative) | Chemical labyrinthectomy for intractable vertigo |
| Surgical | Endolymphatic sac decompression/shunting, labyrinthectomy, vestibular nerve section | Reserved for medical failure |
Betahistine is the only drug specifically licensed for Meniere's disease. Recent evidence (PMID: 38808803) confirms spontaneous recovery occurs in ~50% of untreated sudden SNHL cases, highlighting the importance of controlled studies for any Meniere's intervention.
3. Sudden Sensorineural Hearing Loss (SSNHL)
Definition: SNHL ≥30 dB across ≥3 consecutive frequencies developing over ≤72 hours.
Etiology: Idiopathic (85%), viral (mumps, herpes), vascular, autoimmune, acoustic neuroma.
Treatment:
- Oral corticosteroids (1st line): Prednisolone 1 mg/kg/day (max 60 mg) × 10-14 days, then taper
- Intratympanic steroids (ITG): Dexamethasone or methylprednisolone - for patients who cannot take systemic steroids or as salvage (2nd line)
- Hyperbaric oxygen (HBO): Adjunct to steroids - 2025 meta-analysis (PMID: 40405024) confirms HBO as effective adjunct to corticosteroids
- Salvage treatment: 2025 systematic review (PMID: 40734818) reviews salvage options including HBO, IT steroids, and combination approaches for refractory SSNHL
- Antiviral therapy (acyclovir): Only if herpes zoster oticus suspected
- Vasodilators (pentoxifylline, carbogen inhalation): Weak evidence; 2025 review (PMID: 40332573) on pentoxifylline in inner ear disease
Time sensitivity: Treatment within 2 weeks of onset gives best prognosis. Delayed treatment reduces chance of recovery.
4. Noise-Induced Hearing Loss (NIHL)
Pathophysiology: Acoustic trauma destroys OHCs in the 4 kHz basal turn region (most vulnerable due to resonance). Chronic exposure causes cumulative damage. Reactive oxygen species (ROS) are the primary mechanism of OHC death.
Audiogram: Notch at 4000 Hz (pathognomonic); recovers partially after acute exposure (temporary threshold shift, TTS), permanent after chronic exposure (PTS).
Treatment:
- Prevention: Ear protection (>85 dB noise levels at work - OSHA standard), monitoring programs
- Antioxidants (experimental): N-acetylcysteine (NAC), Mg2+ supplementation, D-methionine - reduce ROS-mediated OHC damage in animal models; human trials ongoing
- Established: Hearing aids for established NIHL; cochlear implant if profound
5. Presbycusis (Age-Related Hearing Loss)
Pathophysiology (Schuknecht classification):
- Sensory type: OHC loss at base (high frequency)
- Neural type: Spiral ganglion neuron loss (poor speech discrimination)
- Strial/metabolic type: Stria vascularis atrophy (flat HL)
- Mechanical/cochlear conductive type: Basilar membrane stiffening
Audiogram: Downward sloping bilateral symmetrical SNHL beginning at high frequencies.
Treatment:
- Hearing aids: First-line for mild-moderate HL; amplification helps but does not restore normal discrimination
- Cochlear implants: For severe-profound HL; meta-analysis (PMID: 38016438) confirms excellent outcomes even in auditory neuropathy
- Hearing loops, captioned telephones, assistive listening devices
- No established pharmacological treatment; research into BDNF, NT-3 to protect spiral ganglion neurons
6. Auditory Neuropathy Spectrum Disorder (ANSD)
Key feature: OAEs present (OHCs intact) but ABR absent or grossly abnormal. The problem is in IHC/synapse/cochlear nerve/brainstem.
Causes: Neonatal hyperbilirubinemia, hypoxia-ischaemia, genetic (OTOF gene mutation - otoferlin, essential for IHC ribbon synapse exocytosis), CMV.
Treatment:
- FM systems (bypass background noise)
- Cochlear implants work well because they bypass the damaged IHC/synapse and directly stimulate the nerve - PMID: 38016438 meta-analysis confirms cochlear implantation gives excellent outcomes in ANSD children
7. Congenital Hearing Loss
Genetics:
- 50-60% of congenital SNHL is genetic
- GJB2 (Connexin 26) mutation - most common cause of non-syndromic autosomal recessive SNHL (DFNB1); connexin channels in supporting cells maintain K+ recycling
- Pendred syndrome: SNHL + goitre (SLC26A4/pendrin mutation) - enlarged vestibular aqueduct; second most common syndromic cause
- Usher syndrome: SNHL + retinitis pigmentosa + vestibular dysfunction
- Waardenburg syndrome: SNHL + white forelock + heterochromia iridis (PAX3/MITF mutations); 2023 meta-analysis (PMID: 37847940) supports cochlear implantation
Newborn Hearing Screening:
- Transient OAEs (TEOAEs) or ABR in all neonates within 1 month
- Refer if fail; audiological diagnosis by 3 months
- Intervention by 6 months ("1-3-6 rule")
Treatment:
- Hearing aids for all degrees of HL from 3-4 months
- Cochlear implants: eligible from 12 months (or earlier in some guidelines) for bilateral profound SNHL
- Sign language and oral-aural habilitation
Drug-Induced Hearing Loss (Ototoxic Drugs)
| Drug Class | Examples | Effect | Reversibility |
|---|---|---|---|
| Aminoglycosides | Gentamicin, tobramycin, neomycin, streptomycin | SNHL (cochleotoxic) + vestibulotoxic | Irreversible |
| Platinum compounds | Cisplatin, carboplatin | Bilateral high-freq SNHL | Irreversible |
| Loop diuretics | Furosemide, ethacrynic acid | Transient or permanent SNHL | Often reversible |
| Salicylates | Aspirin (high dose >3g/day) | Reversible SNHL + tinnitus | Reversible on stopping |
| Quinine/chloroquine | Antimalarials | SNHL + tinnitus | Often reversible |
| NSAIDs | Ibuprofen, indomethacin | SNHL | Reversible |
Monitoring Protocol for Ototoxic Drugs: Baseline audiogram before starting cisplatin or aminoglycosides; repeat at each cycle and 3 months post-treatment. Monitor UHF (ultra-high frequencies 8-20 kHz) - earliest sign of damage. If significant threshold shift (>10 dB at 2+ frequencies), discuss with oncology team about dose modification or alternative agent.
Summary Table: Clinical Diagnosis at a Glance
| Feature | Otitis Media (Conductive) | Meniere's | Acoustic Neuroma | NIHL |
|---|---|---|---|---|
| Audiogram | Conductive HL, air-bone gap | Low-freq SNHL (early), flat (late) | Unilateral SNHL | 4 kHz notch |
| Tympanogram | Type B | Normal | Normal | Normal |
| OAEs | Normal or absent (B/L) | Absent (affected ear) | Absent (affected ear) | Absent (high freq) |
| ABR | Normal | Normal | Prolonged I-V latency | Normal |
| Rinne | Negative | Positive | Positive | Positive |
| Weber | Toward affected ear | Toward unaffected (later) | Toward unaffected | Toward better ear |
| MRI | Not needed | Not needed (unless atypical) | Gadolinium MRI - MANDATORY | Not needed |
Key Drugs Summary for Hearing Disorders
| Condition | Drug | Class | Dose/Route |
|---|---|---|---|
| SSNHL | Prednisolone | Corticosteroid | 60 mg/day PO × 14d |
| SSNHL | Dexamethasone | IT steroid | 4 mg/mL IT injection × 4 doses |
| Meniere's | Betahistine | Histamine analogue | 16 mg TDS PO |
| Meniere's | Hydrochlorothiazide | Thiazide diuretic | 25 mg OD PO |
| Meniere's | Gentamicin | IT aminoglycoside | 26-40 mg IT (ablative) |
| Meniere's (acute) | Prochlorperazine | Phenothiazine antiemetic | 12.5 mg IM acute |
| Ototoxicity prevention | N-acetylcysteine | Antioxidant | Investigational |
| Otosclerosis | Sodium fluoride | Bone remodeling inhibitor | 20-60 mg/day PO |
Recent Evidence (2023-2025)
- Natural history of untreated SSNHL (PMID: 38808803, 2024) - ~50% spontaneous recovery; underlines why controlled studies are needed
- Hyperbaric oxygen + steroids for SSNHL (PMID: 40405024, 2025) - Systematic review/meta-analysis confirms HBO is an effective adjunct to corticosteroids
- Salvage treatment for refractory SSNHL (PMID: 40734818, 2025) - Comprehensive review of IT steroids, HBO, and combination approaches with practical recommendations
- Pentoxifylline in inner ear disease (PMID: 40332573, 2025) - Reviews vasodilator use; limited evidence
- Cochlear implantation in ANSD children (PMID: 38016438, 2024) - Meta-analysis confirms excellent speech outcomes post-CI
Sources: Cummings Otolaryngology Head and Neck Surgery; Bailey & Love's Short Practice of Surgery 28th ed; Bradley & Daroff's Neurology in Clinical Practice; Neuroscience: Exploring the Brain 5th ed; Scott-Brown's Otorhinolaryngology; PubMed 2023-2025 systematic reviews.
Give the full response
This is a shared conversation. Sign in to Orris to start your own chat.