Give 10 marks answer of shoulder joint
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
I now have comprehensive content from authoritative textbooks. Let me compile the full 10-marks answer.
The Shoulder Joint (Glenohumeral Joint)
1. Introduction
The shoulder joint (glenohumeral joint) is the articulation between the head of the humerus and the glenoid cavity of the scapula. It is a ball-and-socket synovial joint and is the most mobile yet least stable joint in the human body, owing to the shallow glenoid fossa relative to the large humeral head. This design sacrifices bony stability in favour of an enormous range of motion.
2. Articulating Surfaces
| Structure | Description |
|---|---|
| Head of humerus | Large, rounded; covered with hyaline cartilage |
| Glenoid cavity of scapula | Shallow, pear-shaped fossa; faces anterolaterally |
| Glenoid labrum | Fibrocartilaginous ring that deepens the cavity marginally |
The glenoid cavity covers only about one-third of the humeral head at any given position, making the labrum and soft-tissue stabilisers essential.
3. Capsule and Ligaments
Articular Capsule: A fibrous sleeve that is loose and redundant (especially inferiorly - the axillary recess) to permit wide movement. It attaches to the glenoid labrum medially and the anatomic neck of the humerus laterally.
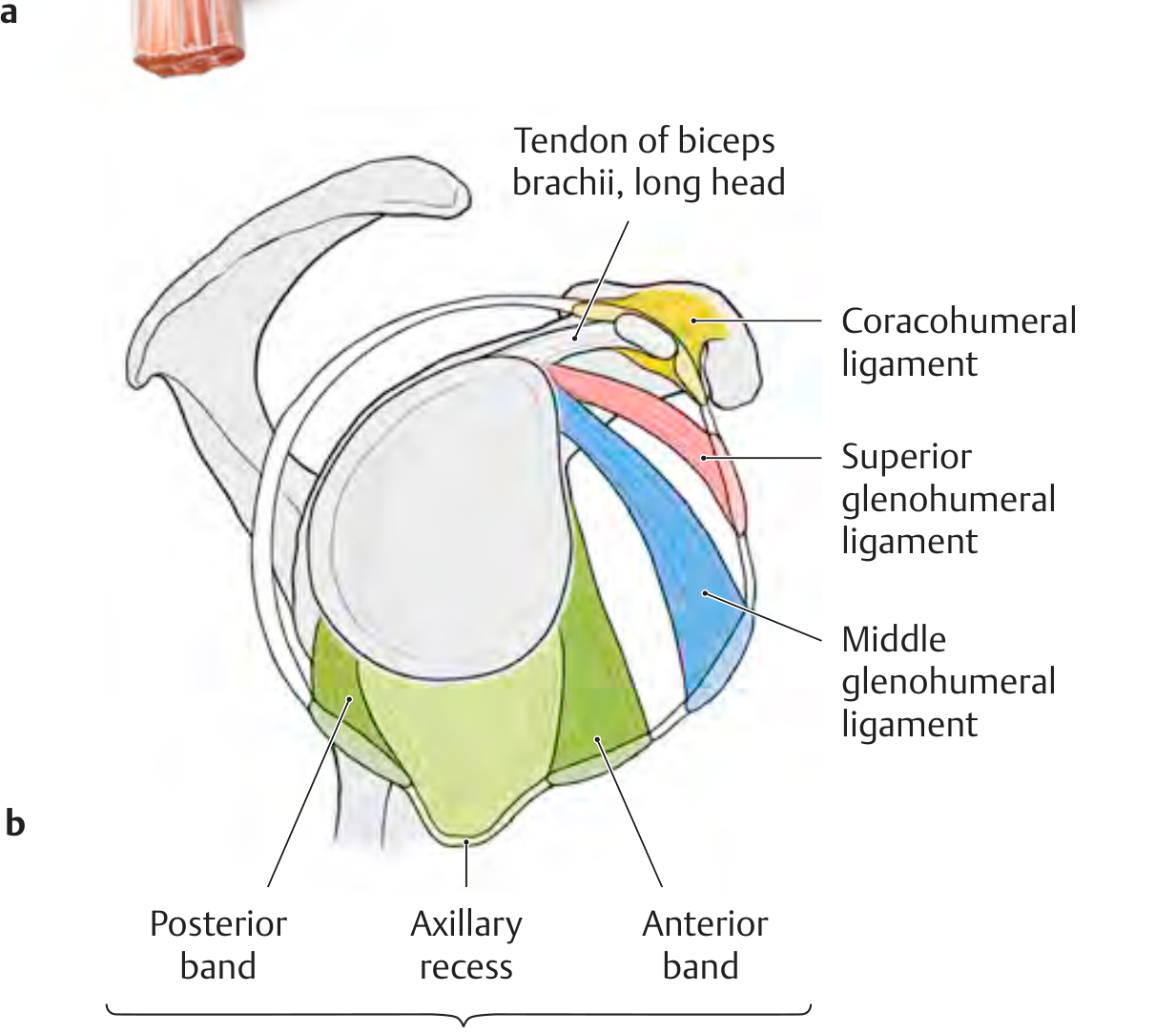
Glenohumeral Ligaments (thickenings of the anterior capsule - best seen arthroscopically):
- Superior glenohumeral ligament (SGHL): Runs from the upper glenoid margin to the intertubercular groove and lesser tubercle. Forms the "roof" of the biceps pulley (rotator interval).
- Middle glenohumeral ligament (MGHL): Passes at almost a right angle to the subscapularis tendon from the upper glenoid margin to the anatomic neck of the humerus.
- Inferior glenohumeral ligament (IGHL): The most important stabiliser. Has three parts: anterior band, posterior band, and axillary recess (which hangs as a "hammock" during abduction). Extends from the inferior glenoid margin to the surgical neck of the humerus. This is the primary restraint to anterior-inferior dislocation.
Coracohumeral Ligament: A strong, broad band arising from the base of the coracoid process; its two bands attach to the greater and lesser tubercles of the humerus. Together with the SGHL it forms the rotator interval structure, stabilising the biceps tendon long head.
Transverse Humeral Ligament: A band stretching between the greater and lesser tubercles that holds the biceps long head tendon in the intertubercular groove.
4. Rotator Cuff (Dynamic Stabilisers)
The rotator cuff is formed by four muscles whose tendons blend with and reinforce the joint capsule:
| Muscle | Origin | Insertion | Action |
|---|---|---|---|
| Supraspinatus | Supraspinous fossa | Greater tubercle (superior facet) | Initiates abduction (first 0-10°); keeps humeral head centred in glenoid |
| Infraspinatus | Infraspinous fossa | Greater tubercle (middle facet) | External rotation |
| Teres minor | Lateral border of scapula | Greater tubercle (inferior facet) | External rotation |
| Subscapularis | Subscapular fossa (anterior scapula) | Lesser tubercle | Internal rotation (sole anterior muscle) |
The rotator cuff muscles contribute 30-50% of abduction power and 90% of external rotation power. Their tendons send expansions to the joint capsule, actively pressing the humeral head into the glenoid during movement (concavity-compression mechanism).
5. Bursae
Several bursae reduce friction around the shoulder:
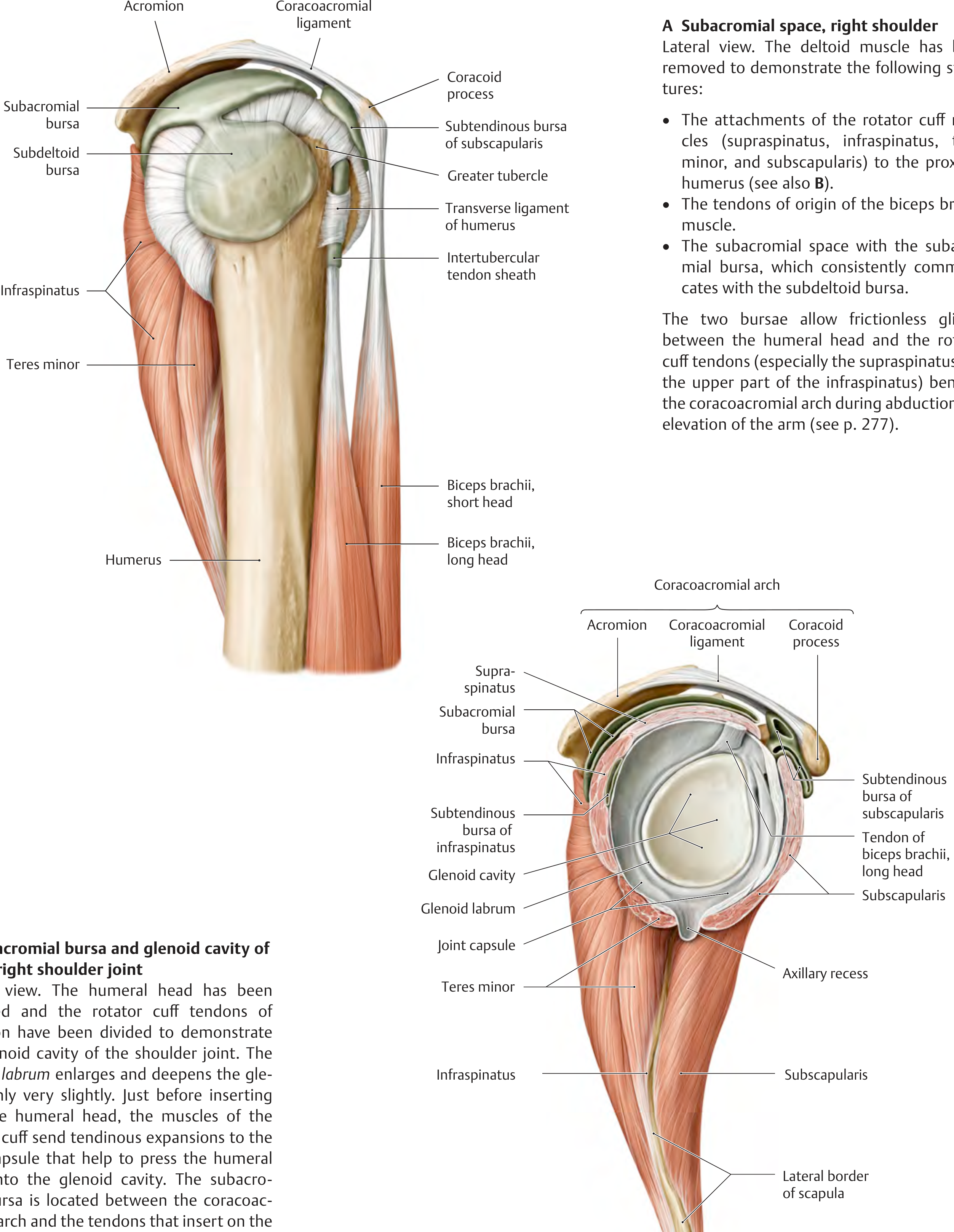
- Subacromial bursa - lies between the coracoacromial arch and the rotator cuff tendons; allows frictionless gliding during arm elevation.
- Subdeltoid bursa - between the deltoid and greater tubercle; communicates consistently with the subacromial bursa.
- Subtendinous bursa of subscapularis - between the subscapularis tendon and the scapular neck; may communicate with the joint cavity.
- Subtendinous bursa of infraspinatus - posterior aspect.
After a complete rotator cuff rupture, the subacromial and subdeltoid bursae communicate directly with the articular cavity.
6. Intracapsular Structures
- Tendon of the long head of biceps brachii: Arises from the supraglenoid tubercle inside the capsule, passes over the humeral head, and exits through the intertubercular groove where it is held by the transverse humeral ligament. It is a weak stabiliser that assists the rotator cuff.
- Synovial membrane: Lines the capsule and extends as a sleeve around the biceps long head tendon, forming the intertubercular tendon sheath.
7. Movements and Muscles Responsible
| Movement | Range | Prime Movers |
|---|---|---|
| Flexion | 0-180° | Anterior deltoid, pectoralis major (clavicular), coracobrachialis, biceps brachii |
| Extension | 0-60° | Posterior deltoid, latissimus dorsi, teres major |
| Abduction | 0-180° | Supraspinatus (first 10-15°), middle deltoid; requires scapular rotation for full elevation |
| Adduction | - | Pectoralis major, latissimus dorsi, teres major |
| Internal rotation | 0-70° | Subscapularis, pectoralis major, latissimus dorsi, teres major, anterior deltoid |
| External rotation | 0-90° | Infraspinatus, teres minor, posterior deltoid |
| Circumduction | Full arc | Combination of above |
Scapulohumeral rhythm: For every 3° of shoulder abduction, 2° occur at the glenohumeral joint and 1° at the scapulothoracic joint. This rhythm allows the full 180° arc of elevation.
8. Nerve Supply
The shoulder joint receives innervation from multiple sources (Hilton's law):
- Axillary nerve (C5, C6) - primary supply
- Suprascapular nerve (C5, C6) - posterosuperior capsule
- Musculocutaneous nerve (C5, C6, C7) - anterior capsule (small branch)
- Lateral pectoral nerve - anterosuperior capsule
The axillary nerve winds around the surgical neck of the humerus (quadrangular space) and is at risk in shoulder dislocations and proximal humeral fractures.
9. Blood Supply
- Anterior and posterior circumflex humeral arteries (branches of the axillary artery) - form an anastomotic ring around the surgical neck
- Suprascapular artery (from thyrocervical trunk)
- Subscapular artery (from axillary artery)
10. Clinical Correlations
a) Shoulder dislocation (most common joint dislocation):
- Anterior dislocation (95% of cases) - the humeral head is forced anteroinferiorly, typically rupturing the anterior capsule/IGHL. The Hill-Sachs lesion (posterosuperior humeral head impaction defect) and Bankart lesion (avulsion of the anteroinferior glenoid labrum) are characteristic MRI findings.
- Axillary nerve injury is the most common neurological complication.
b) Rotator cuff tear:
- Supraspinatus tendon is involved in 95% of complete tears.
- Subacromial impingement is caused by mechanical contact between the calcified or degenerate supraspinatus tendon and the coracoacromial arch during abduction.
c) Frozen shoulder (adhesive capsulitis):
- Progressive contracture and fibrosis of the joint capsule, especially the IGHL and rotator interval, leading to loss of external rotation and abduction.
d) Bankart lesion:
- Detachment of the glenoid labrum and IGHL from the anteroinferior glenoid rim, causing recurrent anterior instability. Treated by arthroscopic Bankart repair with anchor sutures.
Sources: General Anatomy and Musculoskeletal System - THIEME Atlas of Anatomy, pp. 285-290; Tintinalli's Emergency Medicine, pp. 2151-2165; ROSEN's Emergency Medicine, p. 670.
Knee joint
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent - I have comprehensive textbook content and three high-quality anatomical diagrams. Now I can write the full 10-marks answer.
The Knee Joint
1. Introduction
The knee joint is the largest and most complex synovial joint in the human body. It consists of two distinct articulations enclosed in a single joint cavity:
- Tibiofemoral joint - between the femoral condyles and tibial condyles; weight-bearing.
- Patellofemoral joint - between the patella and the patellar (trochlear) surface of the femur; redirects the pull of the quadriceps anteriorly over the knee.
Structurally it is primarily a modified hinge joint (ginglymus), but it allows small degrees of rotation when flexed.
2. Articulating Surfaces
| Bone | Articular Surface |
|---|---|
| Femur | Two condyles (medial and lateral) + patellar (trochlear) surface anteriorly |
| Tibia | Superior surfaces of medial and lateral condyles (tibial plateau) |
| Patella | Posterior articular surface (divided by a vertical ridge) |
All surfaces are covered by hyaline cartilage. The surfaces of the femoral condyles that articulate in flexion are curved and rounded; those in full extension are broad and flat - a key feature of the locking mechanism.
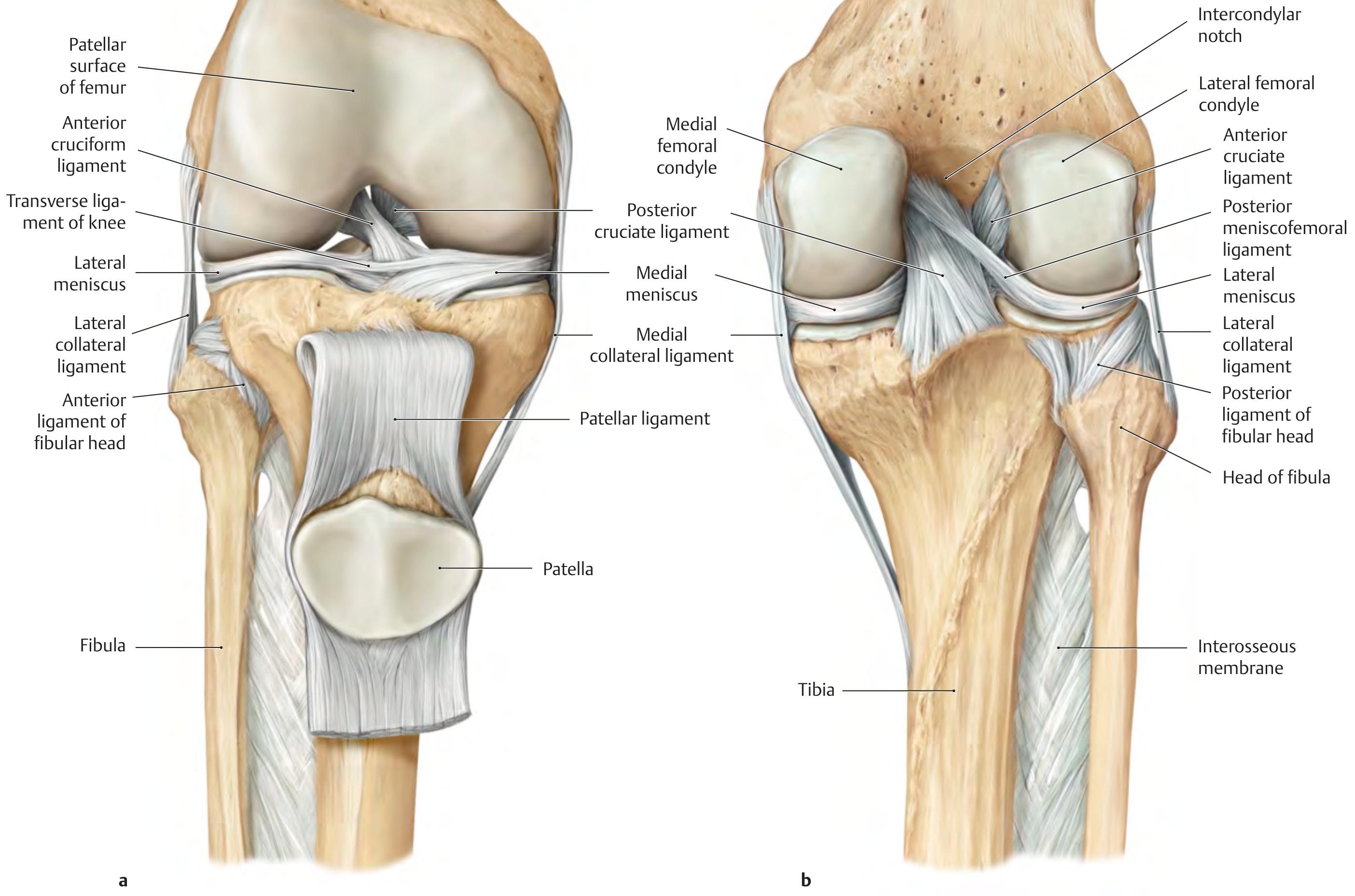
3. Menisci
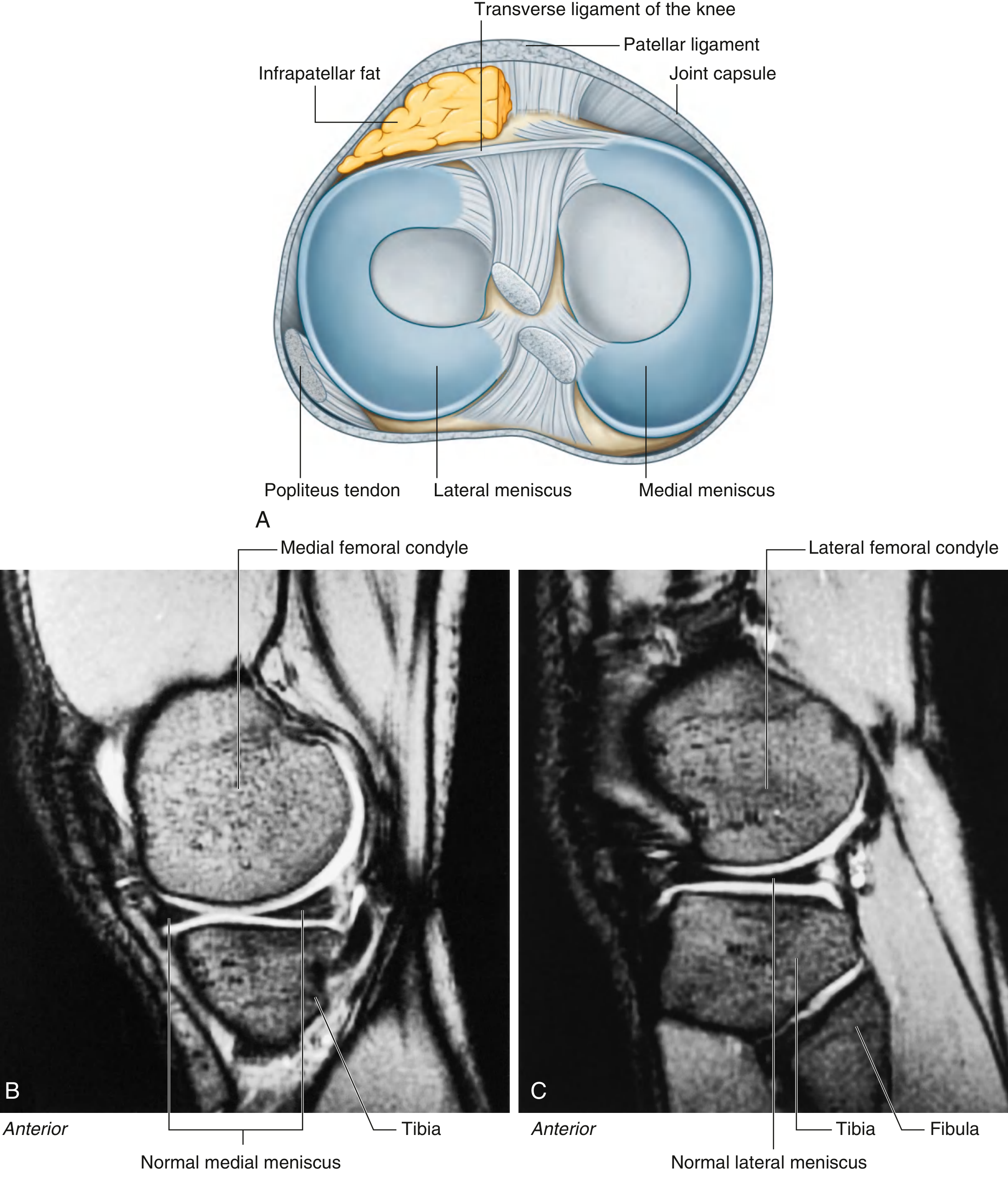
Two C-shaped fibrocartilaginous discs lie between the femoral and tibial condyles. They improve congruency, distribute load, act as shock absorbers, and assist in lubrication.
| Feature | Medial Meniscus | Lateral Meniscus |
|---|---|---|
| Shape | C-shaped (larger, wider posteriorly) | Nearly circular (O-shaped) |
| Attachment | Firmly attached to joint capsule and tibial (medial) collateral ligament | Not attached to capsule or LCL; connected to popliteus tendon |
| Mobility | Less mobile | More mobile |
| Injury risk | Higher (less mobile - commonly torn) | Lower |
The two menisci are connected anteriorly by the transverse ligament of the knee. The lateral meniscus is also connected posteriorly to the femur by the posterior meniscofemoral ligament (ligament of Wrisberg).
4. Articular Capsule
A wide, loose fibrous sleeve encloses the entire joint. Notable features:
- Anteriorly: Deficient in midline, replaced by the patella and patellar ligament. Reinforced by the quadriceps expansion and patellar retinacula.
- Posteriorly: Reinforced by the oblique popliteal ligament (expansion of semimembranosus) and arcuate popliteal ligament.
- The cruciate ligaments lie within the fibrous capsule but outside the synovial cavity (they are intracapsular but extrasynovial).
5. Ligaments
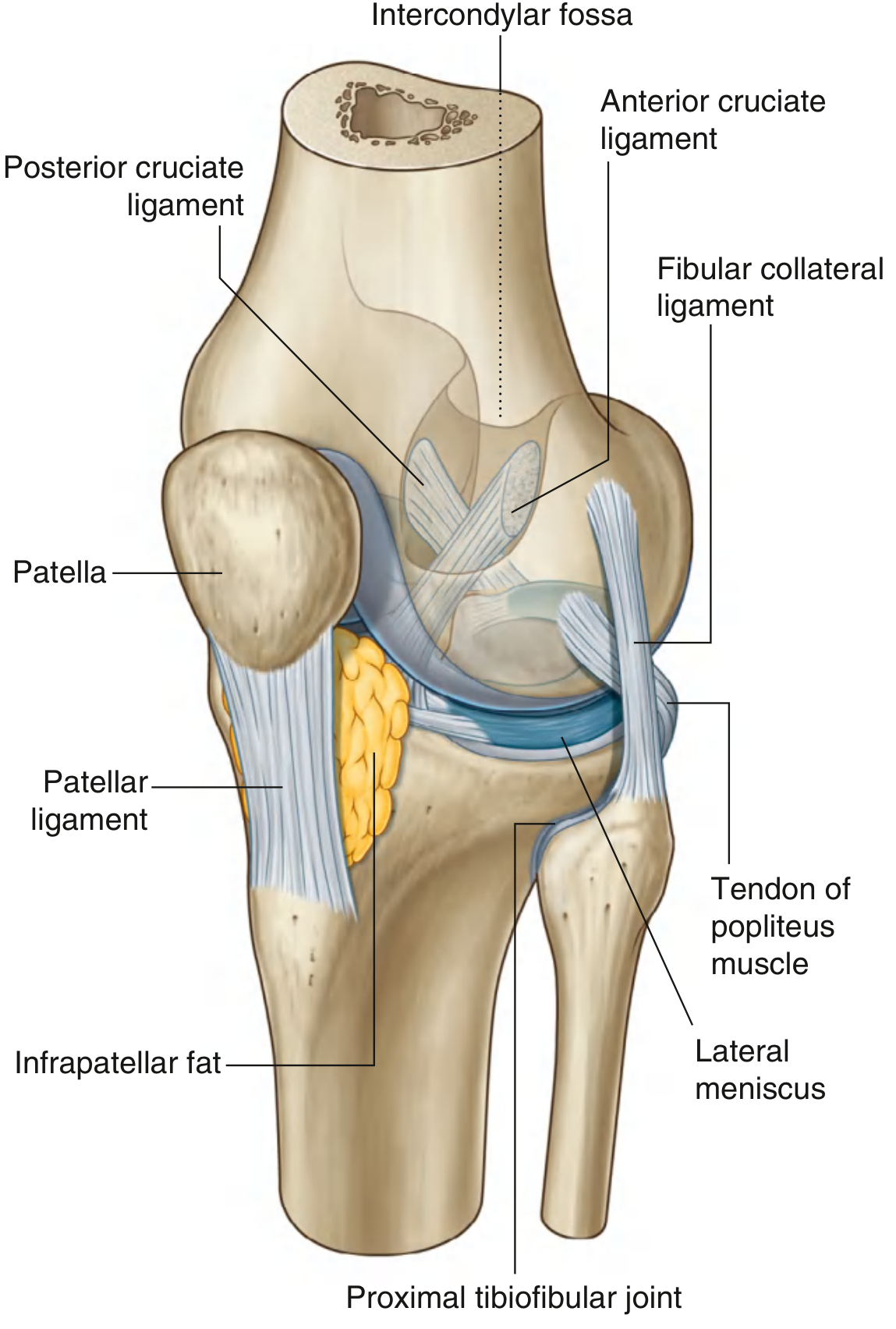
A. Cruciate Ligaments (Intrinsic - inside the capsule)
| Ligament | Tibial Attachment | Femoral Attachment | Function |
|---|---|---|---|
| ACL (Anterior Cruciate) | Anterior intercondylar area | Medial surface of lateral femoral condyle (posterior intercondylar notch) | Prevents anterior displacement of tibia on femur; limits hyperextension |
| PCL (Posterior Cruciate) | Posterior intercondylar area | Lateral surface of medial femoral condyle | Prevents posterior displacement of tibia; stronger and thicker than ACL |
The cruciate ligaments cross each other (ACL runs superoposterolaterally; PCL runs superoanteromedialy). Some fibres are taut in every position of the joint, ensuring constant stability in the sagittal plane.
B. Collateral Ligaments (Extrinsic)
| Ligament | Origin | Insertion | Function |
|---|---|---|---|
| MCL (Tibial collateral) | Medial femoral epicondyle | Medial surface of upper tibia (~7-8 cm below tibial plateau) | Resists valgus stress; stabilises in coronal plane |
| LCL (Fibular collateral) | Lateral femoral epicondyle | Head of fibula | Resists varus stress |
Both collateral ligaments are taut in extension and lax in flexion. The MCL is attached to the medial meniscus (explaining why MCL injuries often co-involve the medial meniscus).
C. Patellar Ligament
The continuation of the quadriceps tendon from the apex of the patella to the tibial tuberosity. The strongest ligament of the knee.
D. Other Ligaments
- Transverse ligament of knee: Connects the anterior horns of both menisci.
- Oblique popliteal ligament: Posterior capsule reinforcement.
- Arcuate popliteal ligament: Y-shaped, reinforces posterolateral capsule.
6. Synovial Membrane and Bursae
The synovial membrane is the largest and most complex in the body. It attaches to the articular margins and to the outer rims of the menisci. The cruciate ligaments are excluded from the synovial cavity (the synovial membrane reflects around them).
Key bursae:
| Bursa | Location | Communication with joint |
|---|---|---|
| Suprapatellar bursa | Between distal femur and quadriceps tendon | Always communicates (clinically an extension of the joint) |
| Prepatellar bursa (subcutaneous) | Over the patella | No |
| Infrapatellar bursa (deep) | Between patellar ligament and upper tibia | No |
| Infrapatellar bursa (subcutaneous) | Over tibial tuberosity | No |
| Popliteal (Baker's) cyst | Medial popliteal fossa - fusion of semimembranosus + gastrocnemius bursa | Secondary communication in disease states |
The articularis genus muscle (small slip of vastus intermedius) attaches to the suprapatellar bursa and pulls it superiorly during extension, preventing it from being pinched.
7. Movements and Muscles Responsible
| Movement | Range | Prime Movers |
|---|---|---|
| Flexion | 0-135° (active); 160° (passive) | Hamstrings (biceps femoris, semitendinosus, semimembranosus), gastrocnemius, popliteus, sartorius, gracilis |
| Extension | 0° (full extension) | Quadriceps femoris (rectus femoris, vastus medialis, lateralis, intermedius) |
| Medial rotation (tibia on femur, knee flexed) | ~10° | Popliteus, semitendinosus, semimembranosus, sartorius, gracilis |
| Lateral rotation (tibia on femur, knee flexed) | ~30° | Biceps femoris |
8. Locking Mechanism
When the knee reaches full extension during standing:
- The broad, flat inferior femoral condyle surfaces come into contact with the tibial plateau - maximising joint congruence.
- Because the medial femoral condyle has a longer articular surface, the femur undergoes medial rotation on the tibia during the last few degrees of extension.
- This tightens all ligaments (especially the collateral and cruciate ligaments), locking the joint in a "close-packed" position.
- This passive stability reduces quadriceps energy expenditure during prolonged standing.
Unlocking: The popliteus muscle initiates unlocking by rotating the femur laterally on the fixed tibia (or rotating the tibia medially on a fixed femur) - it is called the "key that unlocks the knee."
9. Blood Supply
The arterial supply is derived from a rich peripatellar and genicular anastomosis formed by:
- Femoral artery - descending genicular artery
- Popliteal artery - 5 genicular branches (superior medial, superior lateral, middle, inferior medial, inferior lateral genicular arteries)
- Anterior tibial artery - anterior tibial recurrent artery
- Lateral circumflex femoral artery - descending branch
- Circumflex fibular artery
10. Nerve Supply
Following Hilton's law (nerves supplying muscles that cross a joint also supply the joint):
| Nerve | Origin | Region supplied |
|---|---|---|
| Femoral nerve | L2-L4 | Anterior and medial capsule (via branches to vastus muscles) |
| Obturator nerve | L2-L4 | Medial capsule (posterior branch) |
| Common peroneal (fibular) nerve | L4-S2 | Lateral and posterolateral capsule |
| Tibial nerve | L4-S3 | Posterior capsule |
| Saphenous nerve | L3-L4 (femoral branch) | Medial and anteromedial capsule |
11. Clinical Correlations
a) ACL injury:
- Most common serious knee ligament injury, especially in sports involving pivoting/cutting.
- Positive anterior drawer test and Lachman test. MRI is the investigation of choice.
- Managed arthroscopically with patellar tendon or hamstring graft reconstruction.
b) "Unhappy triad" (O'Donoghue's triad):
- Simultaneous injury to the ACL + MCL + medial meniscus following a valgus force with external rotation (e.g., tackled from the side in football).
c) Meniscal tears:
- Medial meniscus is more commonly injured due to its firm capsular attachment limiting mobility.
- Patterns: vertical, horizontal, or bucket-handle tear (longitudinal tear where the inner fragment displaces into the intercondylar notch, causing locking).
- MRI is the modality of choice; arthroscopic repair/meniscectomy for treatment.
d) PCL injury:
- "Dashboard injury" - posterior force on the proximal tibia with the knee flexed (e.g., car accident). Positive posterior drawer test.
e) Baker's cyst (Popliteal cyst):
- A synovial-fluid-filled cyst in the medial popliteal fossa, often secondary to rheumatoid arthritis or osteoarthritis. Formed by fusion of the semimembranosus and gastrocnemius bursae, which communicates with the joint under elevated intra-articular pressure.
f) Prepatellar bursitis ("Housemaid's knee"):
- Inflammation of the subcutaneous prepatellar bursa from repeated kneeling (e.g., carpet layers, domestic workers).
Sources: Gray's Anatomy for Students, pp. 709-716; General Anatomy and Musculoskeletal System - THIEME Atlas of Anatomy, pp. 462-466; Tintinalli's Emergency Medicine; S Das: A Manual on Clinical Surgery, 13th ed.
This is a shared conversation. Sign in to Orris to start your own chat.