Sepsis
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"sepsis"[MeSH Terms] AND "management"[MeSH Terms]
Searching the Web
Surviving Sepsis Campaign guidelines 2024 update
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the material needed for a comprehensive overview. Let me compile the full answer.
Sepsis — Comprehensive Overview
Definition (Sepsis-3, 2016)
Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection.
Septic shock is a subset of sepsis in which underlying circulatory and cellular metabolic abnormalities are profound enough to substantially increase mortality. It is identified clinically by:
- Vasopressor requirement to maintain MAP ≥ 65 mmHg, AND
- Serum lactate > 2 mmol/L despite adequate fluid resuscitation
Mortality in septic shock is approximately 40%.
The older SIRS-based definition (≥2 of: fever/hypothermia, tachycardia, tachypnea, leukocytosis/leukopenia) has been replaced by the SOFA score — sepsis is now diagnosed as a SOFA score increase ≥ 2 from baseline in the setting of suspected or confirmed infection. — Washington Manual of Medical Therapeutics, p. 295; Tintinalli's Emergency Medicine, p. 1039
SIRS vs. Sepsis vs. Infection
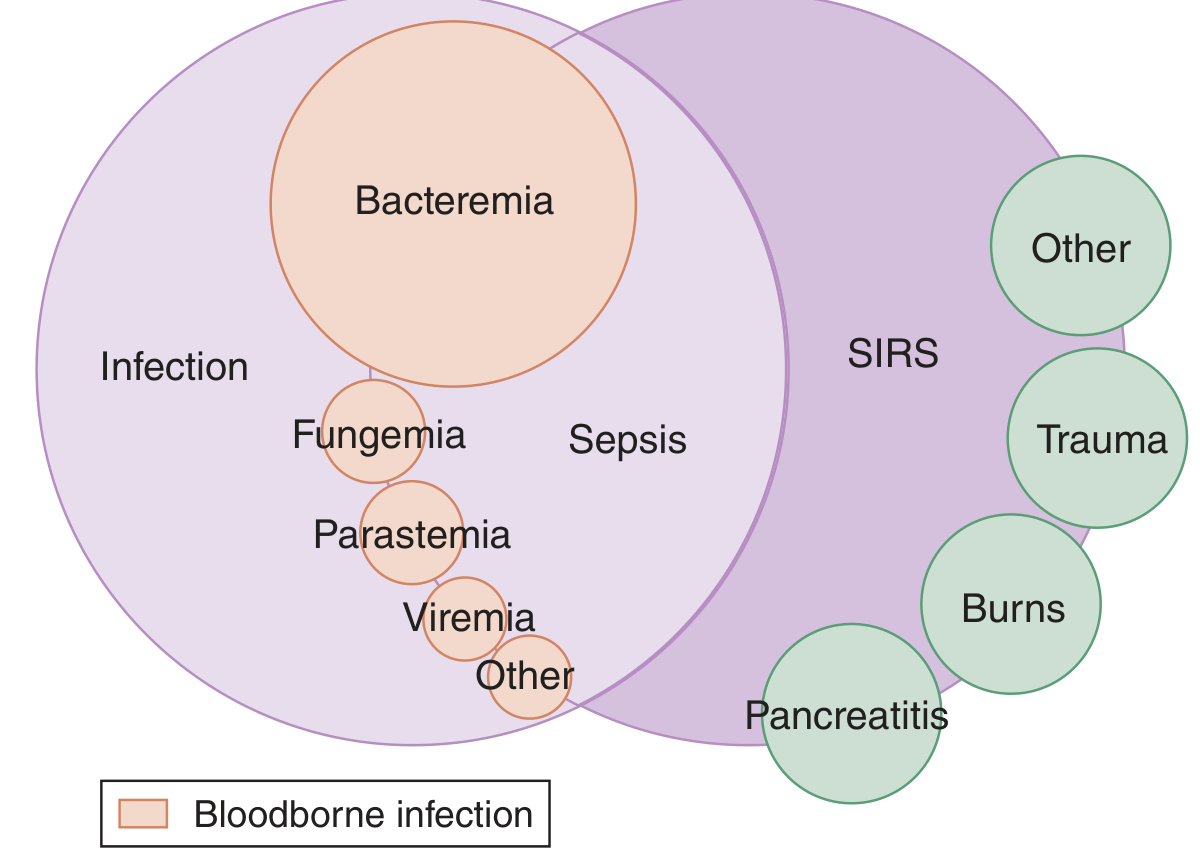
SIRS can occur without infection (trauma, burns, pancreatitis); sepsis sits at the intersection of SIRS and infection. — Tintinalli's Emergency Medicine
Pathophysiology
The cascade begins when microbial products (PAMPs — pathogen-associated molecular patterns) or injured-cell products (DAMPs) bind Toll-like receptors (TLRs) on innate immune cells (neutrophils, monocytes), triggering NF-κB activation and release of:
- Pro-inflammatory cytokines: TNF, IL-1, IL-12, IL-18, IFN-γ, HMGB1
- Reactive oxygen species, prostaglandins, platelet-activating factor (PAF)
- Complement cascade: C3a (mast cell activation), C5a (chemotactic), C3b (opsonin)
- Nitric oxide (NO): causes vascular smooth muscle relaxation → hypotension
Two critical downstream events drive organ failure:
-
Hyperinflammation → immunosuppression: The initial cytokine storm triggers counter-regulatory mechanisms (shift from Th1 to Th2, IL-10, lymphocyte apoptosis), leaving patients susceptible to secondary nosocomial infections.
-
Procoagulant–anticoagulant imbalance: Endothelial activation increases tissue factor expression, depletes protein C and thrombomodulin, and elevates PAI-1, causing microvascular thrombosis and DIC, impairing tissue perfusion and perpetuating organ injury.
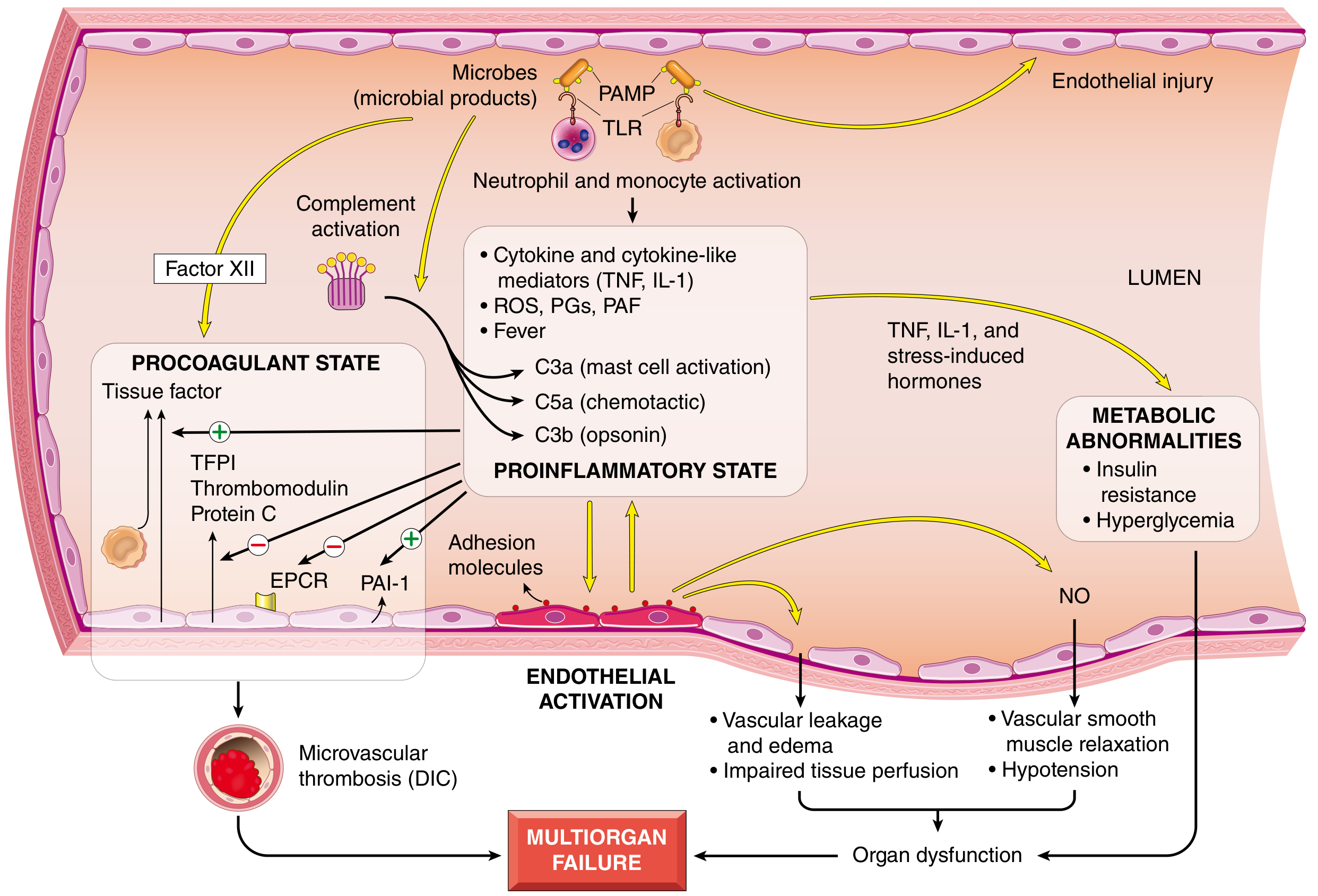
Microbial products activate TLRs → proinflammatory state → endothelial activation → vascular leakage, DIC, organ dysfunction. — Robbins Pathologic Basis of Disease, p. 135
Organ Complications
| Organ | Manifestation |
|---|---|
| Lung | ARDS — PaO₂/FiO₂ <300; bilateral infiltrates; mortality 27–45% by severity |
| Kidney | Acute kidney injury — elevated creatinine, reduced GFR |
| Coagulation | DIC — thrombocytopenia, elevated PT/aPTT, ↓ fibrinogen, ↑ fibrin split products |
| Liver | Elevated bilirubin/LFTs |
| Heart | Septic cardiomyopathy — reversible systolic/diastolic dysfunction; may present as "cold shock" |
| Metabolism | Lactic acidosis, hyperglycemia/insulin resistance |
Diagnosis
Screening Tools
- qSOFA (bedside, no labs): ≥2 of — altered mentation, RR ≥22/min, SBP ≤100 mmHg → warrants concern
- SOFA score: formal organ-dysfunction scoring across respiratory, coagulation, liver, cardiovascular, CNS, renal domains — increase ≥2 confirms sepsis
Key Laboratory Tests
| Test | Significance |
|---|---|
| Lactate | >2 mmol/L = tissue hypoperfusion; >4 mmol/L = ~28% mortality; serial clearance is prognostic |
| CBC | Leukocytosis/leukopenia, thrombocytopenia, bandemia ≥5–10% |
| Blood cultures | Before antibiotics if possible; only 30–40% of clinical sepsis has positive cultures |
| Procalcitonin / CRP | Elevated; procalcitonin best used for serial measurement and antibiotic stewardship |
| BMP/CMP | Anion-gap metabolic acidosis, elevated creatinine, low bicarbonate, electrolyte disturbances |
| Coagulation | PT, aPTT, fibrinogen, D-dimer — screen for DIC |
| Urinalysis + culture | Essential, especially in elderly patients |
| ABG | Classify acid-base; assess oxygenation |
Rosen's Emergency Medicine, p. 2757; Tintinalli's Emergency Medicine, p. 1039
Management (Surviving Sepsis Campaign Principles)
1. Early Fluid Resuscitation
- ≥ 30 mL/kg IBW IV crystalloid within the first hour
- Prefer balanced crystalloids (lactated Ringer's) over normal saline — associated with lower rates of renal dysfunction
- Reassess volume responsiveness continuously to avoid overload; adjust if concomitant heart failure
2. Vasopressors
- Start if MAP remains <65 mmHg despite adequate fluids
- Norepinephrine — first-line agent (fewer adverse events than dopamine)
- Vasopressin — second-line adjunct
3. Antimicrobials
- Broad-spectrum IV antibiotics immediately — delays increase mortality
- Obtain blood cultures before antibiotics if this can be done quickly, but do not significantly delay treatment
- De-escalate based on culture results and sensitivity data
- Procalcitonin can guide antibiotic duration/stewardship
4. Source Control
- Identify and control the anatomical source of infection as soon as possible (e.g., drain abscess, debride necrotizing tissue)
5. Additional Measures
- Glucose control: target <180 mg/dL
- Lung-protective ventilation if ARDS develops: low tidal volume (6 mL/kg IBW), PEEP optimization
- Corticosteroids (hydrocortisone 200 mg/day): considered in refractory septic shock
- Transfusion: current guidelines do not recommend transfusion to a specific hemoglobin threshold (targeting Hgb 7–9 g/dL is generally acceptable)
- Avoid colloids (albumin) — no significant benefit over crystalloids in most trials
6. Monitoring & Goals
- Lactate clearance (repeat measurement) — downtrending lactate mirrors clinical improvement
- Serial SOFA scores for organ trajectory
- CVP and dynamic parameters (pulse pressure variation, passive leg raise response) to guide ongoing resuscitation
Washington Manual of Medical Therapeutics, pp. 295–296; Rosen's Emergency Medicine, pp. 2757–2758; Surviving Sepsis Campaign (SSC) 2021 Guidelines
Summary Table
| Feature | Sepsis | Septic Shock |
|---|---|---|
| Definition | Infection + SOFA ≥2 | Sepsis + vasopressor-dependent + lactate >2 mmol/L |
| Hypotension | May be absent | Persistent despite fluids |
| Lactate | May be elevated | >2 mmol/L required for definition |
| Mortality | Significant | ~40% |
The SSC 2021 Guidelines remain the current international standard, with updated emphasis on post-ICU care and long-term sepsis sequelae. New SSC guideline updates have been released in 2024 by ESICM/SCCM with further refinements based on recent trial evidence.
This is a shared conversation. Sign in to Orris to start your own chat.