Abdominal pain with diarrhea 6 episodes/day for 2 days
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"acute diarrhea" AND "management" AND "adult"
Finding Sources
Searching PubMed
"acute diarrhea" AND treatment
Reading File
Reading File
Reading Article
PMID: 35839362
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive data. Let me compile the full management response.
Acute Diarrhea - Adult Management Approach
6 episodes/day for 2 days = acute diarrhea (onset <14 days). At this frequency, this is moderate-to-severe in volume but needs clinical stratification before acting.
Step 1 - Assess Severity and Red Flags
Concerning features that change management:
| Feature | Implication |
|---|---|
| Bloody or mucoid stool | Suggests invasive/inflammatory pathogen - avoid loperamide, consider antibiotics |
| Fever >38.5°C | Inflammatory diarrhea; stool cultures warranted |
| Signs of dehydration (orthostasis, decreased urine output, dry mucosae) | IV fluids may be needed |
| Severe abdominal pain | Consider surgical cause, C. diff, ischemic colitis |
| Diarrhea >7 days without improvement | Broadens differential (parasitic, IBD) |
| Recent antibiotics (<8 weeks) | C. difficile must be excluded |
| Recent travel (especially to endemic areas) | Travelers' diarrhea, parasites |
| Immunocompromised | Aggressive workup warranted |
If none of these are present, the most likely cause is viral gastroenteritis (norovirus #1 in the US), which is self-limited and requires only supportive care.
Step 2 - Investigations (Selective, Not Routine)
For uncomplicated watery diarrhea in a healthy adult with no red flags - no testing needed. Only 2-15% of stool bacterial cultures are positive, and results rarely change management in self-limited illness. - Symptom to Diagnosis, 4th Ed.
Test when:
- Bloody/mucoid stool, or fever >38.5°C
- Symptoms >7 days without improvement
- Severe dehydration or systemic signs of sepsis
- Recent antibiotic use (send C. diff PCR/toxin)
- Immunocompromised patient
- Outbreak setting or public health concern
Preferred tests:
- Multiplex molecular stool panel (PCR) - preferred over traditional cultures; higher sensitivity, faster turnaround
- C. diff toxin/PCR if antibiotic-associated
- Stool for ova and parasites if travel history or symptoms >7 days
Step 3 - Rehydration (First-Line for All)
Oral rehydration is the foundation of treatment and works because the sodium-coupled glucose transport mechanism in the small bowel typically remains intact even during acute infectious diarrhea.
Mild dehydration: Sports drinks, electrolyte drinks, soup broth are acceptable.
Moderate-to-significant dehydration: Use a balanced oral rehydration solution (ORS):
| Component | WHO ORS Composition |
|---|---|
| Sodium | 75 mmol/L |
| Glucose | 75 mmol/L |
| Potassium | 20 mmol/L |
| Chloride | 65 mmol/L |
| Citrate | 10 mmol/L |
Home ORS recipe (1 L clean water): ½ tsp salt + ¼ tsp baking soda + 8 tsp sugar. - Symptom to Diagnosis, 4th Ed.; Goldman-Cecil Medicine
IV fluids (Lactated Ringer's or normal saline) are reserved for:
- Inability to tolerate oral intake
- Severe dehydration
- Signs of sepsis
Step 4 - Symptomatic Agents
Loperamide (Imodium):
- 4 mg loading dose, then 2 mg after each unformed stool, max 16 mg/day
- Safe and effective for watery, nonbloody diarrhea without fever
- Avoid if: bloody stool, fever, suspected C. difficile - risk of toxic megacolon, prolonged fever, hemolytic uremic syndrome (with STEC)
Bismuth subsalicylate (Pepto-Bismol):
- 524 mg every 30-60 min as needed, up to 8 doses/day
- Reduces stool frequency and nausea; avoid if aspirin-sensitive
Diet:
-
BRAT diet (banana, rice, applesauce, toast) is commonly recommended
-
Avoid dairy temporarily (transient lactase deficiency post-viral illness)
-
Resume normal diet as tolerated; prolonged fasting is not beneficial
-
Goldman-Cecil Medicine, Table 26-5; Symptom to Diagnosis, 4th Ed.
Step 5 - Antibiotics (Rarely Indicated for Acute Diarrhea)
Empiric antibiotics are NOT recommended for most cases of acute community-acquired watery diarrhea in healthy adults. They do not shorten illness in viral gastroenteritis (the most common cause) and increase C. diff risk.
Consider antibiotics when:
| Indication | Preferred Regimen |
|---|---|
| Suspected sepsis | Empiric broad-spectrum (IV) |
| Travelers' diarrhea (moderate-severe) | Azithromycin 1 g PO x1 (preferred); Rifaximin 200 mg TID x3 days (non-invasive, no fever); Ciprofloxacin 500 mg q12h x3 days (increasing resistance) |
| Confirmed Shigella | Azithromycin or ciprofloxacin x3-5 days |
| Confirmed Campylobacter (severe) | Azithromycin 500 mg/day x3 days |
| Confirmed C. difficile | Fidaxomicin 200 mg BID x10 days (preferred) or oral vancomycin 125 mg QID x10 days |
| Confirmed Giardia | Metronidazole 250 mg TID x5-7 days |
Avoid antibiotics entirely for:
-
STEC (E. coli O157:H7) - associated with increased risk of hemolytic uremic syndrome
-
Uncomplicated Salmonella (non-typhoidal) in immunocompetent adults
-
Goldman-Cecil Medicine, Table 26-5; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine
Step 6 - When to Reassess or Refer
- Diarrhea persisting >7 days without improvement
- New development of bloody stool, fever, or worsening dehydration
- Inability to maintain oral hydration
- Elderly patients or those with significant comorbidities deteriorating
Summary Algorithm
Acute watery diarrhea x2 days, 6 episodes/day, healthy adult
|
Red flags? (blood, fever, recent antibiotics, travel, immunocompromised)
/ \
YES NO
| |
Stool testing Clinical diagnosis (viral gastroenteritis)
Targeted Rx Supportive care only:
- ORS / oral fluids
- Loperamide if watery/non-bloody
- BRAT diet, avoid dairy
- Reassess if >7 days
Key point from current literature (Am Fam Physician 2022, PMID 35839362): Antidiarrheal agents like loperamide are underused and can reduce inappropriate antibiotic prescribing - they are safe in non-inflammatory, non-bloody acute diarrhea in adults and help avoid unnecessary antimicrobial exposure.
Treatment for cracked soles
Finding Sources
Searching PubMed
"heel fissures" OR "cracked heels" treatment
Finding Sources
Reading Article
PMID: 34090765
Searching the Web
cracked heels heel fissures treatment urea emollients clinical management
Finding Sources
Reading Web Page
https://www.austinpublishinggroup.com/dermatology/fulltext/a…
I have solid evidence to give a thorough answer. Here it is:
Treatment for Cracked Soles (Heel Fissures)
Cracked soles result from excessive xerosis (dryness) causing the thickened stratum corneum to lose elasticity and split. The key drivers are mechanical pressure on the heel fat pad, reduced skin moisture, and callus buildup. Treatment is graded by severity.
Classify Severity First
| Grade | Description | Management Level |
|---|---|---|
| Grade I (Superficial) | Dry, flaking skin; no visible crack depth | OTC emollients + exfoliation |
| Grade II (Moderate) | Partial-thickness fissures into dermis; pain on walking | Keratolytics + occlusion |
| Grade III (Severe) | Full-thickness splits; bleeding, infection risk | Wound care + possible procedural treatment |
Grade I - Superficial Fissures
1. Moisturize daily (the cornerstone)
- Apply a thick emollient twice daily - after bathing is optimal when skin is still slightly damp
- Best OTC options: Eucerin, Cetaphil, CeraVe Healing Ointment, petroleum jelly (Vaseline)
- Occlusives (petrolatum-based) are more effective than thin lotions for very dry skin
2. Urea-based creams - first-line keratolytic
- Urea works via two mechanisms: humectant (draws water into the stratum corneum) + keratolytic (breaks hydrogen bonds in hardened keratin)
- For Grade I: 10-15% urea cream, applied twice daily
- An RCT (J Tissue Viability 2021, PMID 34090765) confirmed 20% urea cream significantly outperforms placebo for plantar skin hydration - visible softening typically within 3-7 days at 20-25%
3. Gentle exfoliation
- Pumice stone or foot file used on wet skin (after soaking) 1-2x/week
- Removes hyperkeratotic buildup that prevents emollients from penetrating
- Do not file dry skin - always wet first
4. Foot soaks
- Warm water soak for 10-15 min before exfoliation softens the callus
- Avoid prolonged soaking (>20 min) which paradoxically dries skin by disrupting the barrier
Grade II - Moderate Fissures
Higher-concentration urea or alpha-hydroxy acids:
| Agent | Concentration | Notes |
|---|---|---|
| Urea cream | 20-40% | Gold standard; 40% is prescription-strength; aggressive keratolysis for thick callus |
| Lactic acid / ammonium lactate | 5-12% | Comparable efficacy to urea; better cosmetic feel; use if urea causes irritation |
| Salicylic acid | 6-17% (in combination products) | Keratolytic; found in products like Kerasal; AMPA-approved for heel fissures |
| Urea + lactic acid combination | - | Synergistic - urea penetrates deep, lactic acid promotes surface turnover |
Occlusion technique (significantly boosts efficacy):
- Apply high-concentration urea cream at night, cover with cotton socks - the occlusion increases penetration depth substantially
- Known as "sock therapy" or "wet wrap"
Cyanoacrylate tissue adhesive (liquid bandage / skin glue):
- Effective for painful Grade II fissures that do not have signs of infection
- Fills the crack, reduces pain immediately, protects from mechanical stress during healing
- Applied once the crack is clean and dry; reapply as needed
Grade III - Severe/Bleeding Fissures
- Wound care: Clean with saline, apply antimicrobial dressing if infected
- Debridement: Podiatric or dermatology referral for safe removal of deep callus using a blade (do not attempt at home)
- Cyanoacrylate adhesive remains useful for pain relief and closure
- Topical timolol 0.5% gel - a case series (JAAD 2021, PMID 32479981) reported effective healing of deep painful heel fissures with topical timolol, thought to work via beta-receptor mediated keratinocyte proliferation (emerging evidence, off-label)
- If signs of infection (warmth, erythema, purulence): wound culture + topical or oral antibiotics depending on severity
Special Populations
Diabetic patients:
- Heel fissures are high-risk - can be a portal for serious foot infections
- Use 20-25% urea (not higher concentrations that may over-exfoliate fragile skin)
- Avoid blade debridement at home
- Regular podiatry review is essential
- An RCT in diabetic patients showed urea cream reduced deep open fissures from 24% to 6.4% at 4 weeks vs. placebo (p=0.002)
Elderly patients:
- More prone due to reduced sebaceous gland activity and skin thinning
- Regular moisturizing is preventive, not just therapeutic
Prevention
- Moisturize heels daily year-round
- Wear supportive, closed-heel footwear (open-backed shoes increase heel fat pad splaying and friction)
- Avoid prolonged standing on hard floors without cushioned footwear
- Stay hydrated
- Manage underlying conditions: hypothyroidism, diabetes, psoriasis, eczema - all increase heel fissure risk
When to Refer (Podiatry or Dermatology)
- Grade III fissures with bleeding or signs of infection
- Diabetic foot with any fissure
- No improvement after 4 weeks of consistent topical therapy
- Underlying skin disorder suspected (psoriasis, palmoplantar keratoderma, tinea pedis)
What to look for ESR and CRP in fevee
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive, textbook-sourced data. Here is the full answer:
ESR and CRP in Fever - What to Look For
Both are acute-phase reactants - non-specific markers of systemic inflammation. Neither diagnoses a cause, but their magnitude, pattern, and combination help narrow the differential and guide workup.
Understanding the Two Tests
| Feature | ESR | CRP |
|---|---|---|
| What it measures | Rate of fall of RBCs in 1 hour - indirect reflection of fibrinogen, globulins | Single acute-phase protein synthesized by hepatocytes |
| Normal | Men: age ÷ 2 mm/h; Women: (age + 10) ÷ 2 mm/h | <0.3 mg/dL (most healthy adults) |
| Rise after stimulus | Slow - peaks over days to weeks | Rapid - rises within 6-12 hours, peaks at 2-3 days |
| Fall after resolution | Slow (weeks) | Rapid - half-life ~19 hours; clears fast when inflammation resolves |
| Age/sex effect | Higher in women and elderly | Not significantly affected by age or sex |
| Precision | Lower - affected by many variables | Higher - precise, reproducible, measurable on stored sera |
- Firestein & Kelley's Textbook of Rheumatology
ESR Reference Ranges and What Elevation Means
Normal formula (Westergren):
- Men: age ÷ 2 mm/h
- Women: (age + 10) ÷ 2 mm/h
Factors that falsely elevate ESR (not inflammation): anemia, macrocytosis, pregnancy (2nd/3rd trimester), female sex, advanced age, hypoalbuminemia, high room temperature, tilted tube.
Factors that falsely lower ESR: polycythemia, microcytosis, sickle cell disease, spherocytosis, extreme leukocytosis.
| ESR Level | Interpretation in Fever |
|---|---|
| Mildly elevated (up to ~40 mm/h) | Often non-specific; viral illness, minor inflammation |
| Moderately elevated (40-70 mm/h) | Warrants workup; infection, autoimmune, malignancy possible |
| Markedly elevated (>100 mm/h) | Strongly suggests serious disease - bacterial infection, temporal arteritis/PMR, malignancy (multiple myeloma, lymphoma), or major autoimmune disease |
Key point: An ESR >100 mm/h almost always has an identifiable serious cause - the underlying diagnosis is usually apparent from history and physical, especially at extreme levels. If no cause is found, repeat in months rather than initiating a blind workup. - Textbook of Family Medicine, 9e
Specific use of ESR:
- Best validated for polymyalgia rheumatica and temporal arteritis: 90% of biopsy-proven cases have ESR >30 mm/h (mean ~90 mm/h). A normal ESR does not rule it out - ~4% of cases have normal ESR.
- Monitoring treatment response in PMR/temporal arteritis (falls within days of corticosteroids)
CRP Reference Ranges and What Elevation Means
Normal: <0.3 mg/dL. Clinically significant elevation: >1 mg/dL.
| CRP Level | Clinical Interpretation |
|---|---|
| <1 mg/dL (minor/normal) | Vigorous exercise, common cold, pregnancy, gingivitis, obesity, depression, insulin resistance |
| 1-10 mg/dL (moderate) | Myocardial infarction, malignancies, pancreatitis, mucosal infections (bronchitis, cystitis), most systemic autoimmune diseases (RA, IBD) |
| >10 mg/dL (marked) | Acute bacterial infection (80-85% of cases), major trauma, systemic vasculitis |
| >15 mg/dL | Strongly suggests bacterial infection |
| >50 mg/dL | Infection present in 88% of cases |
Critical rule: CRP >10 mg/dL = bacterial infection until proven otherwise. - Firestein & Kelley's Rheumatology
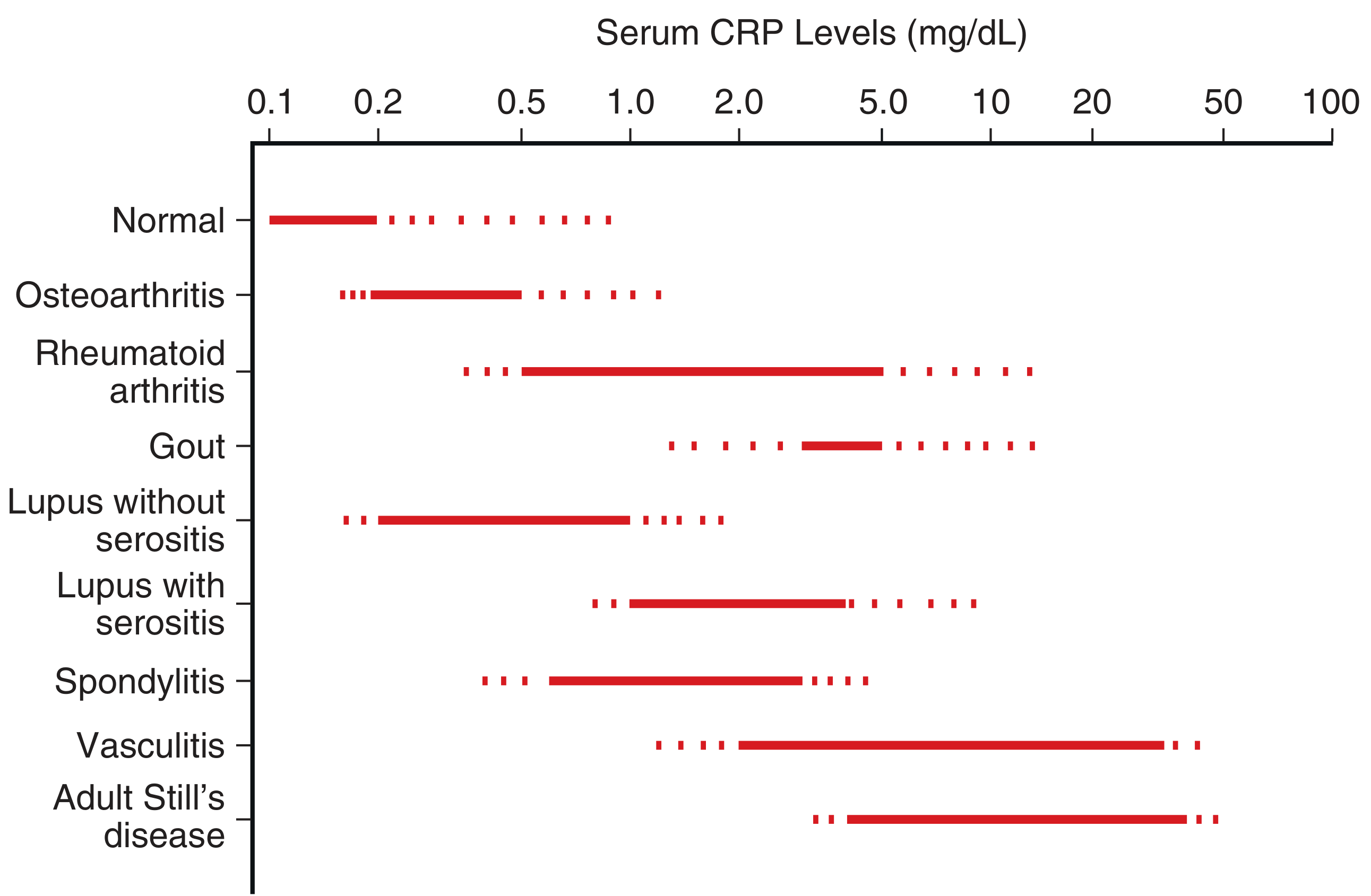
Note on SLE (Lupus): CRP is characteristically low or only mildly elevated despite active lupus flare - this is a classic exam and clinical pearl. A high CRP in a lupus patient with fever should raise suspicion for superimposed infection, not lupus activity.
CRP Range Across Conditions
How to Use Them Together in Fever
CRP is more useful than ESR for acute fever because it rises and falls much faster - it reflects the current inflammatory state, not a lagging picture.
| Clinical scenario | What to expect |
|---|---|
| Viral fever | ESR mildly elevated, CRP low-to-moderate (<5 mg/dL) |
| Bacterial infection | CRP markedly elevated (>10 mg/dL), ESR also elevated but lags |
| Autoimmune flare (RA, vasculitis) | Both elevated; CRP 1-10+ mg/dL depending on disease |
| Lupus flare | ESR elevated, CRP normal or only mildly elevated |
| Malignancy (lymphoma, myeloma) | ESR markedly elevated; CRP variable |
| Resolving infection on antibiotics | CRP falls first (half-life 19h); ESR may stay elevated for weeks |
Procalcitonin (PCT) - A Better Bacterial Marker
When you specifically need to distinguish bacterial vs. viral/non-infectious fever, PCT outperforms both ESR and CRP:
-
Normal PCT: <0.1 ng/mL
-
Bacterial sepsis: can rise to >100 ng/mL
-
PCT is not elevated in viral illness or non-infectious inflammatory states (unlike CRP which rises in both)
-
Particularly useful for: antibiotic stewardship (guide duration), sepsis monitoring, differentiating bacterial from viral pneumonia
-
Firestein & Kelley's Textbook of Rheumatology
Practical Summary
- Use CRP when you want a real-time inflammatory marker in acute fever - responds within hours, clears fast
- Use ESR when monitoring chronic conditions (PMR, temporal arteritis, TB response)
- CRP >10 mg/dL = strong pointer to bacterial infection
- ESR >100 mm/h = serious underlying disease (infection, vasculitis, myeloma)
- High ESR + low CRP in febrile patient = think SLE or viral illness
- Both normal = makes significant bacterial infection unlikely but does not exclude it
- Neither test replaces clinical judgment - always interpret alongside history, exam, and targeted investigations
This is a shared conversation. Sign in to Orris to start your own chat.