Shock
Reading File
Finding Sources
Searching PubMed
shock classification pathophysiology management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, well-sourced information from multiple major textbooks. I can now compose a thorough, well-organized answer on Shock.
Shock
Definition
Shock is a state of circulatory failure causing inadequate tissue perfusion and cellular hypoxia. At the cellular level, oxygen delivery falls below metabolic demand, forcing cells to switch to anaerobic glycolysis and generating lactic acid. At the outset the injury is reversible; prolonged shock leads to irreversible cell death and multi-organ failure. - Robbins & Cotran Pathologic Basis of Disease, p. 134
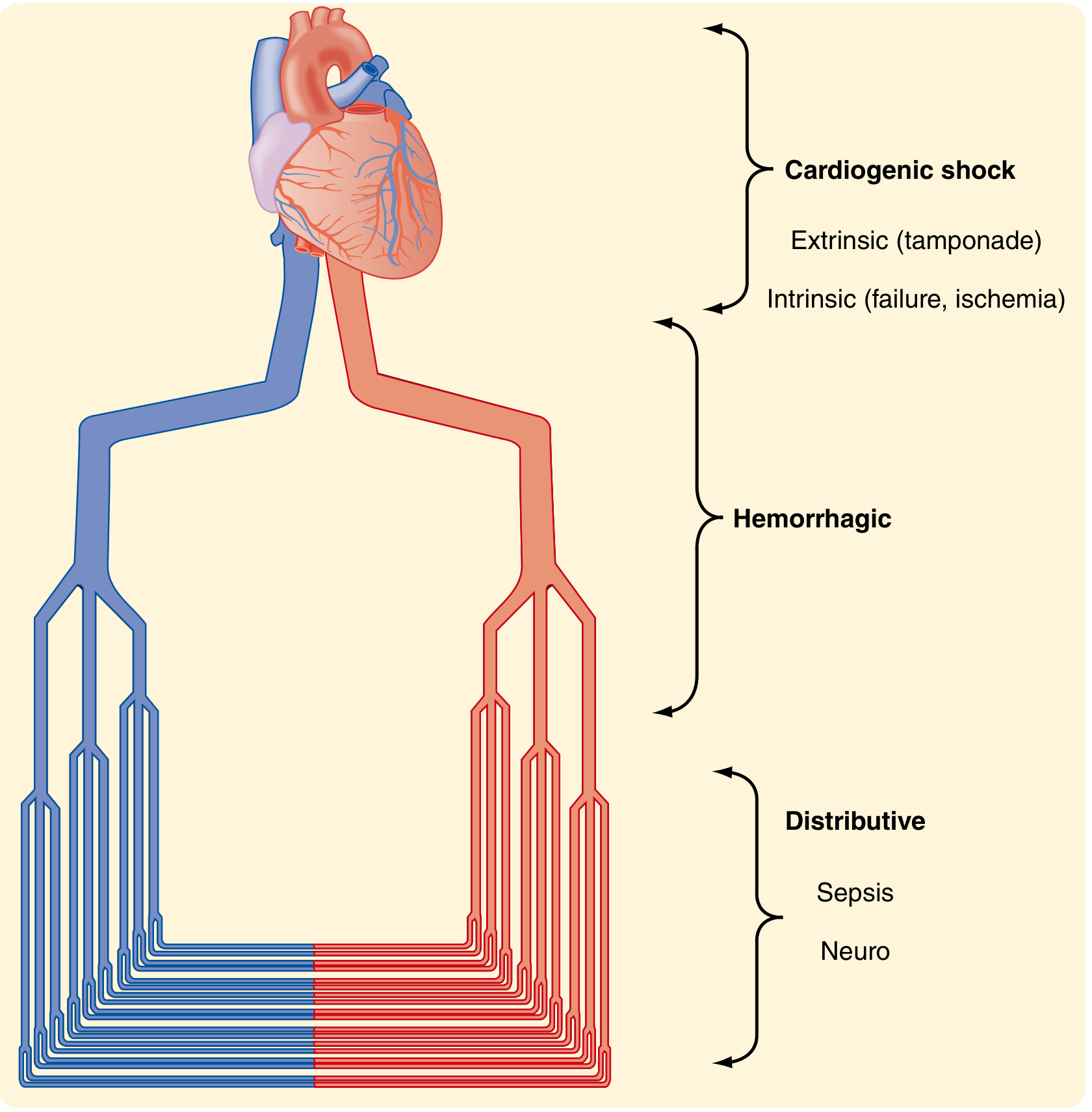
Classification
The modern classification divides shock into four broad categories. The Sabiston diagram illustrates the anatomical basis:
1. Hypovolemic Shock
- Cause: Loss of blood volume (hemorrhage, burns, vomiting, diarrhea, excessive sweating)
- Hemodynamics: Low CO, high SVR, low CVP, low mixed venous O2 saturation
- Mechanism: Reduced venous return → reduced preload → reduced cardiac output → hypoperfusion
2. Cardiogenic Shock
- Cause: Pump failure - intrinsic (MI, arrhythmia, cardiomyopathy) or extrinsic/obstructive (cardiac tamponade, pulmonary embolism, tension pneumothorax)
- Hemodynamics: Low CO, high SVR, HIGH CVP (backed-up venous pressure), low mixed venous O2 saturation
- Note: Obstructive shock (tamponade, PE) is sometimes listed as its own fourth category
3. Distributive Shock
Inadequate organ perfusion accompanied by vasodilatation, low SVR, and paradoxically high cardiac output (warm shock). Includes:
- Septic shock - dysregulated host response to infection; bacterial endotoxin/gram-positive toxins activate TLRs → TNF, IL-1, IL-6, IL-12 cascade → endothelial activation, vasodilation, microvascular injury, DIC
- Anaphylactic shock - IgE-mediated mast cell degranulation → massive histamine release → vasodilatation
- Neurogenic shock - high spinal cord injury → loss of sympathetic outflow → vasodilatation and bradycardia
4. Endocrine Shock
- Adrenal insufficiency (Addison's, relative insufficiency in sepsis), hypothyroidism (low CO from reduced inotropy + bradycardia), thyrotoxicosis (high-output failure). May combine features of hypovolemic and distributive shock. - Bailey and Love's Short Practice of Surgery, p. 34
Summary hemodynamic table (from Bailey & Love):
| Parameter | Hypovolemic | Cardiogenic | Obstructive | Distributive |
|---|---|---|---|---|
| Cardiac Output | Low | Low | Low | High |
| SVR | High | High | High | Low |
| CVP/Venous Pressure | Low | High | High | Low |
| Mixed Venous O2 Sat | Low | Low | Low | High |
| Base Deficit | High | High | High | High |
Pathophysiology & Stages (Guyton)
Stage 1 - Nonprogressive (Compensated) Shock
The body activates negative feedback mechanisms to restore perfusion:
- Baroreceptor reflexes - immediate sympathetic activation within 30 seconds
- CNS ischemic response - extreme sympathetic discharge when BP < 50 mmHg
- Renin-Angiotensin-Aldosterone - peripheral vasoconstriction + sodium/water retention (10-60 min)
- ADH (vasopressin) - arteriole and venous constriction + water retention
- Adrenal catecholamines - epinephrine/norepinephrine → tachycardia, vasoconstriction
- Reverse stress-relaxation - blood vessels contract around diminished volume
- Fluid absorption - interstitial → intravascular shift; thirst; renal conservation (1-48 hours)
Stage 2 - Progressive Shock (Positive Feedback / Vicious Cycles)
When shock becomes severe enough, protective mechanisms fail and positive feedback loops drive deterioration:
- Cardiac depression: Coronary flow falls → myocardial ischemia → further reduced CO
- Vasomotor failure: Brainstem ischemia → vasomotor center fails → vasodilation → catastrophic BP drop (after 10-15 min of severe ischemia)
- Microvascular sludging: Lactic and carbonic acid accumulation → RBC agglutination → capillary obstruction
- Endothelial injury: Activated neutrophils + oxidants + cytokines → capillary leak
- Coagulopathy: Endothelial activation + consumptive coagulopathy → DIC
Stage 3 - Irreversible Shock
- Extensive tissue necrosis, lysosomal enzyme release, depletion of cellular ATP and creatine phosphate
- ATP degrades to adenosine → diffuses out of cells → converted to uric acid → cannot be resynthesized (only ~2%/hour regeneration)
- At this point, even restoration of cardiac output to normal cannot prevent death - Guyton & Hall Medical Physiology, p. 302-304
ATLS Hemorrhagic Shock Classification
| Class | Blood Loss | HR | BP | Pulse Pressure | Mental Status |
|---|---|---|---|---|---|
| I | < 15% (< 750 mL) | < 100 | Normal | Normal | Anxious |
| II | 15-30% (750-1500 mL) | 100-120 | Normal/Low | Narrowed | Anxious |
| III | 30-40% (1500-2000 mL) | 120-140 | Decreased | Narrowed | Confused |
| IV | > 40% (> 2000 mL) | > 140 | Very low | Narrowed | Lethargic/obtunded |
Important caveat: ATLS classes were not rigorously validated. Children compensate longer (only tachycardia until a tipping point); the elderly decompensate earlier. Heart rate alone is neither sensitive nor specific for hemorrhagic shock. - Sabiston Textbook of Surgery, p. 568
Pathogenesis of Septic Shock (in detail)
The two key pathways are:
- Pro-inflammatory cascade: Microbial PAMPs (LPS, peptidoglycan, M-protein) bind TLRs → NF-κB activation → TNF, IL-1, IL-12, IFN-γ, HMGB1, prostaglandins, PAF → endothelial adhesion molecule upregulation, capillary leak, DIC
- Counter-regulatory immunosuppression: Th1 → Th2 cytokine shift, IL-10, soluble TNF receptor, lymphocyte apoptosis → septic patients oscillate between hyperinflammatory and immunosuppressed states
Septic shock is most commonly triggered by:
- Gram-positive bacteria (most frequent)
- Gram-negative bacteria
- Fungi
- Viral infections (e.g. SARS-CoV-2)
Mortality remains approximately 40% despite improvements in care. - Robbins & Cotran Pathologic Basis of Disease, p. 135
Cellular & Metabolic Consequences
- Anaerobic metabolism → lactic acidosis → base deficit
- The Lethal Triad (in hemorrhagic/traumatic shock): Acidosis + Hypothermia + Coagulopathy - these three feed each other in a destructive cycle
- Hypothermia impairs clotting enzyme function; acidosis worsens coagulopathy; coagulopathy perpetuates hemorrhage
- Large-volume crystalloid resuscitation contributes to the triad (dilutional coagulopathy + heat loss from cold fluids)
- ATP depletion → cell membrane pump failure → cellular swelling (oncotic cell death)
- DIC: Widespread microvascular thrombi form in septic/traumatic shock → consumptive coagulopathy → paradoxical bleeding - Sabiston Textbook of Surgery, p. 571
Organ Effects
| Organ | Effect |
|---|---|
| Kidney | Acute tubular necrosis (ischemia to proximal tubules/loop of Henle) → acute kidney injury |
| Liver | Centrilobular necrosis (zone 3, most oxygen-dependent) |
| Lungs | ARDS - diffuse alveolar damage from neutrophil activation + capillary leak |
| GI tract | Mucosal barrier failure → bacterial translocation → worsening sepsis |
| Brain | Encephalopathy; preserved until late due to autoregulation |
| Adrenals | Cortical lipid depletion (hemorrhage in meningococcemia = Waterhouse-Friderichsen) |
| Heart | Subendocardial necrosis (most vulnerable; zone farthest from coronary supply) |
Management Principles
General
- Identify and treat the cause - source control is the foundation
- Restore tissue perfusion: target normalization of serum lactate, base deficit, pH, and urine output
- Blood pressure alone is insufficient as an endpoint - occult hypoperfusion can exist with normal vitals
Fluid Resuscitation
- Hemorrhagic shock: Limit crystalloids (avoid resuscitation injury); after 1-2 L crystalloid, switch to blood products. Damage control resuscitation: balanced ratio of PRBCs:FFP:platelets (~1:1:1)
- Septic shock (Surviving Sepsis Campaign): 30 mL/kg IV crystalloid within 3 hours; then reassess with dynamic markers
- Neurogenic shock: Small volumes isotonic crystalloid; vasopressors early (phenylephrine or norepinephrine) to restore vascular tone
- Avoid routine pulmonary artery catheter (no longer recommended)
Vasopressors
- Norepinephrine - first line for septic shock and most distributive shock
- Vasopressin - adjunct in septic shock; add when norepinephrine dose is escalating
- Dopamine - alternative to norepinephrine in selected patients (bradycardic)
- Phenylephrine - pure alpha agonist; useful in neurogenic shock
Specific Treatments
- Cardiogenic shock: Revascularization (PCI for MI), inotropes (dobutamine), mechanical circulatory support (IABP, Impella)
- Septic shock: Antibiotics within 1 hour of recognition, source control, corticosteroids if vasopressor-refractory
- Anaphylactic shock: Epinephrine IM (first line), antihistamines, corticosteroids
- Cardiac tamponade: Pericardiocentesis
- Tension pneumothorax: Needle decompression → chest tube
Acidosis
- Treat the underlying cause of acidosis, not the pH value alone
- Sodium bicarbonate: no proven benefit for metabolic acidosis; rapid infusion may worsen intracellular acidosis (CO2 diffusion); use is controversial and generally reserved for extreme scenarios
- THAM (tromethamine): Alternative buffer; sodium-free, effective during hypothermia, pKa 7.8 - Sabiston Textbook of Surgery, p. 571-572
Key Summary Points
- Shock = inadequate tissue perfusion → cellular hypoxia → lactic acidosis
- Four types: Hypovolemic, Cardiogenic/Obstructive, Distributive (septic/anaphylactic/neurogenic), Endocrine
- Three stages: Compensated (reversible with treatment), Progressive (positive feedback loops), Irreversible (cellular death, ATP depletion)
- The lethal triad in traumatic/hemorrhagic shock: acidosis + hypothermia + coagulopathy
- Septic shock mortality ~40%; first-line treatment = antibiotics + source control + norepinephrine
- Resuscitation endpoints: lactate clearance, base deficit normalization, urine output > 0.5 mL/kg/hr
Sources: Robbins & Cotran Pathologic Basis of Disease; Sabiston Textbook of Surgery; Bailey and Love's Short Practice of Surgery; Guyton & Hall Medical Physiology; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.